You might also like
- 2009, Krassioucov, A Systematic Review of The Management of Autonomic Dysreflexia After Spinal Cord InjuryDocument14 pages2009, Krassioucov, A Systematic Review of The Management of Autonomic Dysreflexia After Spinal Cord InjuryISLinkNo ratings yet
- Guidelines, DysreflexiacpgDocument40 pagesGuidelines, DysreflexiacpgISLinkNo ratings yet
- Concise Chronic Spinal Cord Injury 2008Document15 pagesConcise Chronic Spinal Cord Injury 2008ISLinkNo ratings yet
- Rehab Phase After Acute SCIDocument9 pagesRehab Phase After Acute SCIISLinkNo ratings yet
- Neurogenic Bladder in SCIDocument111 pagesNeurogenic Bladder in SCIISLinkNo ratings yet
- 2009, Patients and Caregivers Knowledge For ADDocument6 pages2009, Patients and Caregivers Knowledge For ADISLinkNo ratings yet
- Tetraplegia Hand Activity QuestionnaireDocument20 pagesTetraplegia Hand Activity QuestionnaireISLinkNo ratings yet
- Neuromodulation SCIDocument14 pagesNeuromodulation SCIISLinkNo ratings yet
- Restore - Funtion in SCI PatientsDocument15 pagesRestore - Funtion in SCI PatientsISLinkNo ratings yet
- Acute and Chronic Management of Spinal Cord InjuryDocument16 pagesAcute and Chronic Management of Spinal Cord InjuryISLinkNo ratings yet
- Urinary 2Document28 pagesUrinary 2ISLinkNo ratings yet
- MS Neurogenic BladderDocument11 pagesMS Neurogenic BladderISLinkNo ratings yet
- 2012 Guidelines Large Text Print Total FileDocument1,600 pages2012 Guidelines Large Text Print Total FileISLinkNo ratings yet
- Clare Fowler - PPT!!!!Document58 pagesClare Fowler - PPT!!!!ISLinkNo ratings yet
- French Guide Lines MS Bladder!!!!Ful ArticleDocument15 pagesFrench Guide Lines MS Bladder!!!!Ful ArticleISLinkNo ratings yet
- Consensus StatementDocument18 pagesConsensus StatementISLinkNo ratings yet
- Urinary Dysfunction and Multiple SclerosisDocument44 pagesUrinary Dysfunction and Multiple SclerosisMac Perez LopezNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5783)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (72)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Japanese Water TherapyDocument3 pagesJapanese Water TherapyJun DangoyNo ratings yet
- ABBREVIATIONS ACRONYMS AND SYMBOLS COMMONLY USED FACULTY Revised 2015 PDFDocument4 pagesABBREVIATIONS ACRONYMS AND SYMBOLS COMMONLY USED FACULTY Revised 2015 PDFishang14No ratings yet
- Medmicronotes 3Document66 pagesMedmicronotes 3Lethal BaconNo ratings yet
- Daftar PustakaDocument4 pagesDaftar PustakaDPMF FK UNPATTINo ratings yet
- Health Assessment SAS Session 17Document5 pagesHealth Assessment SAS Session 17pw49cbqxnfNo ratings yet
- CBI Procedure Guide for NursesDocument9 pagesCBI Procedure Guide for NursesAlvin OccianoNo ratings yet
- Urinary Tract Infection Risk FactorsDocument20 pagesUrinary Tract Infection Risk FactorsAnas Mk HindawiNo ratings yet
- Cranberry LaunchDocument11 pagesCranberry LaunchShouvik Das100% (1)
- Urology HX and ExamDocument31 pagesUrology HX and ExamMisbah KaleemNo ratings yet
- Oleos e Óleos Essenciais (71-80)Document10 pagesOleos e Óleos Essenciais (71-80)monise motaNo ratings yet
- Medical History FormatDocument5 pagesMedical History Formatkrzia TehNo ratings yet
- Clinical: MCQ TestDocument47 pagesClinical: MCQ TestAhmed AlrkabeNo ratings yet
- Possible Interview Questions For NursesDocument32 pagesPossible Interview Questions For NursesElisabeta Ivan75% (4)
- Urology PDFDocument24 pagesUrology PDFzzNo ratings yet
- N120 Final Review PDFDocument7 pagesN120 Final Review PDFsutopianoNo ratings yet
- Puerperal Pyrexia 2Document7 pagesPuerperal Pyrexia 2dyah ayu noer fadilaNo ratings yet
- Microbiology Unknown ReportDocument25 pagesMicrobiology Unknown Reportacj56100% (1)
- The Nursing Shortage and Its Effect On Patient CareDocument7 pagesThe Nursing Shortage and Its Effect On Patient Careapi-641842901No ratings yet
- CBA 8 MCQ Compilation 2020Document20 pagesCBA 8 MCQ Compilation 2020Sadia YousafNo ratings yet
- Bag Technique and Urine TestDocument19 pagesBag Technique and Urine TestBenz Jim Gragasin100% (1)
- All BacteriaDocument14 pagesAll Bacteriamorale28100% (2)
- Efficacy of Styplon Vet Bolus for Hemorrhagic ConditionsDocument2 pagesEfficacy of Styplon Vet Bolus for Hemorrhagic ConditionsKishan PatelNo ratings yet
- Manual of Antimicrobial Susceptibility TestingDocument241 pagesManual of Antimicrobial Susceptibility TestingEndale Balcha100% (4)
- Clean Intermittent Catheterization Techniques and BenefitsDocument2 pagesClean Intermittent Catheterization Techniques and BenefitsSri HariNo ratings yet
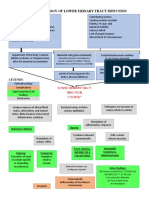
- Pathophysiology of Lower Urinary Tract InfectionDocument1 pagePathophysiology of Lower Urinary Tract InfectionSTORAGE FILENo ratings yet
- Research-Evaluating Children's Health and DevelopmentDocument4 pagesResearch-Evaluating Children's Health and Developmentdenyl ramosNo ratings yet
- Asynchronous Activity Day 2 Dinson, Red Angela O. BSN 2-BDocument11 pagesAsynchronous Activity Day 2 Dinson, Red Angela O. BSN 2-BRed Angela DinsonNo ratings yet
- Pylonephritis 130520160226 Phpapp02Document17 pagesPylonephritis 130520160226 Phpapp02Elena-Dana OpreaNo ratings yet
- Cantellops, N Soap Note #4 02.25.20Document3 pagesCantellops, N Soap Note #4 02.25.20Nicole Juliette CCNo ratings yet
- Gallium ApaDocument3 pagesGallium Apavedha mungaraNo ratings yet