You might also like
- Quick Study Weights & Measures PDFDocument4 pagesQuick Study Weights & Measures PDFheysemberg100% (6)
- Study Nervous SystemDocument2 pagesStudy Nervous SystemIoana Temeliescu Ex Zamfir100% (4)
- (Dale Nibbe) Brain Reference Guide PDFDocument2 pages(Dale Nibbe) Brain Reference Guide PDFSuryakantaRoulTuntun100% (4)
- QuickStudy - The HeartDocument2 pagesQuickStudy - The HeartAbc Abc100% (5)
- Tips - Barcharts Quickstudy Psychology PDFDocument4 pagesTips - Barcharts Quickstudy Psychology PDFsmacuja100% (1)
- QuickStudy - Lymphatic SystemDocument2 pagesQuickStudy - Lymphatic SystemEmina Borovac100% (2)
- BarCharts QuickStudy Business Facts PDFDocument4 pagesBarCharts QuickStudy Business Facts PDF220479100% (1)
- Muscular System (Quick Study Academic) - Inc. BarChartsDocument4 pagesMuscular System (Quick Study Academic) - Inc. BarChartskogawobu0% (2)
- QuickStudy FinanceDocument4 pagesQuickStudy FinanceAnge William Kouadio100% (1)
- Biochemical Periodic Table: Key Elements in The BodyDocument6 pagesBiochemical Periodic Table: Key Elements in The BodyEline Moyo100% (1)
- Calculus Reference (SparkCharts)Document2 pagesCalculus Reference (SparkCharts)www_webb100% (1)
- Hundreds of Titles At: Word/Phrase Replace WithDocument1 pageHundreds of Titles At: Word/Phrase Replace WithenriNo ratings yet
- The Sparkcharts Algebra IDocument4 pagesThe Sparkcharts Algebra IMuhammad Fariz Mohamed Zain88% (8)
- Chemistry Equations Answers QuickstudyDocument6 pagesChemistry Equations Answers QuickstudyRafael Ramos100% (6)
- Review ChartDocument6 pagesReview Chartapi-238667529100% (1)
- Chemistry - Periodic Table - Advanced PDFDocument2 pagesChemistry - Periodic Table - Advanced PDFCA_Ken86% (7)
- Anatomy of The Senses QuickStudy Reference Guide - (HEARING)Document2 pagesAnatomy of The Senses QuickStudy Reference Guide - (HEARING)statsoNo ratings yet
- BarCharts QuickStudy Anatomy Vol 2 PDFDocument6 pagesBarCharts QuickStudy Anatomy Vol 2 PDFRichard Harrow100% (7)
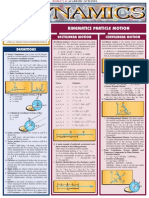
- Dynamics - Quick Reference SheetDocument4 pagesDynamics - Quick Reference Sheetmech118No ratings yet
- Nursing School Necessities Cheat SheetDocument3 pagesNursing School Necessities Cheat SheetRevNo ratings yet
- Comprehensive overview of basic mathematical conceptsDocument4 pagesComprehensive overview of basic mathematical conceptsalberthawking100% (8)
- Quick Study Academic Physics 600dpiDocument6 pagesQuick Study Academic Physics 600dpiSunshineK95100% (8)
- Barchart (Calculus 1)Document6 pagesBarchart (Calculus 1)Kevin McGuire100% (1)
- (Quickstudy - Academic) Inc. BarCharts - Geometric Formulas-QuickStudy (2005)Document6 pages(Quickstudy - Academic) Inc. BarCharts - Geometric Formulas-QuickStudy (2005)Dany el100% (2)
- Emt - Emergency Medical Technician (Quick Study Academic) - Inc. BarChartsDocument4 pagesEmt - Emergency Medical Technician (Quick Study Academic) - Inc. BarChartsgoticifa0% (2)
- QuickStudy Biology PDFDocument4 pagesQuickStudy Biology PDFmed1978100% (8)
- BarCharts QuickStudy Reproductive SystemDocument2 pagesBarCharts QuickStudy Reproductive SystemRUDY792100% (4)
- Venous System Arterial System: A. Artery A.A. Arteries L. Left R. Right v. Vein V.V. VeinsDocument2 pagesVenous System Arterial System: A. Artery A.A. Arteries L. Left R. Right v. Vein V.V. VeinsJann ericka Jao100% (2)
- (Quickstudy Reference Guides - Academic) Mark Jackson - Chemistry Lab Basics-Barcharts (2002) PDFDocument2 pages(Quickstudy Reference Guides - Academic) Mark Jackson - Chemistry Lab Basics-Barcharts (2002) PDFLouis Nguyen100% (4)
- Microbiology - (Beneficial or Pathogenic) PDFDocument1 pageMicrobiology - (Beneficial or Pathogenic) PDFanaNo ratings yet
- Literary Terms 1spark Charts1Document6 pagesLiterary Terms 1spark Charts12ygbk7100% (2)
- Lymphatic SystemDocument2 pagesLymphatic SystemDN NLL100% (1)
- Periodic Table Basic, 2nd EditionDocument2 pagesPeriodic Table Basic, 2nd EditionMaki MajomNo ratings yet
- Dental Anatomy Reference Guide - (Malestrom)Document2 pagesDental Anatomy Reference Guide - (Malestrom)ronaldricardo_ladiesman01100% (1)
- Cardiac Study GuideDocument11 pagesCardiac Study Guidesurviving nursing school100% (2)
- QuickStudy Resumes & Interviews PDFDocument4 pagesQuickStudy Resumes & Interviews PDFJohn100% (3)
- Fiches AnatomyDocument6 pagesFiches AnatomyAnas Ismail100% (2)
- Animal GKDocument4 pagesAnimal GKSARVEJAYA KRISHNANo ratings yet
- BarCharts QuickStudy Memorial DayDocument2 pagesBarCharts QuickStudy Memorial DayBrandon WangNo ratings yet
- Mnemonics For NursingDocument35 pagesMnemonics For Nursingbetterdenthat100% (1)
- The World The World: Canada CanadaDocument4 pagesThe World The World: Canada CanadaStipe KodzomanNo ratings yet
- Founder To Ceo - How To Build A Great Company - Matt MocharyDocument84 pagesFounder To Ceo - How To Build A Great Company - Matt MocharyPratiiek MorNo ratings yet
- Skillslab HandbookDocument25 pagesSkillslab HandbookJun Man0% (1)
- Fundamentals of Nursing NotesDocument34 pagesFundamentals of Nursing NotesKate Therese TaronNo ratings yet
- Pyrethrum Component of Chrysanthemum Plant As An Insecticide For PlantsDocument58 pagesPyrethrum Component of Chrysanthemum Plant As An Insecticide For PlantsKristine Cabal100% (5)
- GB Free Guide Apr 2023 Week 3Document17 pagesGB Free Guide Apr 2023 Week 3tala ismailNo ratings yet
- Fish ProcessingDocument9 pagesFish ProcessingKenkoi Sanchez100% (1)
- BAR OPERATIONS GUIDEDocument11 pagesBAR OPERATIONS GUIDERishabh ChawdaNo ratings yet
- Anatomy and Physiology Nursing Mnemonics TipsDocument8 pagesAnatomy and Physiology Nursing Mnemonics TipsariNo ratings yet
- Principles Underlying Medical and Surgical AsepsisDocument12 pagesPrinciples Underlying Medical and Surgical AsepsisKiyoteru Hiyama0% (1)
- Final Business PlanDocument35 pagesFinal Business Planjeanuel100% (1)
- ALHS 1090 Final Exam WorksheetDocument18 pagesALHS 1090 Final Exam WorksheetCesilia Martinez Castro0% (1)
- The Safire WoodDocument18 pagesThe Safire WoodPip TurenNo ratings yet
- Really Useful English GrammarDocument108 pagesReally Useful English GrammarYamchi Arnavaz0% (1)
- Preparing Vegetable Dishes: Sptve-Cookery Guided Learning Activity KitDocument14 pagesPreparing Vegetable Dishes: Sptve-Cookery Guided Learning Activity KitLucille PaglingayenNo ratings yet
- Infection ControlDocument58 pagesInfection ControlYoyen Gonzaga100% (10)
- Gestational Diabetes Case Study With Questions For The Undergraduate NurseDocument46 pagesGestational Diabetes Case Study With Questions For The Undergraduate NurseAndrea Donmyer100% (1)
- The Wolf by Philipp Meyer (The Iowa Review)Document14 pagesThe Wolf by Philipp Meyer (The Iowa Review)NouriNo ratings yet
- Spark Charts - NursingDocument4 pagesSpark Charts - Nursinggeminix92100% (1)
- Blood Vessels List HandoutDocument2 pagesBlood Vessels List HandoutSopheNo ratings yet
- Presentation Disaster NursingDocument25 pagesPresentation Disaster NursingShiehan Mae ForroNo ratings yet
- Patient Management Course ReviewDocument76 pagesPatient Management Course ReviewclaraNo ratings yet
- Common 1 (Infection Control)Document46 pagesCommon 1 (Infection Control)kristaNo ratings yet
- Asepsis and Infection Control ConceptsDocument76 pagesAsepsis and Infection Control ConceptsSirWin AmidNo ratings yet
- Asepsis and Infection ControlDocument46 pagesAsepsis and Infection ControlecocafephNo ratings yet
- Complete dentures: Structure and strategy of initial patient interviewDocument8 pagesComplete dentures: Structure and strategy of initial patient interviewjorefe12No ratings yet
- Introduction To Medical Surgical Nursing: Mr. Sandip Rangari Suretech College of NursingDocument21 pagesIntroduction To Medical Surgical Nursing: Mr. Sandip Rangari Suretech College of NursingSanket TelangNo ratings yet
- Basic Principles and Procedures of Infection Prevenetion and ControlDocument98 pagesBasic Principles and Procedures of Infection Prevenetion and Controlbasl.hazm34No ratings yet
- ASEPSIS: Preventing Infection Through Proper TechniquesDocument36 pagesASEPSIS: Preventing Infection Through Proper TechniquesChevelle Valenciano-GaanNo ratings yet
- Implement and Monitor Infection Control Policies and Procedure in CaregivingDocument91 pagesImplement and Monitor Infection Control Policies and Procedure in Caregivingjessica coronelNo ratings yet
- Ringkasan Eksekutif Luas Panen Dan Produksi Padi Di Indonesia 2019Document32 pagesRingkasan Eksekutif Luas Panen Dan Produksi Padi Di Indonesia 2019zulfaNo ratings yet
- Preliminary English TestDocument10 pagesPreliminary English TestMathuraa MathuNo ratings yet
- Nana 11 - Traditional Practices Assessment IV Elementary School SiteDocument127 pagesNana 11 - Traditional Practices Assessment IV Elementary School Siteapi-289052060No ratings yet
- Begin Goat Farming with DVBF's Profitable PackageDocument16 pagesBegin Goat Farming with DVBF's Profitable PackageGiacenNo ratings yet
- Determiners Both Either Neither Grammar Esl Exercises WorksheetDocument2 pagesDeterminers Both Either Neither Grammar Esl Exercises WorksheetMaría VallejoNo ratings yet
- Marketing Plan of Green Olive RestaurantDocument11 pagesMarketing Plan of Green Olive RestaurantMuhammad Sajid Saeed100% (1)
- Jungle SurvivalDocument14 pagesJungle SurvivalMuhammad Hijrahli RijaNo ratings yet
- BREI’s Blue Ridge Public School Monthly Activities July 2021Document2 pagesBREI’s Blue Ridge Public School Monthly Activities July 2021AnantNo ratings yet
- Micronutrients Status and Management in Orchards Soils Applied AspectsDocument11 pagesMicronutrients Status and Management in Orchards Soils Applied AspectsMuhammad AliNo ratings yet
- Delivery Man ScriptDocument14 pagesDelivery Man ScriptJayhze DizonNo ratings yet
- (Assignment - 1) Unit Operation in Food ProcessingDocument23 pages(Assignment - 1) Unit Operation in Food ProcessingHARINo ratings yet
- AGRICULTUREDocument8 pagesAGRICULTUREANKIT RAJNo ratings yet
- The Product Life Cycle of IceCreamDocument4 pagesThe Product Life Cycle of IceCreamClaudiuPascoviciNo ratings yet
- Sandpoint Residents - Sheet1Document2 pagesSandpoint Residents - Sheet1Joseph NietubiczNo ratings yet
- Sale Sep. 22Document3 pagesSale Sep. 22birpal singhNo ratings yet
- Proiect EnglezaDocument13 pagesProiect EnglezaPop OannaNo ratings yet
- Benguet TribeDocument18 pagesBenguet Tribejoey tugay-anNo ratings yet
- Physiological Functions and Metabolism of Essential Dietary Element IodineDocument4 pagesPhysiological Functions and Metabolism of Essential Dietary Element IodinefitrizeliaNo ratings yet
- Cold Sauces and Soups LessonDocument7 pagesCold Sauces and Soups LessonMary Annavic SalumbidesNo ratings yet