You might also like
- Cranial NervesDocument65 pagesCranial Nervessarguss14100% (13)
- Cranial Nerves Assessment GuideDocument8 pagesCranial Nerves Assessment GuideTrisha Najial AlmendraNo ratings yet
- Head To Toe AssessmentDocument18 pagesHead To Toe AssessmentCin Dy100% (2)
- Physical Assessment Guide of Head-To-ToeDocument9 pagesPhysical Assessment Guide of Head-To-Toeneleh gray100% (2)
- Cranial Nerves SummaryDocument3 pagesCranial Nerves SummaryJoash F. Pacquing75% (4)
- Cranial NervesDocument17 pagesCranial Nervesdankirsh100% (17)
- Performance Checklist On Cranial Nerve AssessmentDocument3 pagesPerformance Checklist On Cranial Nerve AssessmentSolsona Natl HS Maananteng100% (1)
- Cranial Nerve AssessmentDocument4 pagesCranial Nerve AssessmentAnonymous h2EnKyDbNo ratings yet
- Cranial Nerve ExaminationDocument19 pagesCranial Nerve ExaminationBhargavi SoodNo ratings yet
- Cranial NervesDocument9 pagesCranial Nervesangrypandasaredangerous100% (3)
- Head To Toe AssessmentDocument56 pagesHead To Toe AssessmentAna95% (39)
- Neurological AssessmentDocument3 pagesNeurological AssessmentGellian Placido100% (3)
- Neurological AssessmentDocument127 pagesNeurological Assessmentstudent_019100% (1)
- Sr. Herona Bute- Black D.O.N.E October 7th 2011Document35 pagesSr. Herona Bute- Black D.O.N.E October 7th 2011Jemicia AdamsNo ratings yet
- Cranial Nerve AssessmentDocument42 pagesCranial Nerve AssessmentValeryn Quiman100% (6)
- Eye AssessmentDocument123 pagesEye Assessmentjaypee01100% (1)
- Cranial Nerve ExaminationDocument3 pagesCranial Nerve ExaminationtomodachiNo ratings yet
- Cranial Nerves: DR Dyan Roshinta Laksmi Dewi, SP.S SMF Saraf Rsud DR Soedarso PontianakDocument19 pagesCranial Nerves: DR Dyan Roshinta Laksmi Dewi, SP.S SMF Saraf Rsud DR Soedarso PontianakVidia AsriyantiNo ratings yet
- Assistive Devices For WalkingDocument4 pagesAssistive Devices For WalkingAbigail Mangaoang100% (1)
- Health Assessment Complete 2Document14 pagesHealth Assessment Complete 2kimberly100% (1)
- Cranial NervesDocument27 pagesCranial NervesTni JolieNo ratings yet
- Head To Toe Assessment (Body Parts)Document16 pagesHead To Toe Assessment (Body Parts)jutah2013No ratings yet
- Apgar ScoreDocument2 pagesApgar Scorejulialeo100% (3)
- Neurologic Assessment: Chapter OutlineDocument22 pagesNeurologic Assessment: Chapter Outlinekenthepa100% (1)
- Neuro Assessment: The Single Most Important AssessmentDocument10 pagesNeuro Assessment: The Single Most Important AssessmentpapadaadNo ratings yet
- Abdominal AssessmentDocument2 pagesAbdominal AssessmentMuhammad Fahrin AzhariNo ratings yet
- During The CCA Exam. Please Note You Are Responsible For The Content Knowledge of Items Without An Asterisk That May Be Present On The Written Exam.Document2 pagesDuring The CCA Exam. Please Note You Are Responsible For The Content Knowledge of Items Without An Asterisk That May Be Present On The Written Exam.helamahjoubmounirdmoNo ratings yet
- Summary of Cranial Nerves and Their FunctionsDocument2 pagesSummary of Cranial Nerves and Their Functionscrsoriano2011No ratings yet
- Physical Assessment Head To ToeDocument4 pagesPhysical Assessment Head To ToeFely Theresa Lanes Loreno95% (43)
- Head To Toe AssessmentDocument56 pagesHead To Toe AssessmentmisshieNo ratings yet
- Complete Physical Examination Eyes, Ears, Nose, ThroatDocument103 pagesComplete Physical Examination Eyes, Ears, Nose, Throatjennylyn guadalupe100% (3)
- NEURO VITAL SIGNS ASSESSMENT Procedure and ChecklistDocument12 pagesNEURO VITAL SIGNS ASSESSMENT Procedure and ChecklistMemer-alasadNo ratings yet
- Physical Assessment Summary for Weak Hospitalized PatientDocument3 pagesPhysical Assessment Summary for Weak Hospitalized PatientRijelNo ratings yet
- Comprehensive Head To Toe AssessmentDocument22 pagesComprehensive Head To Toe Assessmentqueenzk80% (30)
- Cerebral Palsy AnatomyDocument5 pagesCerebral Palsy AnatomyIoana irimiaNo ratings yet
- Procedure Checklist Chapter 19: Assessing The Chest and LungsDocument2 pagesProcedure Checklist Chapter 19: Assessing The Chest and LungsjthsNo ratings yet
- Assessment of Head and NeckDocument11 pagesAssessment of Head and Neckjacnpoy100% (2)
- Head To Toe Assessment NRS 111Document4 pagesHead To Toe Assessment NRS 111Danielle Shull100% (2)
- Module 6 Breast Axilla Assessment-Edited 0 0Document13 pagesModule 6 Breast Axilla Assessment-Edited 0 0Laila PasiganNo ratings yet
- Head to Toe Physical Assessment GuideDocument16 pagesHead to Toe Physical Assessment Guideabagatsing100% (5)
- Anatomy and Physiology CVADocument11 pagesAnatomy and Physiology CVAmaryrose_jordan100% (6)
- Assessing the Abdomen: 4 Quadrants and 9 RegionsDocument54 pagesAssessing the Abdomen: 4 Quadrants and 9 RegionsWilma Acorin OrillinedaNo ratings yet
- 4 - Stroke FinalDocument74 pages4 - Stroke FinalSamir SkejicNo ratings yet
- Use The Following Criteria in Evaluating The Skill PerformanceDocument4 pagesUse The Following Criteria in Evaluating The Skill PerformancekookieNo ratings yet
- Neurological AssessmentDocument7 pagesNeurological AssessmentErika NicaNo ratings yet
- Nursing - Health AssessmentDocument17 pagesNursing - Health Assessmentzsazsageorge100% (1)
- Neurological Assessment: Alice E. Davis, PH.D., RNDocument6 pagesNeurological Assessment: Alice E. Davis, PH.D., RNdhekuh100% (2)
- Neuro AssessmentDocument13 pagesNeuro AssessmentOrlea Francisco-Sisio100% (2)
- Thorax and Lungs Assessment ChecklistDocument8 pagesThorax and Lungs Assessment ChecklistXing-Jin RomeroNo ratings yet
- Neurological AssessmentDocument9 pagesNeurological AssessmentrlinaoNo ratings yet
- Nursing Cardiovascular AssessmentDocument2 pagesNursing Cardiovascular Assessmentgladz25100% (2)
- Cranial Nerve Functions and Assessment MethodsDocument7 pagesCranial Nerve Functions and Assessment MethodsNewb TobikkoNo ratings yet
- 12 Cranial Nerves and AssessmentDocument9 pages12 Cranial Nerves and AssessmentRella QuelNo ratings yet
- Cranial Nerves Assessment: Prepared By: Eloisa M. Bonus, RN MANDocument56 pagesCranial Nerves Assessment: Prepared By: Eloisa M. Bonus, RN MANsarooah1994No ratings yet
- Examination of The Cranial Nerves: I OlfactoryDocument6 pagesExamination of The Cranial Nerves: I Olfactorygolagani praveenkumarNo ratings yet
- Neuro ExamDocument25 pagesNeuro ExamkamalNo ratings yet
- 12 Cranial Nerves AssessmentDocument8 pages12 Cranial Nerves AssessmentAllean Sarmiento Apolinario100% (1)
- Professional Skills Review Central Nervous System (CNS)Document25 pagesProfessional Skills Review Central Nervous System (CNS)Noora AlmuailiNo ratings yet
- Neurological ExaminationDocument58 pagesNeurological ExaminationMartin Ogbac100% (2)
- Neurological AssessmentDocument7 pagesNeurological AssessmentSharon LawrenceNo ratings yet
- ResearchDocument3 pagesResearchapolloNo ratings yet
- NCLEX Medical Terminology ReviewDocument15 pagesNCLEX Medical Terminology Reviewapollo100% (3)
- Medical AbbreviationsDocument10 pagesMedical AbbreviationsapolloNo ratings yet
- Treatment For Ectopic PregnancyDocument5 pagesTreatment For Ectopic PregnancyapolloNo ratings yet
- Cignal Channel 490Document2 pagesCignal Channel 490Arild JuliusNo ratings yet
- Geraads 2016 Pleistocene Carnivora (Mammalia) From Tighennif (Ternifine), AlgeriaDocument45 pagesGeraads 2016 Pleistocene Carnivora (Mammalia) From Tighennif (Ternifine), AlgeriaGhaier KazmiNo ratings yet
- English FinalDocument321 pagesEnglish FinalManuel Campos GuimeraNo ratings yet
- ACCOUNTING FOR SPECIAL EDUCATION FUNDSDocument12 pagesACCOUNTING FOR SPECIAL EDUCATION FUNDSIrdo KwanNo ratings yet
- List/Status of 655 Projects Upto 5.00 MW Capacity As On TodayDocument45 pagesList/Status of 655 Projects Upto 5.00 MW Capacity As On Todayganvaqqqzz21No ratings yet
- The Political Philosophy of Giorgio Agamben A Critical EvaluationDocument20 pagesThe Political Philosophy of Giorgio Agamben A Critical EvaluationLEANo ratings yet
- Financial Management Module - 3Document2 pagesFinancial Management Module - 3Roel AsduloNo ratings yet
- Perancangan Kota: Jurusan Perencanaan Wilayah Dan Kota Institut Teknologi Nasional Tahun 2021/2022Document27 pagesPerancangan Kota: Jurusan Perencanaan Wilayah Dan Kota Institut Teknologi Nasional Tahun 2021/2022idaNo ratings yet
- Colégio XIX de Março 2a Prova Substitutiva de InglêsDocument5 pagesColégio XIX de Março 2a Prova Substitutiva de InglêsCaio SenaNo ratings yet
- Curriculum Vitae (October 31, 2011)Document5 pagesCurriculum Vitae (October 31, 2011)Alvin Ringgo C. Reyes100% (1)
- Reading and Writing Skills: Quarter 4 - Module 1Document16 pagesReading and Writing Skills: Quarter 4 - Module 1Ericka Marie AlmadoNo ratings yet
- Onkyo TX NR555 ManualDocument100 pagesOnkyo TX NR555 ManualSudhit SethiNo ratings yet
- dlp4 Math7q3Document3 pagesdlp4 Math7q3Therence UbasNo ratings yet
- Once in his Orient: Le Corbusier and the intoxication of colourDocument4 pagesOnce in his Orient: Le Corbusier and the intoxication of coloursurajNo ratings yet
- Here Late?", She Asked Me.: TrangDocument3 pagesHere Late?", She Asked Me.: TrangNguyễn Đình TrọngNo ratings yet
- Unitrain I Overview enDocument1 pageUnitrain I Overview enDragoi MihaiNo ratings yet
- History: The Origin of Kho-KhotheDocument17 pagesHistory: The Origin of Kho-KhotheIndrani BhattacharyaNo ratings yet
- Asian Paints SmartCare Damp Proof Warranty for TerracesDocument11 pagesAsian Paints SmartCare Damp Proof Warranty for Terracesiman.krisman2109No ratings yet
- Bo de On Thi Hoc Ki 1 Lop 3 Mon Tieng AnhDocument66 pagesBo de On Thi Hoc Ki 1 Lop 3 Mon Tieng AnhHằng DiệuNo ratings yet
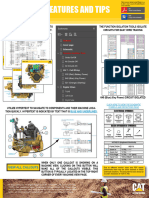
- Schematic Electric System Cat D8T Vol1Document33 pagesSchematic Electric System Cat D8T Vol1Andaru Gunawan100% (1)
- Commercial Contractor Exam Study GuideDocument7 pagesCommercial Contractor Exam Study Guidejclark13010No ratings yet
- Little Match GirlDocument8 pagesLittle Match GirlsubhaseduNo ratings yet
- Line GraphDocument13 pagesLine GraphMikelAgberoNo ratings yet
- Genocide/Politicides, 1954-1998 - State Failure Problem SetDocument9 pagesGenocide/Politicides, 1954-1998 - State Failure Problem SetSean KimNo ratings yet
- 2020052336Document4 pages2020052336Kapil GurunathNo ratings yet
- Inferences Worksheet 6Document2 pagesInferences Worksheet 6Alyssa L0% (1)
- 3 QDocument2 pages3 QJerahmeel CuevasNo ratings yet
- Bhojpuri PDFDocument15 pagesBhojpuri PDFbestmadeeasy50% (2)
- Presidential Decree 1613 Amending The Law of ArsonDocument19 pagesPresidential Decree 1613 Amending The Law of ArsonBfp Atimonan QuezonNo ratings yet
- Comment On Motion To Release Vehicle BeridoDocument3 pagesComment On Motion To Release Vehicle BeridoRaffy PangilinanNo ratings yet