You might also like
- Bipolar DisordersDocument8 pagesBipolar Disorderssarguss14100% (2)
- Pediatric GI RadiologyDocument6 pagesPediatric GI Radiologysarguss14No ratings yet
- Cerebellar DisordersDocument29 pagesCerebellar DisordersArslan Aslam100% (1)
- 1 - Neuro Assessment 2021 - 336Document30 pages1 - Neuro Assessment 2021 - 336HADI BADWAN100% (2)
- Developmental AssessmentDocument3 pagesDevelopmental Assessmentsarguss14No ratings yet
- Introduction To RadiologyDocument3 pagesIntroduction To Radiologysarguss14No ratings yet
- Test Bank For Basic Pharmacology For Nursing 17th EditionDocument10 pagesTest Bank For Basic Pharmacology For Nursing 17th EditionUsman HaiderNo ratings yet
- Wall Neuro 2010Document34 pagesWall Neuro 2010Kath Jacinto100% (1)
- NeuroradiologyDocument25 pagesNeuroradiologysarguss14100% (2)
- Pleura and MediastinumDocument16 pagesPleura and Mediastinumsarguss14100% (1)
- Neuroscience - 4.3 - Examination of Cerebellar Systems and Meninges (KSD)Document4 pagesNeuroscience - 4.3 - Examination of Cerebellar Systems and Meninges (KSD)Kevin C. AguilarNo ratings yet
- Cardiac ImagingDocument7 pagesCardiac Imagingsarguss14No ratings yet
- Dissociative and Eating DisordersDocument6 pagesDissociative and Eating Disorderssarguss14No ratings yet
- Exercise For CoordinationDocument19 pagesExercise For Coordinationbpt250% (2)
- Acetabulum FractureDocument32 pagesAcetabulum FracturePhysiotherapist AliNo ratings yet
- NeuroradiologyDocument11 pagesNeuroradiologysarguss14100% (2)
- Epidural and Spinal AnesthesiaDocument86 pagesEpidural and Spinal Anesthesiasarguss1471% (7)
- CRANIALDocument11 pagesCRANIALDemianaNo ratings yet
- Genitourinary SystemDocument8 pagesGenitourinary Systemsarguss14100% (1)
- Cyanotic Congenital Heart Diseases, Etc.Document12 pagesCyanotic Congenital Heart Diseases, Etc.sarguss14100% (2)
- Lower Crossed SyndromeDocument8 pagesLower Crossed SyndromeThaseen75% (4)
- Small BowelDocument4 pagesSmall Bowelsarguss14100% (1)
- Sensory Examination and CoordinationDocument7 pagesSensory Examination and CoordinationFatimah Alsultan100% (1)
- From Doc Bandong's Own Words:: Shar 1 of 20Document20 pagesFrom Doc Bandong's Own Words:: Shar 1 of 20sarguss14100% (1)
- 9 Hip & Lumber DDDocument29 pages9 Hip & Lumber DDHeba Abo bakrNo ratings yet
- MED 2.7 Gait and StationDocument3 pagesMED 2.7 Gait and StationelleinasNo ratings yet
- Neuro PEDocument36 pagesNeuro PEkhaderbasha2020No ratings yet
- Hip Examination - OSCE Guide - Geeky MedicsDocument6 pagesHip Examination - OSCE Guide - Geeky MedicsAmcDelhiNo ratings yet
- Neurological Examination of The Limbs TextDocument8 pagesNeurological Examination of The Limbs Textvidur_talrejaNo ratings yet
- Med TemplateDocument1 pageMed TemplateAnbar100% (1)
- Cerebellar DisordersDocument51 pagesCerebellar DisorderswasimNo ratings yet
- Inhalational Anesthetics: Patigas, Requinta, ResuelloDocument88 pagesInhalational Anesthetics: Patigas, Requinta, Resuellosarguss140% (1)
- Final Yemen Cmam Guidelines - Feb 2014Document243 pagesFinal Yemen Cmam Guidelines - Feb 2014Anas Abdo SenanNo ratings yet
- Functional AssesmentDocument22 pagesFunctional AssesmentHeri WibisonoNo ratings yet
- Cranial Nerve AssessmentDocument5 pagesCranial Nerve AssessmentBAdz TanNo ratings yet
- Neurological AssessmentDocument19 pagesNeurological AssessmentRyan-Jay Abolencia100% (1)
- The Neurological Exam: Respect and Kindness. When You Enter TheDocument9 pagesThe Neurological Exam: Respect and Kindness. When You Enter TheRemelou Garchitorena Alfelor100% (1)
- Stage 1: Dorsal Induction: Pediatric NeuroradiologyDocument8 pagesStage 1: Dorsal Induction: Pediatric Neuroradiologysarguss14100% (1)
- Test 3 July 2018Document8 pagesTest 3 July 2018Mobin Ur Rehman KhanNo ratings yet
- ALI ZAYED Medical CertificateDocument3 pagesALI ZAYED Medical CertificateZizo AlaliNo ratings yet
- Homevisit PlanDocument13 pagesHomevisit PlanTimmy CincoNo ratings yet
- Neuro 101: Nursing Neuro Assessment: Kristen Ankrom, RN, SCRN, CCCC Stroke Coordinator Coliseum Medical CentersDocument29 pagesNeuro 101: Nursing Neuro Assessment: Kristen Ankrom, RN, SCRN, CCCC Stroke Coordinator Coliseum Medical CentersDarvin MathewNo ratings yet
- Introduction To Cerebral PalsyDocument23 pagesIntroduction To Cerebral PalsyVenkata Nagaraj Mummadisetty100% (1)
- Coolection of SpecimenDocument16 pagesCoolection of SpecimenPracticalranjuNo ratings yet
- Health Talk TopicsDocument3 pagesHealth Talk Topicsvarshasharma0562% (13)
- Gallbladder, Liver, Pancreas and SpleenDocument19 pagesGallbladder, Liver, Pancreas and Spleensarguss14100% (3)
- Brain Imaging of Drug EffectsDocument36 pagesBrain Imaging of Drug EffectsLuis Concepción AramendíaNo ratings yet
- Immunization UipDocument20 pagesImmunization Uipdevesh gargNo ratings yet
- Upper Extremity AnatomyDocument1 pageUpper Extremity AnatomyKristineNo ratings yet
- Assesment of Cerebeller Function 30-04-2020Document9 pagesAssesment of Cerebeller Function 30-04-2020Harshit SharmaNo ratings yet
- Pemeriksaan Keseimbangan Dan KoordinasiDocument8 pagesPemeriksaan Keseimbangan Dan KoordinasidrecoriusxNo ratings yet
- Coordination, Balance, Gait and PostureDocument15 pagesCoordination, Balance, Gait and PostureFA AnthonyNo ratings yet
- Cerebellar Function Assessment NHA 2021 2Document26 pagesCerebellar Function Assessment NHA 2021 2Larra LorenzoNo ratings yet
- Tests That Will Elicit Cerebellar Signs Are inDocument4 pagesTests That Will Elicit Cerebellar Signs Are inRaina DeWyzeNo ratings yet
- Diagnosing: Muskuloskeletal PainDocument44 pagesDiagnosing: Muskuloskeletal PainRizka RamadaniNo ratings yet
- 1 - Stance, Gait and CoordinationDocument65 pages1 - Stance, Gait and CoordinationsofiaNo ratings yet
- Coordination Exercise 3Document16 pagesCoordination Exercise 3Ella CooperNo ratings yet
- Vestibular Interp PDFDocument5 pagesVestibular Interp PDFElsa VionaNo ratings yet
- Upper & Lower Limb ExaminationDocument20 pagesUpper & Lower Limb Examinationcvmqx7yppd100% (1)
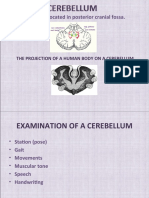
- A Cerebellum Is Located in Posterior Cranial Fossa.: The Projection of A Human Body On A CerebellumDocument9 pagesA Cerebellum Is Located in Posterior Cranial Fossa.: The Projection of A Human Body On A CerebellumShourya PratapNo ratings yet
- Cerebellar Examination OSCE GuideDocument11 pagesCerebellar Examination OSCE GuideLeen abusarhanNo ratings yet
- Sem 2 Week 4Document30 pagesSem 2 Week 4Fong Yu-hengNo ratings yet
- Cerebellar ExaminationDocument1 pageCerebellar ExaminationPraveenNo ratings yet
- 4-Back Examination ٢Document6 pages4-Back Examination ٢رغد رشيدNo ratings yet
- Ortho Neuro ExamsDocument0 pagesOrtho Neuro ExamsMaybs Palec Pamplona-ParreñoNo ratings yet
- Spine 2020Document1 pageSpine 2020fihimeh581No ratings yet
- Neurological AssessmentDocument76 pagesNeurological Assessmentjcabatit3No ratings yet
- Neuro LabDocument37 pagesNeuro LabIonut SegaNo ratings yet
- Cerebellar Function Tests: Experiment 29: Md-1C Group 5Document42 pagesCerebellar Function Tests: Experiment 29: Md-1C Group 5Verlette Roselle Aguisanda LizardoNo ratings yet
- Neurological Eval SensoryDocument25 pagesNeurological Eval SensoryAyen FornollesNo ratings yet
- Procedures For Neurologic Health AssessmentDocument6 pagesProcedures For Neurologic Health Assessmentelmer.platiljrNo ratings yet
- Co-Ordination ExercisesDocument22 pagesCo-Ordination ExercisesBudi DarmaNo ratings yet
- WA0044.encDocument40 pagesWA0044.encmalfed adrianoNo ratings yet
- Abnormalities of Gait & PostureDocument24 pagesAbnormalities of Gait & PosturePamudri BasnayakeNo ratings yet
- HINTDocument16 pagesHINTMahynaz ElkomyNo ratings yet
- Professional Skills Review Central Nervous System (CNS)Document25 pagesProfessional Skills Review Central Nervous System (CNS)Noora AlmuailiNo ratings yet
- Script NeuroDocument3 pagesScript NeuroKrysstal GerongaNo ratings yet
- Neuro Sensory AssessmentDocument46 pagesNeuro Sensory AssessmentPrecious SantayanaNo ratings yet
- Exam KneeDocument11 pagesExam KneesingwongcsNo ratings yet
- Case PresentationDocument37 pagesCase PresentationRevan NasirNo ratings yet
- Adult Psychiatric Sensory Integration EvaluationDocument18 pagesAdult Psychiatric Sensory Integration Evaluationemesep1850% (2)
- Central Integration of Motor FunctionDocument3 pagesCentral Integration of Motor FunctionM51785No ratings yet
- Lec7 Assessment of SpineDocument35 pagesLec7 Assessment of Spinesana mumtazNo ratings yet
- Cervical Ortho TestsDocument74 pagesCervical Ortho Testsjdavis3100% (1)
- WK 6 Study QsDocument7 pagesWK 6 Study Qsapi-479720222No ratings yet
- Examination of The Hip Joint - RP's Ortho NotesDocument5 pagesExamination of The Hip Joint - RP's Ortho NotesSabari NathNo ratings yet
- Axial Arthritis: Degenerative Annular DiseaseDocument18 pagesAxial Arthritis: Degenerative Annular Diseasesarguss14100% (1)
- Kidney, Ureter, BladderDocument12 pagesKidney, Ureter, Bladdersarguss14100% (1)
- Bone TumorsDocument15 pagesBone Tumorssarguss1450% (2)
- Congenital Cystic Adenomatoid Malformation (CCAM)Document7 pagesCongenital Cystic Adenomatoid Malformation (CCAM)sarguss14No ratings yet
- Substance AbuseDocument4 pagesSubstance Abusesarguss14No ratings yet
- The Normal Kidney: Pediatrics 2 The Urinary System and Urinary Tract InfectionsDocument4 pagesThe Normal Kidney: Pediatrics 2 The Urinary System and Urinary Tract Infectionssarguss14No ratings yet
- DepressionDocument3 pagesDepressionsarguss14No ratings yet
- Mental Retardation and Learning DisordersDocument4 pagesMental Retardation and Learning Disorderssarguss14100% (1)
- Respiratory Distress of The NewbornDocument3 pagesRespiratory Distress of The Newbornsarguss14100% (1)
- Pediatric Endocrinology Part 2: Pediatrics 2Document8 pagesPediatric Endocrinology Part 2: Pediatrics 2sarguss14No ratings yet
- Child Abuse and NeglectDocument3 pagesChild Abuse and Neglectsarguss14No ratings yet
- Neonatal Anaesthesia 2 Anaesthesia For Neonates With Abdominal Wall DefectsDocument10 pagesNeonatal Anaesthesia 2 Anaesthesia For Neonates With Abdominal Wall DefectsDr. Anish GolchhaNo ratings yet
- ALGLUCOSIDASE ALFA 50 MG-VIAL (Myiztme)Document2 pagesALGLUCOSIDASE ALFA 50 MG-VIAL (Myiztme)asdwasdNo ratings yet
- Panduan Kesehatan OlahragaDocument1 pagePanduan Kesehatan OlahragaVidini Kusuma AjiNo ratings yet
- Volume 05 No.1Document28 pagesVolume 05 No.1Rebin AliNo ratings yet
- Classified AdsDocument3 pagesClassified Adsapi-312735990No ratings yet
- Library Genesis PDFDocument8 pagesLibrary Genesis PDFSipra PaulNo ratings yet
- PDF To WordDocument284 pagesPDF To WordVictoria UrsachiNo ratings yet
- Introduction To Pathology Infectious DiseasesDocument37 pagesIntroduction To Pathology Infectious DiseasesNirav PatelNo ratings yet
- Laguna State Polytechnic University: College of Nursing and Allied Health A.Y. 2021-22 PurposeDocument4 pagesLaguna State Polytechnic University: College of Nursing and Allied Health A.Y. 2021-22 PurposeKristine Louise JavierNo ratings yet
- Planning Design and Analysis of G+1 Hospital Building For Iiit Srikakulam CampusDocument1 pagePlanning Design and Analysis of G+1 Hospital Building For Iiit Srikakulam CampusSaritha TejavathNo ratings yet
- EndosDocument38 pagesEndosYogi AnjasmaraNo ratings yet
- 11 - Genitourinary Injuries TestDocument3 pages11 - Genitourinary Injuries TestSusi YuliawatiNo ratings yet
- Idrrmu Written Exam ReviewerDocument132 pagesIdrrmu Written Exam ReviewerDaniel Adrian FalaminianoNo ratings yet
- Review: How Old Is This Fracture? Radiologic Dating of Fractures in Children: A Systematic ReviewDocument5 pagesReview: How Old Is This Fracture? Radiologic Dating of Fractures in Children: A Systematic Reviewsigne_paoNo ratings yet
- JCDR 10 FC01Document4 pagesJCDR 10 FC01Adriyan SikumalayNo ratings yet
- MAPEHDocument9 pagesMAPEHNoraNo ratings yet
- Team Code 34 PDocument22 pagesTeam Code 34 PShivam TiwaryNo ratings yet
- Abdomen PE ChecklistDocument6 pagesAbdomen PE ChecklistJulienne Sanchez-SalazarNo ratings yet
- RUNNING HEAD: A Powerful Noise Reflective Essay Mahan 1Document5 pagesRUNNING HEAD: A Powerful Noise Reflective Essay Mahan 1Rachael MahanNo ratings yet
- Drug StudyDocument2 pagesDrug StudyJi Vista MamigoNo ratings yet
- GMR 2019Document6 pagesGMR 2019arvindat14No ratings yet