You might also like
- Nokia 2630 User Guide: 9203559 Issue 2 ENDocument69 pagesNokia 2630 User Guide: 9203559 Issue 2 ENTataSaleNo ratings yet
- Truefire Swing Ukulele Progression 1 - C C#dim C6 Dm7 G9: Marcy MarxerDocument1 pageTruefire Swing Ukulele Progression 1 - C C#dim C6 Dm7 G9: Marcy MarxerMTEMEINo ratings yet
- Clinch Mountain Backstep: aEAC#E Tuning, Brainjo Level 3Document1 pageClinch Mountain Backstep: aEAC#E Tuning, Brainjo Level 3MTEMEINo ratings yet
- Reeling Silk BookDocument13 pagesReeling Silk BookMTEMEI100% (3)
- The Ballad of Jed: GDGBD Tuning, Brainjo Level 2Document1 pageThe Ballad of Jed: GDGBD Tuning, Brainjo Level 2MTEMEINo ratings yet
- Nokia 2630 User Guide: 9203559 Issue 2 ENDocument69 pagesNokia 2630 User Guide: 9203559 Issue 2 ENTataSaleNo ratings yet
- Woman Called Mary TabDocument7 pagesWoman Called Mary TabMTEMEI100% (1)
- Speed Ladder DrillsDocument95 pagesSpeed Ladder Drillsmtemei4414No ratings yet
- Module 6 Lesson 7 PDFDocument1 pageModule 6 Lesson 7 PDFMTEMEINo ratings yet
- Cider: aDADE Tuning, Brainjo Level 2Document1 pageCider: aDADE Tuning, Brainjo Level 2MTEMEINo ratings yet
- Whiskey Before Breakfast2Document3 pagesWhiskey Before Breakfast2MTEMEINo ratings yet
- The Spider - Music Scores and Helpful Notes: Section 6, Lecture 15Document1 pageThe Spider - Music Scores and Helpful Notes: Section 6, Lecture 15MTEMEINo ratings yet
- Vol 19 ST2 Online Approved 5 PDFDocument1 pageVol 19 ST2 Online Approved 5 PDFMTEMEINo ratings yet
- 12 Bar Blues Chart PDFDocument1 page12 Bar Blues Chart PDFMTEMEINo ratings yet
- Yoga 3D: Quick Reference GuideDocument15 pagesYoga 3D: Quick Reference GuideMTEMEINo ratings yet
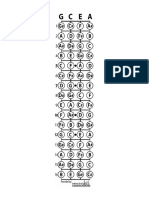
- Fretboard DiagramDocument1 pageFretboard DiagramMTEMEINo ratings yet
- Rotatorcuff RehabDocument3 pagesRotatorcuff RehabMTEMEI100% (1)
- Nrol Blank Training Log For LifeDocument6 pagesNrol Blank Training Log For Lifescason9100% (1)
- Plantar FasciaDocument7 pagesPlantar Fasciamtemei4414No ratings yet
- Alwyn Cosgrove - The New Rules of Lifting Supercharged - 2013 - LogsDocument24 pagesAlwyn Cosgrove - The New Rules of Lifting Supercharged - 2013 - Logsh4leluy4h100% (1)
- PSSB Home Exercise ProgrammeDocument27 pagesPSSB Home Exercise ProgrammeMTEMEINo ratings yet
- Otago Home Exercise ProgrammeDocument46 pagesOtago Home Exercise ProgrammeMTEMEINo ratings yet
- Solo Blues 1Document1 pageSolo Blues 1MTEMEINo ratings yet
- NZ Otago ManualDocument71 pagesNZ Otago ManualMTEMEINo ratings yet
- Chair Based Home Exercise Programme PDFDocument23 pagesChair Based Home Exercise Programme PDFmtemei4414100% (1)
- Solo Blues 1Document1 pageSolo Blues 1MTEMEINo ratings yet
- Reeling Silk IDocument6 pagesReeling Silk IMTEMEINo ratings yet
- Plantar FasciaDocument7 pagesPlantar Fasciamtemei4414No ratings yet
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Ancient History Mod 1 Stone AgeDocument9 pagesAncient History Mod 1 Stone AgeShubham KhokerNo ratings yet
- X606 PDFDocument1 pageX606 PDFDany OrioliNo ratings yet
- Manual Helios 2Document33 pagesManual Helios 2Jose Luis Albornoz HermosillaNo ratings yet
- Practice Tests U5Document15 pagesPractice Tests U5Ihshan Destro IqbalNo ratings yet
- General ToleranceDocument16 pagesGeneral ToleranceNARENDER SINGHNo ratings yet
- Performance of Gesture Controlled DroneDocument11 pagesPerformance of Gesture Controlled DroneKrishna SivaNo ratings yet
- Fertilizer Transportation Sampling: International Fertilizer Industry Association (IFA)Document10 pagesFertilizer Transportation Sampling: International Fertilizer Industry Association (IFA)lamvanthongNo ratings yet
- Loctite 2701: Technical Data SheetDocument3 pagesLoctite 2701: Technical Data SheethendrabudimanNo ratings yet
- CVE162 Third ExamDocument7 pagesCVE162 Third ExamMerwin Andrew UyNo ratings yet
- Ch-04 Moving Charges and Magnetism: Lect-10Document32 pagesCh-04 Moving Charges and Magnetism: Lect-10Kishan KumarNo ratings yet
- Full Download Essentials of Ecology 4th Edition Begon Test BankDocument35 pagesFull Download Essentials of Ecology 4th Edition Begon Test Bankfannerbarogram.ywlkl100% (19)
- Stonex S70G Handheld User Manual: Jul 2020 - Ver.1.0Document55 pagesStonex S70G Handheld User Manual: Jul 2020 - Ver.1.0Walter Huallpa RedondezNo ratings yet
- Five basic steps for fixture design processDocument6 pagesFive basic steps for fixture design processykc38No ratings yet
- Multi VibratorsDocument11 pagesMulti VibratorsPallavi Kr K RNo ratings yet
- Presentation On The Project Topic: A Study of Comparative Use of Light Gauge Steel Construction Over Concrete Works For Public and Housing UnitsDocument14 pagesPresentation On The Project Topic: A Study of Comparative Use of Light Gauge Steel Construction Over Concrete Works For Public and Housing UnitsBakareNo ratings yet
- Gabion BasketsDocument1 pageGabion BasketsAziz Khan KakarNo ratings yet
- FH12, FH16 Abs A517769 - B266298Document10 pagesFH12, FH16 Abs A517769 - B266298Евгений АксёновNo ratings yet
- The Secrets of Viktor SchaubergerDocument1 pageThe Secrets of Viktor SchaubergerAmanat Hossain SumonNo ratings yet
- Acoustic SensorsDocument7 pagesAcoustic SensorsNihal AhmadNo ratings yet
- Grade-10 Module-3 MAPEHDocument8 pagesGrade-10 Module-3 MAPEHFerry May ManzonNo ratings yet
- DR Khaled Final Exam MCQ 2012 - 2013Document89 pagesDR Khaled Final Exam MCQ 2012 - 2013ﻣﻠﻚ عيسى100% (2)
- 21ELN24 - Question Bank For ExamDocument4 pages21ELN24 - Question Bank For ExamEmail ServiceNo ratings yet
- Modern Digital Electronics R P Jain Solution ManualDocument167 pagesModern Digital Electronics R P Jain Solution ManualHarpreet PaliaNo ratings yet
- Product Correction: Urgent Immediate Action RequiredDocument7 pagesProduct Correction: Urgent Immediate Action RequiredŽeljkoNo ratings yet
- Test LPDocument127 pagesTest LPUmar DiwarmanNo ratings yet
- Configurations & Parts Identification: Trailer Suspension SeriesDocument26 pagesConfigurations & Parts Identification: Trailer Suspension SeriesleosignareNo ratings yet
- Full Download Introduction To Statistical Methods and Data Analysis 6th Edition Ott Solutions ManualDocument36 pagesFull Download Introduction To Statistical Methods and Data Analysis 6th Edition Ott Solutions Manualrucaizatax98% (45)
- Cononical-Active DirectoryDocument21 pagesCononical-Active DirectoryHemanth RyaliNo ratings yet
- Water Ace PumpDocument20 pagesWater Ace PumpDana Milner100% (1)
- The Really Useful Little Book of Knots - Owen P. (2004)Document81 pagesThe Really Useful Little Book of Knots - Owen P. (2004)tkbernardi6410100% (3)