You might also like
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
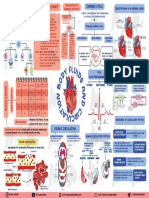
- Cardiovascular MneumonicsDocument10 pagesCardiovascular MneumonicsKaly RieNo ratings yet
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- Atrial FibrillationDocument19 pagesAtrial FibrillationAnwari MuhammadNo ratings yet
- Zoology Full PDF EMDocument108 pagesZoology Full PDF EMSmiruthi RavichandranNo ratings yet
- Blood Flow Through The HeartDocument2 pagesBlood Flow Through The HeartZah SchlafmützeNo ratings yet
- General.: Blood CirculationDocument3 pagesGeneral.: Blood CirculationJessica MichaelNo ratings yet
- PREECLAMPSIADocument60 pagesPREECLAMPSIAMary Grace MasNo ratings yet
- Pediatric Cardiovascular DisordersDocument9 pagesPediatric Cardiovascular Disorderscayla mae carlos0% (1)
- Analogue New Tools Challange Diabetes (Slide)Document67 pagesAnalogue New Tools Challange Diabetes (Slide)Habiby Habibaty QolbiNo ratings yet
- Novomix Tawang Mangu SW 12 Mei 2012Document39 pagesNovomix Tawang Mangu SW 12 Mei 2012Habiby Habibaty QolbiNo ratings yet
- Analogue New Tools Challange Diabetes (Slide)Document67 pagesAnalogue New Tools Challange Diabetes (Slide)Habiby Habibaty QolbiNo ratings yet
- Basal Insulin TreatmentDocument33 pagesBasal Insulin TreatmentHabiby Habibaty QolbiNo ratings yet
- Workshop Residen 1Document2 pagesWorkshop Residen 1Habiby Habibaty QolbiNo ratings yet
- Gagal Ginjal Akut Dan Kronik: Divisi Ginjal & Hipertensi SMF/Lab - Ilmu Penyakit Dalam FK - UNS / RSUD DR - MoewardiDocument29 pagesGagal Ginjal Akut Dan Kronik: Divisi Ginjal & Hipertensi SMF/Lab - Ilmu Penyakit Dalam FK - UNS / RSUD DR - MoewardiHabiby Habibaty QolbiNo ratings yet
- Workshop Residen 1Document2 pagesWorkshop Residen 1Habiby Habibaty QolbiNo ratings yet
- GESTASIONAL DIABETES MELLITUS SimposiumDocument18 pagesGESTASIONAL DIABETES MELLITUS SimposiumHabiby Habibaty QolbiNo ratings yet
- Student Registration List with Personal DataDocument8 pagesStudent Registration List with Personal DataHabiby Habibaty QolbiNo ratings yet
- 30-8 Final Ann Konker, PIT, Treg CetakDocument4 pages30-8 Final Ann Konker, PIT, Treg CetakHabiby Habibaty Qolbi100% (1)
- The Role of Rapid Acting Analogue in Basal-Bolus StrategyDocument39 pagesThe Role of Rapid Acting Analogue in Basal-Bolus StrategyHabiby Habibaty QolbiNo ratings yet
- Denah Kampus A UNAIRDocument1 pageDenah Kampus A UNAIRHabiby Habibaty QolbiNo ratings yet
- Takmir MasjidDocument5 pagesTakmir MasjidHabiby Habibaty QolbiNo ratings yet
- Cancers Related To Immunodeficiencies: Update and PerspectivesDocument13 pagesCancers Related To Immunodeficiencies: Update and PerspectivesHabiby Habibaty QolbiNo ratings yet
- Pi Is 0091674917309259Document8 pagesPi Is 0091674917309259Habiby Habibaty QolbiNo ratings yet
- Acute Coronary Syndrome: Widhy Puji H Bahan: - Pathophysiology of Heart Disease - ACS AHA 2010 - ACS AHA 2013Document17 pagesAcute Coronary Syndrome: Widhy Puji H Bahan: - Pathophysiology of Heart Disease - ACS AHA 2010 - ACS AHA 2013Habiby Habibaty QolbiNo ratings yet
- 3 Acute Coronary SyndromeDocument57 pages3 Acute Coronary SyndromestephaniedianNo ratings yet
- Insulin GarglineDocument28 pagesInsulin GarglineHabiby Habibaty Qolbi100% (1)
- Everything You Need to Know About Spine ExaminationDocument41 pagesEverything You Need to Know About Spine ExaminationHabiby Habibaty QolbiNo ratings yet
- HIP and BackDocument48 pagesHIP and BackHabiby Habibaty QolbiNo ratings yet
- Notes PediaDocument56 pagesNotes PediaDick Morgan FerrerNo ratings yet
- Circulatory System Packet BDocument5 pagesCirculatory System Packet BLouise SalvadorNo ratings yet
- Unit 4 (4) STRUCTURE & FUNCTION OF THE MAMMALIAN HEARTDocument9 pagesUnit 4 (4) STRUCTURE & FUNCTION OF THE MAMMALIAN HEARTDINAMANI 0inamNo ratings yet
- CARDIAC TUMORS Approach To ManagementDocument12 pagesCARDIAC TUMORS Approach To ManagementAnkit GulatiNo ratings yet
- Austin Journal of Clinical CardiologyDocument15 pagesAustin Journal of Clinical CardiologyAustin Publishing GroupNo ratings yet
- Lesson 5 - Respiratory and Circulatory SystemsDocument60 pagesLesson 5 - Respiratory and Circulatory SystemsBeng QuinnNo ratings yet
- Sean Burke - Virtual-Shark-Dissection QuestionsDocument5 pagesSean Burke - Virtual-Shark-Dissection Questionsapi-386190429No ratings yet
- REGULATION OF CARDIAC ACTIVITYDocument1 pageREGULATION OF CARDIAC ACTIVITYservoculus machatteNo ratings yet
- SWC12Document11 pagesSWC12vikkasNo ratings yet
- 3 MAJOR OPENINGS /right Atirum: Cardiovascular System Serious PericardiumDocument3 pages3 MAJOR OPENINGS /right Atirum: Cardiovascular System Serious PericardiumAebee Alcaraz100% (1)
- Anatomi Dan Fisiologi Sistem Kardiovaskular: Hendra FirmansyahDocument19 pagesAnatomi Dan Fisiologi Sistem Kardiovaskular: Hendra Firmansyahrandy sepasaciNo ratings yet
- DLL SCI9circulatory2Document2 pagesDLL SCI9circulatory2Mantikar IsmaelNo ratings yet
- Normal Oxygen Transport: Susanne A ClarkDocument256 pagesNormal Oxygen Transport: Susanne A Clarkghoncheh0% (1)
- DM Cardiology (Medicine) June 2018 PDFDocument17 pagesDM Cardiology (Medicine) June 2018 PDFAnil SharmaNo ratings yet
- 4 EL Husseinys Essentials of Cardiovascular System @eduwaves360Document236 pages4 EL Husseinys Essentials of Cardiovascular System @eduwaves360ahmed_abu_alrobNo ratings yet
- Circulatory System ReadingDocument4 pagesCirculatory System ReadingAlejandro PabonNo ratings yet
- Heart Anatomy LabDocument19 pagesHeart Anatomy LabDisshiNo ratings yet
- CARDIAC ARRHYTHMIA GUIDEDocument44 pagesCARDIAC ARRHYTHMIA GUIDEChinenye Akwue100% (1)
- Test Bank For Ekg Plain and Simple 3rd Edition EllisDocument8 pagesTest Bank For Ekg Plain and Simple 3rd Edition Elliscanebrutalfniy66No ratings yet
- Association Rule Mining To Detect Factors Which Contribute To Heart Disease in Males and Females 2013Document8 pagesAssociation Rule Mining To Detect Factors Which Contribute To Heart Disease in Males and Females 2013Great Ideas in 5 Minutes افكارعظيمة في 5 دقائقNo ratings yet
- MN - B4 Revision LessonDocument34 pagesMN - B4 Revision Lessonspamzz063No ratings yet
- Medicine National Competitive Entrance Examination 2018Document13 pagesMedicine National Competitive Entrance Examination 2018lalixs71No ratings yet
- Heart: Answers To Workbook ActivitiesDocument12 pagesHeart: Answers To Workbook Activitiesapi-20954241433% (3)