Professional Documents
Culture Documents
Deep Venous Thrombosis: Practice Essentials
Uploaded by
phoechoexOriginal Title
Copyright
Available Formats
Share this document
Did you find this document useful?
Is this content inappropriate?
Report this DocumentCopyright:
Available Formats
Deep Venous Thrombosis: Practice Essentials
Uploaded by
phoechoexCopyright:
Available Formats
Deep Venous Thrombosis
http://emedicine.medscape.com/article/1911303-overview
Medscape Reference Reference
News Reference Education MEDLINE
Deep Venous Thrombosis
Author: Kaushal (Kevin) Patel, MD; Chief Editor: Barry E Brenner, MD, PhD, FACEP more... Updated: Jan 14, 2013
Practice Essentials
Signs and symptoms
Symptoms of deep venous thrombosis (DVT) may include the following: Edema: Most specific symptom Leg pain: Occurs in 50% of patients but is nonspecific Tenderness: Occurs in 75% of patients Warmth or erythema of the skin over the area of thrombosis Clinical symptoms of pulmonary embolism (PE) as the primary manifestation As many as 46% with patients with classic symptoms have negative venograms, [1] and as many as 50% of those with image-documented venous thrombosis lack specific symptoms.[1, 2] No single physical finding or combination of symptoms and signs is sufficiently accurate to establish the diagnosis of DVT, but physical findings in DVT may include the following: Calf pain on dorsiflexion of the foot (Homans sign) A palpable, indurated, cordlike, tender subcutaneous venous segment Variable discoloration of the lower extremity Blanched appearance of the leg because of edema (relatively rare) Potential complications of DVT include the following: As many as 40% of patients have silent PE when symptomatic DVT is diagnosed [3] Paradoxic emboli (rare) Recurrent DVT Postthrombotic syndrome (PTS) See Clinical Presentation for more detail.
Diagnosis
The American Academy of Family Physicians (AAFP)/American College of Physicians (ACP) recommendations for workup of patients with probable DVT are as follows:[4] Validated clinical prediction rules (eg, Wells) should be used to estimate the pretest probability of venous thromboembolism (VTE) and interpret test results In appropriately selected patients with low pretest probability of DVT or PE, it is reasonable to obtain a high-sensitivity D-dimer In patients with intermediate to high pretest probability of lower-extremity DVT, ultrasonography is
1 of 27
05/02/2013 6:21
Deep Venous Thrombosis
http://emedicine.medscape.com/article/1911303-overview
recommended In patients with intermediate or high pretest probability of PE, diagnostic imaging studies (eg, ventilationperfusion scan, multidetector helical CT, and pulmonary angiography) are required The main laboratory studies to be considered include the following: D-dimer testing Coagulation studies (eg, prothrombin time and activated partial thromboplastin time to evaluate for a hypercoagulable state See Workup for more detail.
Management
Treatment options for DVT include the following: Anticoagulation (mainstay of therapy): Heparins, warfarin, factor Xa inhibitors, and various emerging anticoagulants Pharmacologic thrombolysis Endovascular and surgical interventions Physical measures (eg, elastic compression stockings and ambulation) Heparin products used in the treatment of DVT include the following: Low-molecular-weight heparin (LMWH; eg, enoxaparin) Unfractionated heparin (UFH) Factor Xa inhibitors used in the treatment of DVT include the following: Fondaparinux The Matisse study found this agent to be comparable to enoxaparin with respect to efficacy and safety[5] Rivaroxaban Rivaroxaban was approved by the US Food and Drug Administration (FDA) for the treatment of DVT or PE and for reduction of the risk of recurrent DVT and PE after initial treatment; data from a pooled analysis of the EINSTEIN-DVT [6] and EINSTEIN-PE [7] trials suggest that rivaroxaban is as effective in preventing VTE recurrence as enoxaparin followed by a vitamin-K antagonist and may be associated with less bleeding [8] ; in addition, the data suggest that there are no grounds for avoiding rivaroxaban use in high-risk groups (eg, fragile patients, cancer patients, and patients with a large clot) Endovascular therapy is performed to reduce the severity and duration of lower-extremity symptoms, prevent PE, diminish the risk of recurrent VTE, and prevent PTS. Percutaneous transcatheter treatment of DVT includes the following: Thrombus removal with catheter-directed thrombolysis American College of Chest Physicians (ACCP) recommends thrombolytic therapy only for patients with massive iliofemoral vein thrombosis associated with limb ischemia or vascular compromise Mechanical thrombectomy Angioplasty Stenting of venous obstructions American Heart Association (AHA) recommendations for inferior vena cava filters include the following[9] : Confirmed acute proximal DVT or acute PE in patients contraindicated for anticoagulation Recurrent thromboembolism while on anticoagulation Active bleeding complications requiring termination of anticoagulation therapy See Treatment and Medication for more detail.
Image library
2 of 27
05/02/2013 6:21
Deep Venous Thrombosis
http://emedicine.medscape.com/article/1911303-overview
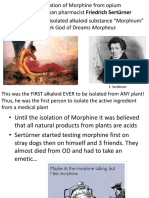
CT venography showing bilateral deep venous thrombosis. Arrows indicate bilateral deep venous thrombosis.
Background
Deep venous thrombosis (DVT) and pulmonary embolism (PE) are manifestations of a single disease entity, namely, venous thromboembolism (VTE). The earliest known reference to peripheral venous disease is found on the Eber papyrus, which dates from 1550 BC and documents the potentially fatal hemorrhage that may ensue from surgery on varicose veins. In 1644, Schenk first observed venous thrombosis when he described an occlusion in the inferior vena cava. In 1846, Virchow recognized the association between venous thrombosis in the legs and PE. DVT is the presence of coagulated blood, a thrombus, in one of the deep venous conduits that return blood to the heart. The clinical conundrum is that symptoms (pain and swelling) are often nonspecific or absent. However, if left untreated, the thrombus may become fragmented or dislodged and migrate to obstruct the arterial supply to the lung, causing potentially life-threatening PE (See Pathophysiology). See the images below.
Venous thrombus.
Pulmonary embolus.
DVT most commonly involves the deep veins of the leg or arm, often resulting in potentially life-threatening emboli to the lungs or debilitating valvular dysfunction and chronic leg swelling. Over the past 25 years, the pathophysiology of DVT has become much better understood, and considerable progress has been made in its diagnosis and treatment. (See Pathophysiology.) DVT is one of the most prevalent medical problems today, with an annual incidence of 80 cases per 100,000. Each year in the United States, more than 200,000 people develop venous thrombosis; of those, 50,000 cases are complicated by PE.[10] Lower-extremity DVT is the most common venous thrombosis, with a prevalence of 1 case per 1000 population. In addition, it is the underlying source of 90% of acute PEs, which cause 25,000 deaths per year in the United States (National Center for Health Statistics [NCHS], 2006). (See Epidemiology.) Conclusive diagnosis has historically required invasive and expensive venography, which is still considered the criterion standard. The diagnosis may also be obtained noninvasively by means of ultrasonographic examination. (See Workup.) Early recognition and appropriate treatment of DVT and its complications can save many lives. (See Treatment and Management.) The goals of pharmacotherapy for DVT are to reduce morbidity, prevent postthrombotic syndrome (PTS), and prevent PE. The primary agents include anticoagulants and thrombolytics. (See Medication.) Other than the immediate threat of PE, the risk of long-term major disability from postthrombotic syndrome is high.[11,
12, 13, 14, 15]
Anatomy
The peripheral venous system functions both as a reservoir to hold extra blood and as a conduit to return blood from the periphery to the heart and lungs. Unlike arteries, which possess 3 well-defined layers (a thin intima, a well-developed muscular media, and a fibrous adventitia), most veins are composed of a single tissue layer. Only the largest veins possess internal elastic membranes, and this layer is thin and unevenly distributed, providing little buttress against high internal pressures. The correct functioning of the venous system depends on a complex series of valves and pumps that are individually frail and prone to malfunction, yet the system as a whole performs remarkably
3 of 27
05/02/2013 6:21
Deep Venous Thrombosis
http://emedicine.medscape.com/article/1911303-overview
well under extremely adverse conditions. Primary collecting veins of the lower extremity are passive, thin-walled reservoirs that are tremendously distensible. Most are suprafascial, surrounded by loosely bound alveolar and fatty tissue that is easily displaced. These suprafascial collecting veins can dilate to accommodate large volumes of blood with little increase in back pressure so that the volume of blood sequestered within the venous system at any moment can vary by a factor of 2 or more without interfering with the normal function of the veins. Suprafascial collecting veins belong to the superficial venous system. Outflow from collecting veins is via secondary conduit veins that have thicker walls and are less distensible. Most of these veins are subfascial and are surrounded by tissues that are dense and tightly bound. These subfascial veins belong to the deep venous system, through which all venous blood must eventually pass through on its way back to the right atrium of the heart. The lower limb deep venous system is typically thought of as 2 separate systems, one below the knee and one above. The calf has 3 groups of paired deep veins: the anterior tibial veins, draining the dorsum of the foot; the posterior tibial veins, draining the sole of the foot; and the peroneal veins, draining the lateral aspect of the foot. Venous sinusoids within the calf muscle coalesce to form soleal and gastrocnemius intramuscular venous plexuses, which join the peroneal veins in the mid calf. These veins play an important role in the muscle pump function of the calf. Just below the knee, these tibial veins join to become the popliteal vein, which too can be paired on occasion. Together, the calfs muscles and deep vein system form a complex array of valves and pumps, often referred to as the peripheral heart, that functions to push blood upward from the feet against gravity. The calf-muscle pump is analogous to the common hand-pump bulb of a sphygmomanometer filling a blood pressure cuff. Before pumping has started, the pressure is neutral and equal everywhere throughout the system and the calf fills with blood, typically 100-150 mL. When the calf contracts, the feeding perforator vein valves are forced closed and the outflow valves are forced open driving the blood proximally. When the calf is allowed to relax, the veins and sinusoids refill from the superficial venous system via perforating veins, and the outflow valve is then forced shut, preventing retrograde flow. With each contraction, 40-60% of the calfs venous volume is driven proximally.[16] The deep veins of the thigh begin distally with the popliteal vein as it courses proximally behind the knee and then passes through the adductor canal, at which point its name changes to the femoral vein. (This important deep vein is sometimes incorrectly referred to as the superficial femoral vein in a misguided attempt to distinguish it from the profunda femoris, or deep femoral vein, a short, stubby vein that usually has its origin in terminal muscle tributaries within the deep muscles of the lateral thigh but may communicate with the popliteal vein in up to 10% of patients. The term superficial femoral vein should never be used, because the femoral vein is in fact a deep vein and is not part of the superficial venous system. This incorrect term does not appear in any definitive anatomic atlas, yet it has come into common use in vascular laboratory practice. Confusion arising from use of the inappropriate name has been responsible for many cases of clinical mismanagement and death.) In theproximal thigh,the femoral vein and the deep femoral vein unite to form the common femoral vein, which passes upwards above the groin crease to become the iliac vein. The external iliac vein is the continuation of the femoral vein as it passes upward behind the inguinal ligament. At the level of the sacroiliac joint, it unites with the hypogastric vein to form the common iliac vein. The left common iliac is longer than the right and more oblique in its course, passing behind the right common iliac artery. This anatomic asymmetry sometimes results in compression of the left common iliac vein by the right common iliac artery to produce May-Thurner syndrome, a left-sided iliac outflow obstruction with localized adventitial fibrosis and intimal proliferation, often with associated deep venous thrombosis. At the level of the fifth lumbar vertebra, the 2 common iliac veins come together at an acute angle to form the inferior vena cava. Please go to the main article on Inferior Vena Caval Thrombosis for more information.
Pathophysiology
Over a century ago, Rudolf Virchow described 3 factors that are critically important in the development of venous thrombosis: (1) venous stasis, (2) activation of blood coagulation, and (3) vein damage. These factors have come to be known as the Virchow triad. Venous stasis can occur as a result of anything that slows or obstructs the flow of venous blood. This results in an increase in viscosity and the formation of microthrombi, which are not washed away by fluid movement; the thrombus that forms may then grow and propagate. Endothelial (intimal) damage in the blood vessel may be intrinsic or secondary to external trauma. It may result from accidental injury or surgical insult. A hypercoagulable state can occur due to a biochemical imbalance between circulating factors. This may result from an increase in circulating tissue activation factor, combined with a decrease in circulating plasma antithrombin and fibrinolysins. Over time, refinements have been made in the description of these factors and their relative importance to the development of venous thrombosis. The origin of venous thrombosis is frequently multifactorial, with components of
4 of 27
05/02/2013 6:21
Deep Venous Thrombosis
http://emedicine.medscape.com/article/1911303-overview
the Virchow triad assuming variable importance in individual patients, but the end result is early thrombus interaction with the endothelium. This interaction stimulates local cytokine production and facilitates leukocyte adhesion to the endothelium, both of which promote venous thrombosis. Depending on the relative balance between activated coagulation and thrombolysis, thrombus propagation occurs. Decreased vein wall contractility and vein valve dysfunction contribute to the development of chronic venous insufficiency. The rise in ambulatory venous pressure causes a variety of clinical symptoms of varicose veins, lower extremity edema, and venous ulceration.
Development of thrombosis
Thrombosis is the homeostatic mechanism whereby blood coagulates or clots, a process crucial to the establishment of hemostasis after a wound. It may be initiated via several pathways, usually consisting of cascading activation of enzymes that magnify the effect of an initial trigger event. A similar complex of events results in fibrinolysis, or the dissolution of thrombi. The balance of trigger factors and enzymes is complex. Microscopic thrombus formation and thrombolysis (dissolution) are continuous events, but with increased stasis, procoagulant factors, or endothelial injury, the coagulation-fibrinolysis balance may favor the pathologic formation of an obstructive thrombus. Clinically relevant deep venous thrombosis is the persistent formation of macroscopic thrombus in the deep proximal veins. For the most part, the coagulation mechanism consists of a series of self-regulating steps that result in the production of a fibrin clot. These steps are controlled by a number of relatively inactive cofactors or zymogens, which, when activated, promote or accelerate the clotting process. These reactions usually occur at the phospholipid surface of platelets, endothelial cells, or macrophages. Generally, the initiation of the coagulation process can be divided into 2 distinct pathways, an intrinsic system and an extrinsic system (see the image below).
Coagulation pathway.
The extrinsic system operates as the result of activation by tissue lipoprotein, usually released as the result of some mechanical injury or trauma. The intrinsic system usually involves circulating plasma factors. Both of these pathways come together at the level of factor X, which is activated to form factor Xa. This in turn promotes the conversion of prothrombin to thrombin (factor II). This is the key step in clot formation, for active thrombin is necessary for the transformation of fibrinogen to a fibrin clot. Once a fibrin clot is formed and has performed its function of hemostasis, mechanisms exist in the body to restore the normal blood flow by lysing the fibrin deposit. Circulating fibrinolysins perform this function. Plasmin digests fibrin and also inactivates clotting factors V and VIII and fibrinogen. Three naturally occurring anticoagulant mechanisms exist to prevent inadvertent activation of the clotting process. These include the heparin-antithrombin III (ATIII), protein C and thrombomodulin protein S, and the tissue factor inhibition pathways. When trauma occurs, or when surgery is performed, circulating ATIII is decreased. This has the effect of potentiating the coagulation process. Studies have demonstrated that levels of circulating ATIII is decreased more, and stay reduced longer, after total hip replacement (THR) than after general surgical cases (see the image below).
Postoperative antithrombin III levels.
Furthermore, patients who have positive venograms postoperatively tend to be those in whom circulating levels of ATIII are diminished (see the image below).
5 of 27
05/02/2013 6:21
Deep Venous Thrombosis
http://emedicine.medscape.com/article/1911303-overview
Antithrombin III levels and deep venous thrombosis formation.
Under normal circumstances, a physiologic balance is present between factors that promote and retard coagulation. A disturbance in this equilibrium may result in the coagulation process occurring at an inopportune time or location or in an excessive manor. Alternatively, failure of the normal coagulation mechanisms may lead to hemorrhage. Thrombus usually forms behind valve cusps or at venous branch points, most of which begin in the calf. Venodilation may disrupt the endothelial cell barrier and expose the subendothelium. Platelets adhere to the subendothelial surface by means of von Willebrand factor or fibrinogen in the vessel wall. Neutrophils and platelets are activated, releasing procoagulant and inflammatory mediators. Neutrophils also adhere to the basement membrane and migrate into the subendothelium. Complexes form of the surface of platelets and increase the rate of thrombin generation and fibrin formation. Stimulated leukocytes irreversibly bind to endothelial receptors and extravasate into the vein wall by means of mural chemotaxis. Because mature thrombus composed of platelets, leukocytes and fibrin develops, and an active thrombotic and inflammatory process occurs at the inner surface of the vein, and an active inflammatory response occurs in the wall of the vein.[17, 18] Studies have shown that low flow sites, such as the soleal sinuses, behind venous valve pockets, and at venous confluences, are at most risk for the development of venous thrombi.[19, 20] However, stasis alone is not enough to facilitate the development of venous thrombosis. Experimental ligation of rabbit jugular veins for periods of up to 60 minutes have failed to consistently cause venous thrombosis.[21, 22] Although, patients that are immobilized for long periods of time seem to be at high risk for the development of venous thrombosis, an additional stimulus is required to develop DVT.
Evolution of venous insufficiency
Over time, thrombus organization begins with the infiltration of inflammatory cells into the clot. This results in a fibroelastic intimal thickening at the site of thrombus attachment in most patients and a fibrous synechiae in up to 11%.[23] In many patients, this interaction between vessel wall and thrombus leads to valvular dysfunction and overall vein wall fibrosis. Histological examination of vein wall remodeling after venous thrombosis has demonstrated an imbalance in connective tissue matrix regulation and a loss of regulatory venous contractility that contributes to the development of chronic venous insufficiency.[24, 25] Some form of chronic venous insufficiency develops in 29-79% of patients with an acute DVT, while ulceration is noted in 4-6%. [26, 27] The risk has been reported to be 6 times greater in those patients with recurrent thrombosis.[28] Over a few months, most acute DVTs evolve to complete or partial recanalization, and collaterals develop (see the images below).[29, 30, 31, 32, 33, 34] Although blood flow may be restored, residual evidence of thrombus or stenosis is observed in half the patients after 1 year. Furthermore, the damage to the underlying valves and those compromised by peripheral dilation and insufficiency usually persists and may progress. Venous stasis, venous reflux, and chronic edema are common in patients who have had a large DVT.[35]
Lower-extremity venogram shows outlining of an acute deep venous thrombosis in the popliteal vein with contrast enhancement.
6 of 27
05/02/2013 6:21
Deep Venous Thrombosis
http://emedicine.medscape.com/article/1911303-overview
Lower-extremity venogram shows a nonocclusive chronic thrombus. The superficial femoral vein (lateral vein) has the appearance of 2 parallel veins, when in fact, it is 1 lumen containing a chronic linear thrombus. Although the chronic clot is not obstructive after it recanalizes, it effectively causes the venous valves to adhere in an open position, predisposing the patient to reflux in the involved segment.
The acute effect of an occluded outflow vein may be minimal if adequate collateral pathways exist. As an alternative, it may produce marked pain and swelling if flow is forced retrograde. In the presence of deep vein outflow obstruction, contraction of the calf muscle produces dilation of the feeding perforating veins, it renders the valves nonfunctional (because the leaflets no longer coapt), and it forces the blood retrograde through the perforator branches and into the superficial system. This high-pressure flow may cause dilation of the superficial (usually low-pressure) system and produce superficial venous incompetence. In clinical terms, the increased incidence of reflux in the ipsilateral greater saphenous vein increases 8.7-fold on follow-up of DVT.[29] This chain of events (ie, obstruction to antegrade flow producing dilation, stasis, further valve dysfunction, with upstream increased pressure, dilation, and other processes) may produce hemodynamic findings of venous insufficiency. Another mechanism that contributes to venous incompetence is the natural healing process of the thrombotic vein. The thrombotic mass is broken down over weeks to months by inflammatory reaction and fibrinolysis, and the valves and venous wall are altered by organization and ingrowth of smooth muscle cells and production of neointima. This process leaves damaged, incompetent, underlying valves, predisposing them to venous reflux. The mural inflammatory reaction breaks down collagen and elastin, leaving a noncompliant venous wall.[29, 30, 31, 32, 33, 34] Persistent obstructive thrombus, coupled with valvular damage, ensures continuation of this cycle. Over time, the venous damage may become irreversible. Hemodynamic venous insufficiency is the underlying pathology of postthrombotic syndrome (PTS), also referred to as postphlebitic syndrome. If numerous valves are affected, flow does not occur centrally unless the leg is elevated. Inadequate expulsion of venous blood results in stasis and a persistently elevated venous pressure or venous hypertension. As fibrin extravasates and inflammation occurs, the superficial tissues become edematous and hyperpigmented. With progression, fibrosis compromises tissue oxygenation, and ulceration may result. After venous insufficiency occurs, no treatment is ideal; elevation and use of compression stockings may compensate, or surgical thrombectomy or venous bypass may be attempted.[36, 37, 38, 39] With anticoagulation alone, as many as 75% of patients with symptomatic DVT present with PTS at 5-10 years. [39, 40] However, the incidence of venous ulceration is far less, at 5%. Of the half million patients with venous ulcers in the United States, 17-45% report having a history of DVT.[41]
Lower-extremity deep venous thrombosis
Most small thrombi in the lower extremities tend to resolve spontaneously after surgery. In about 15% of cases, however, these thrombi may extend into the proximal femoral venous system of the leg. Untreated proximal thrombi represent a significant source of clinically significant pulmonary emboli. In the absence of rhythmic contraction of the leg muscles, as in walking or moving, blood flow in the veins slows and even stops in some areas, predisposing patients to thrombosis.[42] In the postoperative patient, as many as one half of all isolated calf vein thrombi resolve spontaneously within a few hours, whereas approximately 15% extend to involve the femoral vein. A many as one third of untreated symptomatic calf vein DVT extend to the proximal veins.[43] At 1-month follow-up of untreated proximal DVT, 20% regress and 25% propagate. Although calf vein thrombi are rare sources of clinically significant PE, the incidence of PE with untreated proximal thrombi is 29-50%.[44, 43] Most PEs are first diagnosed at autopsy.[45, 46]
Upper-extremity deep venous thrombosis
The 2 forms of upper-extremity DVT are (1) effort-induced thrombosis (Paget-von Schrtter syndrome) and (2) secondary thrombosis. Effort induced thrombosis, or Paget-von Schrtter syndrome, accounts for 25% of cases.[47] Paget in England and von Schrtter in Germany independently described effort thrombosis more than 100 years ago. In this primary form of the disease, an underlying chronic venous compressive abnormality caused by the musculoskeletal structures in the
7 of 27
05/02/2013 6:21
Deep Venous Thrombosis
http://emedicine.medscape.com/article/1911303-overview
costoclavicular space is present at the thoracic inlet and/or outlet. See the images below.
This contrast-enhanced study was obtained through a Mediport placed through the chest wall through the internal jugular vein to facilitate chemotherapy. A thrombus has propagated peripherally from the tip of the catheter in the superior vena cava into both subclavian veins.
Superior vena cava syndrome in a patient with lung cancer. CT scan demonstrates a hypoattenuating thrombus that fills the superior vena cava. The patient was treated with anticoagulation alone.
In 75% of patients with secondary thrombosis, hypercoagulability and/or indwelling central venous catheters are important contributing factors. In fact, with the advent of central venous catheters, upper-extremity and brachiocephalic venous thrombosis has become a more common problem.[48, 49, 50, 51] For more information on upper-extremity DVT, see Imaging in Deep Venous Thrombosis of the Upper Extremity.
Pulmonary embolism
PE develops as venous thrombi break off from their location of origin and travel through the right heart and into the pulmonary artery, causing a ventilation perfusion defect and cardiac strain. PE occurs in approximately 10% of patients with acute DVT and can cause up to 10% of in hospital deaths.[52, 53] However, most patients (up to 75%) are asymptomatic. Traditionally, proximal venous thrombosis are thought to be at highest risk for causing pulmonary emboli; however, the single largest autopsy series ever performed to specifically to look for the source of fatal PE was performed by Havig in 1977, who found that one third of the fatal emboli arose directly from the calf veins.[54]
Etiology
Numerous factors, often in combination, contribute to DVT. These may be categorized as acquired (eg, medication, illness) or congenital (eg, anatomic variant, enzyme deficiency, mutation). A useful categorization may be an acute provoking condition versus a chronic condition, as this distinction affects the length of anticoagulant therapy. The frequent causes of DVT are due to augmentation of venous stasis due to immobilization or central venous obstruction. Immobility can be as transient as that occurring during a transcontinental airplane flight or that during an operation under general anesthesia. It can also be extended, as during hospitalization for pelvic, hip, or spinal surgery, or due to stroke or paraplegia. Individuals in these circumstances warrant surveillance, prophylaxis, and treatment if they develop DVT.[55, 56]
Reduced blood flow from increased blood viscosity or central venous pressure
Increased blood viscosity may decrease venous blood flow. This change may be due to an increase in the cellular component of the blood in polycythemia rubra vera or thrombocytosis or a decrease in the fluid component due to dehydration.
8 of 27
05/02/2013 6:21
Deep Venous Thrombosis
http://emedicine.medscape.com/article/1911303-overview
Increased central venous pressure, either mechanical or functional, may reduce the flow in the veins of the leg. Mass effect on the iliac veins or inferior vena cava from neoplasm, pregnancy, stenosis, or congenital anomaly increases outflow resistance.
Anatomic variants contributing to venous stasis
Anatomic variants that result in diminution or absence of the inferior vena cava or iliac veins may contribute to venous stasis. In iliocaval thromboses, an underlying anatomic contributor is identified in 60-80% of patients. The best-known anomaly is compression of left common iliac vein at the anatomic crossing of the right common iliac artery. The vein normally passes under the right common iliac artery during its normal course. In some individuals, this anatomy results in compression of the left iliac vein and can lead to band or web formation, subsequent stasis, and left leg DVT. The reasons are poorly understood. Compression of the iliac vein is also called May-Thurner syndrome or Cockett syndrome. Inferior vena cava variants are uncommon. Anomalous development is most commonly detected and diagnosed on cross-sectional imaging or venography. The embryologic evolution of the inferior vena cava is from an enlargement or atrophy of paired supracardinal and subcardinal veins. Anomalous embryologic development may result in absence of the normal cava. These variations may increase the risk of symptoms because small-caliber vessels may be most subject to obstruction. In patients younger than 50 years who have deep venous thrombosis, the incidence of a caval anomaly is as high as 5%.[57] A double or duplicated inferior vena cava results from lack of atrophy in part of the left supracardinal vein, resulting in a duplicate structure to the left of the aorta. The common form is a partial paired inferior vena cava that connects the left common iliac and left renal veins. When caval interruption, such as placement of a filter, is planned, these alternate pathways must be considered. As an alternative, the inferior vena cava may not develop. The most common alternate route for blood flow is through the azygous vein, which enlarges to compensate. If a venous stenosis is present at the communication of iliac veins and azygous vein, back pressure can result in insufficiency, stasis, or thrombosis.[58] In rare cases, neither the inferior vena cava nor the azygous vein develops, and the iliac veins drain through internal iliac collaterals to the hemorrhoidal veins and superior mesenteric vein to the portal system of the liver. Hepatic venous drainage to the atrium is patent. Because this pathway involves small hemorrhoidal vessels, thrombosis of these veins can cause severe acute swelling of the legs. Thrombosis of the inferior vena cava is a rare occurrence and is an unusual result of leg deep venous thrombosis unless an inferior vena cava filter is present and stops a large embolus in the cava, resulting in obstruction and extension of thrombosis. Common causes of caval thrombosis include tumors involving the kidney or liver, tumors invading the inferior vena cava, compression of the inferior vena cava by extrinsic mass, and retroperitoneal fibrosis.[59, 60]
Mechanical injury to vein
Mechanical injury to the vein wall appears to provide an added stimulus for venous thrombosis. Hip arthroplasty patients with the associated femoral vein manipulation represent a high-risk group that cannot be explained by just immobilization, with 57% of thrombi originating in the affected femoral vein rather than the usual site of stasis in the calf.[61] Endothelial injury can convert the normally antithrombogenic endothelium to become prothrombotic by stimulating the production of tissue factor, von Willebrand factor, and fibronectin. Injury may be obvious, such as those due to trauma, surgical intervention, or iatrogenic injury, but they may also be obscure, such as those due to remote deep venous thrombosis (perhaps asymptomatic) or minor (forgotten) trauma. Previous DVT is a major risk factor for further DVT. The increased incidence of DVT in the setting of acute urinary tract or respiratory infection may be due to an inflammation-induced alteration in endothelial function.
Common risk factors for deep venous thrombosis
The presence of risk factors plays a prominent role in the assessing the pretest probability of DVT. Furthermore, transient risk factors permit successful short-term anticoagulation, whereas idiopathic deep venous thrombosis or chronic or persistent risk factors warrant long-term therapy. In the MEDENOX study that evaluated 1102 acutely ill, immobilized admitted general medical patients, multiple logistic regression analysis found the following factors to be significantly and independently associated with an increased risk for VTE, most of which were asymptomatic and diagnosed by venography of both lower extremities[62] : Presence of an acute infectious disease Age older than 75 years Cancer History of prior VTE
9 of 27
05/02/2013 6:21
Deep Venous Thrombosis
http://emedicine.medscape.com/article/1911303-overview
The most common risk factors are obesity, previous VTE, malignancy, surgery, and immobility. Each is found in 20-30% of patients. Hospitalized and nursing home patients often have several risk factors and account for one half of all DVT (with an incidence of 1 case per 100 population).[45, 63] The single most powerful risk marker remains a prior history of DVT with as many as 25% of acute venous thrombosis occurring in such patients.[64] Pathologically, remnants of previous thrombi are often seen within the specimens of new acute thrombi. However, recurrent thrombosis may actually be the result of primary hypercoagulable states. Abnormalities within the coagulation cascade are the direct result of discrete genetic mutations within the coagulation cascade. Deficiencies of protein C, protein S, or antithrombin III account for approximately 5-10% of all cases of DVT.[65] Age has been well studied as an independent risk factor for venous thrombosis development. Although a 30-fold increase in incidence is noted from age 30 to age 80, the effect appears to be multifactorial, with more thrombogenic risk factors occurring in the elderly than in those younger than 40 years.[64, 66] Venous stasis, as seen in immobilized patients and paralyzed limbs, also contributes to the development of venous thrombosis. Autopsy studies parallel the duration of bed rest to the incidence of venous thrombosis, with 15% of patients in those studies dying within 7 days of bedrest to greater than 80% in those dying after 12 weeks.[19] Within stroke patients, DVT is found in 53% of paralyzed limbs, compared with only 7% on the nonaffected side.[67] Malignancy is noted in as many as 30% of patients with venous thrombosis.[64, 68] The thrombogenic mechanisms involve abnormal coagulation, as evidenced by 90% of cancer patients having some abnormal coagulation factors.[69] Chemotherapy may increase the risk of venous thrombosis by affecting the vascular endothelium, coagulation cascades, and tumor cell lysis. The incidence has been shown to increase in those patients undergoing longer courses of therapy for breast cancer, from 4.9% for 12 weeks of treatment to 8.8% for 36 weeks.[70] Additionally, DVT complicates 29% of surgical procedures done for malignancy.[71] Postoperative venous thrombosis varies depending on a multitude of patient factors, including the type of surgery undertaken. Without prophylaxis, general surgery operations typically have an incidence of DVT around 20%, whereas orthopedic hip surgery can occur in up to 50% of patients.[72] The nature of orthopedic illnesses and diseases, trauma, and surgical repair or replacement of hip and knee joints predisposes patients to the occurrence of VTE disease. These complications are predictable and are the result of alterations of the natural equilibrium mechanisms in various disease states.[73] For more information, see Deep Venous Thrombosis Prophylaxis. Based on radioactive labeled fibrinogen, about half of lower extremity thrombi develop intraoperatively.[74] Perioperative immobilization, coagulation abnormalities, and venous injury all contribute to the development of surgical venous thrombosis.
Genetic factors
Genetic mutations within the bloods coagulation cascade represent those at highest risk for the development of venous thrombosis. Genetic thrombophilia is identified in 30% of patients with idiopathic venous thrombosis. Primary deficiencies of coagulation inhibitors antithrombin, protein C, and protein S are associated with 5-10% of all thrombotic events.[75, 76, 77] Altered procoagulant enzyme proteins include factor V, factor VIII, factor IX, factor XI, and prothrombin. Resistance of procoagulant factors to an intact anticoagulation system has also recently been described with the recognition of factor V Leiden mutation, representing 10-65% of patients with DVT.[78] In the setting of venous stasis, these factors are allowed to accumulate in thrombosis prone sites, where mechanical vessel injury has occurred, stimulating the endothelium to become prothrombotic.[79] Factor V Leiden is a mutation that results in a form of factor Va that resists degradation by activated protein C, leading to a hypercoagulable state. Its importance lies in the 5% prevalence in the American population and its association with a 3-fold to 6-fold increased risk for VTE. Antiphospholipid syndrome is considered a disorder of the immune system, where antiphospholipid antibodies (cardiolipin or lupus anticoagulant antibodies) are associated with a syndrome of hypercoagulability. Although not a normal blood component, the antiphospholipid antibody may be asymptomatic. It is present in 2% of the population, and it may be detected in association with infections or the administration of certain drugs, including antibiotics, cocaine, hydralazine, procainamide, and quinine.[76] Tests for these genetic defects are often not performed in patients with recurrent venous thrombosis because therapy remains symptomatic. In most patients with these genetic defects, lifetime anticoagulation therapy with warfarin or low molecular weight heparin (LMWH) is recommended after recurrent DVT without an alternative identifiable etiology documented. The risk of recurrent DVT is multiplied 1.4-2 times, with the most common genetic polymorphisms predisposing individuals to DVT. However, the low incidence of factor V Leiden and prothrombin G20210A may not warrant aggressive prophylaxis. Therefore, genetic testing might not be warranted until a second event occurs.[80]
Other conditions that can induce hypercoagulability
10 of 27
05/02/2013 6:21
Deep Venous Thrombosis
http://emedicine.medscape.com/article/1911303-overview
Other diseases and states can induce hypercoagulability in patients without other underlying risks for DVT. They can predispose patients to DVT, though their ability to cause DVT without intrinsic hypercoagulability is in question. The conditions include malignancy, dehydration, and use of medications (eg, estrogens). Acute hypercoagulable states also occur, as in disseminated intravascular coagulopathy (DIC) resulting from infection or heparin-induced thrombocytopenia.[81]
Summary of risk factors
A summary of risk factors is as follows: Age Immobilization longer than 3 days Pregnancy and the postpartum period Major surgery in previous 4 weeks Long plane or car trips (>4 h) in previous 4 weeks Cancer Previous DVT Stroke Acute myocardial infarction (AMI) Congestive heart failure (CHF) Sepsis Nephrotic syndrome Ulcerative colitis Multiple trauma CNS/spinal cord injury Burns Lower extremity fractures Systemic lupus erythematosus (SLE) and the lupus anticoagulant Behet syndrome Homocystinuria Polycythemia rubra vera Thrombocytosis Inherited disorders of coagulation/fibrinolysis Antithrombin III deficiency Protein C deficiency Protein S deficiency Prothrombin 20210A mutation Factor V Leiden Dysfibrinogenemias and disorders of plasminogen activation Intravenous (IV) drug abuse Oral contraceptives Estrogens Heparin-induced thrombocytopenia (HIT)
Epidemiology
DVT and thromboembolism remain a common cause of morbidity and mortality in bedridden or hospitalized patients, as well as generally healthy individuals. The exact incidence of DVT is unknown because most studies are limited by the inherent inaccuracy of clinical diagnosis. Existing data that probably underestimate the true incidence of DVT suggest that about 80 cases per 100,000 population occur annually. Approximately 1 person in 20 develops a DVT in the course of his or her lifetime. About 600,000 hospitalizations per year occur for DVT in the United States. In elderly persons, the incidence is increased 4-fold. The in-hospital case-fatality rate for VTE is 12%, rising to 21% in elderly persons. In hospitalized patients, the incidence of venous thrombosis is considerably higher and varies from 20-70%. Venous ulceration and venous insufficiency of the lower leg, which are long-term complications of DVT, affect 0.5% of the entire population. Extrapolation of these data reveals that as many as 5 million people have venous stasis and varying degrees of venous insufficiency.
Age distribution for deep venous thrombosis
Deep venous thrombosis usually affects individuals older than 40 years. The incidence of VTE increases with age in both sexes. The age-standardized incidence of first-time VTE is 1.92 per 1000 person-years.
Prevalence of deep venous thrombosis by sex
The male-to-female ratio is 1.2:1, indicating that males have a higher risk of DVT than females.
11 of 27
05/02/2013 6:21
Deep Venous Thrombosis
http://emedicine.medscape.com/article/1911303-overview
Prevalence of deep venous thrombosis by race
From a demographic viewpoint, Asian and Hispanic populations have a lower risk of VTE, whereas whites and blacks have a higher risk (2.5-4 times higher).
Prognosis
Most DVT is occult and usually resolves spontaneously without complication. The principal long-term morbidity from DVT is PTS, which complicates about a quarter of cases of symptomatic proximal DVT; most cases develop within 2 years afterward. Death from DVT is attributed to massive PE, which causes as many as 300,000 deaths annually in the United States.[82] PE is the leading cause of preventable in-hospital mortality. The Longitudinal Investigation of Thromboembolism Etiology (LITE) that combined data from two prospective cohort studies, the Atherosclerosis Risk in Communities (ARIC) and the Cardiovascular Health Study (CHS) determined the incidence of symptomatic DVT and pulmonary embolism in 21,680 participants aged 45 years or older who were followed for 7.6 years.[83]
Patient Education
For excellent patient education resources, visit eMedicineHealths Lung and Airway Center. Also, see eMedicineHealths patient education articles Blood Clot in the Legs, Deep Vein Thrombosis (Blood Clot in the Leg, DVT), Phlebitis, and Pulmonary Embolism.
Contributor Information and Disclosures
Author Kaushal (Kevin) Patel, MD Vascular Surgeon, Kaiser Permanente Los Angeles Medical Center Disclosure: Nothing to disclose. Coauthor(s) Linda J Chun, MD Resident Physician, Department of Surgery, Los Angeles Medical Center, Kaiser Permanente Disclosure: Nothing to disclose. Chief Editor Barry E Brenner, MD, PhD, FACEP Professor of Emergency Medicine, Professor of Internal Medicine, Program Director for Emergency Medicine, Case Medical Center, University Hospitals, Case Western Reserve University School of Medicine Barry E Brenner, MD, PhD, FACEP is a member of the following medical societies: Alpha Omega Alpha, American Academy of Emergency Medicine, American College of Chest Physicians, American College of Emergency Physicians, American College of Physicians, American Heart Association, American Thoracic Society, Arkansas Medical Society, New York Academy of Medicine, New York Academy of Sciences, and Society for Academic Emergency Medicine Disclosure: Nothing to disclose. Additional Contributors Marc D Basson, MD, PhD, MBA, FACS Professor, Chair, Department of Surgery, Assistant Dean for Faculty Development in Research, Michigan State University College of Human Medicine Marc D Basson, MD, PhD, MBA, FACS is a member of the following medical societies: Alpha Omega Alpha, American College of Surgeons, American Gastroenterological Association, Phi Beta Kappa, and Sigma Xi
12 of 27
05/02/2013 6:21
Deep Venous Thrombosis
http://emedicine.medscape.com/article/1911303-overview
Disclosure: Nothing to disclose. John J Borsa, MD Consulting Staff, Department of Radiology, St Joseph Medical Center John J Borsa, MD is a member of the following medical societies: American College of Radiology, American Society of Neuroradiology, Cardiovascular and Interventional Radiological Society of Europe, Radiological Society of North America, Royal College of Physicians and Surgeons of Canada, and Society of Interventional Radiology Disclosure: Nothing to disclose. Hearns W Charles, MD Assistant Professor of Radiology, New York University School of Medicine; Attending Physician, Division of Vascular and Interventional Radiology, Department of Radiology, New York University Medical Center Hearns W Charles, MD is a member of the following medical societies: American College of Radiology, American Roentgen Ray Society, Radiological Society of North America, and Society of Cardiovascular and Interventional Radiology Disclosure: Nothing to disclose. Kyung J Cho, MD, FACR William Martel Professor of Radiology, Interventional Radiology Fellowship Director, University of Michigan Health System Kyung J Cho, MD, FACR is a member of the following medical societies: American College of Radiology, American Heart Association, American Medical Association, American Roentgen Ray Society, Association of University Radiologists, and Radiological Society of North America Disclosure: Nothing to disclose. Douglas M Coldwell, MD, PhD Professor of Radiology, Director, Division of Vascular and Interventional Radiology, University of Louisville School of Medicine Douglas M Coldwell, MD, PhD is a member of the following medical societies: American Association for Cancer Research, American College of Radiology, American Heart Association, American Physical Society, American Roentgen Ray Society, Society of Cardiovascular and Interventional Radiology, Southwest Oncology Group, and Special Operations Medical Association Disclosure: Sirtex, Inc. Consulting fee Speaking and teaching; DFINE, Inc. Honoraria Consulting Francis Counselman, MD, FACEP Chair, Professor, Department of Emergency Medicine, Eastern Virginia Medical School Francis Counselman, MD, FACEP is a member of the following medical societies: Alpha Omega Alpha, American College of Emergency Physicians, Association of Academic Chairs of Emergency Medicine (AACEM), Norfolk Academy of Medicine, and Society for Academic Emergency Medicine Disclosure: Nothing to disclose. Paul E Di Cesare, MD, FACS Professor and Chair, Department of Orthopedic Sugery, University of California, Davis, School of Medicine Paul E Di Cesare, MD, FACS is a member of the following medical societies: American Academy of Orthopaedic Surgeons, American College of Surgeons, and Sigma Xi Disclosure: Stryker Consulting fee Consulting Robert S Ennis, MD, FACS Associate Professor, Department of Orthopedic Surgery, University of Miami School of Medicine; President, OrthoMed Consulting Services, Inc Robert S Ennis, MD, FACS is a member of the following medical societies: American Academy of Orthopaedic Surgeons, American College of Surgeons, and Florida Orthopaedic Society Disclosure: Nothing to disclose. Craig F Feied, MD, FACEP, FAAEM, FACPh Professor of Emergency Medicine, Georgetown University School of Medicine; General Manager, Microsoft Enterprise Health Solutions Group Disclosure: Nothing to disclose. Luis G Fernandez, MD, KHS, FACS, FASAS, FCCP, FCCM, FICS Assistant Clinical Professor of Surgery and Family Practice, University of Texas Health Science Center; Adjunct Clinical Professor of Medicine and Nursing, University of Texas, Arlington; Chairman, Division of Trauma Surgery and Surgical Critical Care, Chief of Trauma
13 of 27
05/02/2013 6:21
Deep Venous Thrombosis
http://emedicine.medscape.com/article/1911303-overview
Surgical Critical Care Unit, Trinity Mother Francis Health System; Brigadier General, Texas Medical Rangers, TXSG/MB Luis G Fernandez, MD, KHS, FACS, FASAS, FCCP, FCCM, FICS is a member of the following medical societies: American Association for the Surgery of Trauma, American College of Chest Physicians, American College of Legal Medicine, American College of Surgeons, American Society of Abdominal Surgeons, American Society of General Surgeons, American Society of General Surgeons, American Society of Law, Medicine & Ethics, American Trauma Society, Association for SurgicalEducation, Association of Military Surgeons of the US, Chicago Medical Society, Illinois State Medical Society, International College of Surgeons, New York Academy of Sciences, Pan American Trauma Society, Society of Critical Care Medicine, Society of Laparoendoscopic Surgeons, Southeastern Surgical Congress, Texas Medical Association, and Undersea and Hyperbaric Medical Society Disclosure: Nothing to disclose. Douglas M Geehan, MD Associate Professor, Department of Surgery, University of Missouri at Kansas City Douglas M Geehan, MD is a member of the following medical societies: American College of Surgeons, American Institute of Ultrasound in Medicine, American Medical Association, Association for Academic Surgery, Phi Beta Kappa, Society of American Gastrointestinal and Endoscopic Surgeons, and Society of Critical Care Medicine Disclosure: Nothing to disclose. John Geibel, MD, DSc, MA Vice Chair and Professor, Department of Surgery, Section of Gastrointestinal Medicine, and Department of Cellular and Molecular Physiology, Yale University School of Medicine; Director, Surgical Research, Department of Surgery, Yale-New Haven Hospital John Geibel, MD, DSc, MA is a member of the following medical societies: American Gastroenterological Association, American Physiological Society, American Society of Nephrology, Association for Academic Surgery, International Society of Nephrology, New York Academy of Sciences, and Society for Surgery of the Alimentary Tract Disclosure: AMGEN Royalty Consulting; ARdelyx Ownership interest Board membership Harris Gellman, MD Consulting Surgeon, Broward Hand Center; Voluntary Clinical Professor of Orthopedic Surgery and Plastic Surgery, Departments of Orthopedic Surgery and Surgery, University of Miami, Leonard M Miller School of Medicine Harris Gellman, MD is a member of the following medical societies: American Academy of Medical Acupuncture, American Academy of Orthopaedic Surgeons, American Orthopaedic Association, American Society for Surgery of the Hand, and Arkansas Medical Society Disclosure: Nothing to disclose. Craig Greben, MD Assistant Professor of Radiology, Hofstra University School of Medicine; Chief, Division of Vascular and Interventional Radiology, North Shore University Hospital Craig Greben, MD is a member of the following medical societies: Society of Cardiovascular and Interventional Radiology Disclosure: Nothing to disclose. Lars Grimm, MD, MHS House Staff, Department of Diagnostic Radiology, Duke University Medical Center Disclosure: Nothing to disclose. Michael A Grosso, MD Consulting Staff, Department of Cardiothoracic Surgery, St Francis Hospital Michael A Grosso, MD is a member of the following medical societies: American College of Surgeons, Society of Thoracic Surgeons, and Society of University Surgeons Disclosure: Nothing to disclose. George Hartnell, MBChB Professor of Radiology, Tufts University School of Medicine; Director of Cardiovascular and Interventional Radiology, Department of Radiology, Baystate Medical Center George Hartnell, MBChB is a member of the following medical societies: American College of Cardiology, American College of Radiology, American Heart Association, Association of University Radiologists, British Institute of Radiology, British Medical Association, Massachusetts Medical Society, Radiological Society of North America, Royal College of Physicians, Royal College of Radiologists, andSociety of Cardiovascular and Interventional Radiology
14 of 27
05/02/2013 6:21
Deep Venous Thrombosis
http://emedicine.medscape.com/article/1911303-overview
Disclosure: Nothing to disclose. Eric K Hoffer, MD Director, Vascular and Interventional Radiology, Associate Professor of Radiology, Section of Angiography and Interventional Radiology, Dartmouth-Hitchcock Medical Center Eric K Hoffer, MD is a member of the following medical societies: American Heart Association, Radiological Society of North America, Society for Cardiac Angiography and Interventions, and Society of Interventional Radiology Disclosure: Nothing to disclose. James Quan-Yu Hwang, MD, RDMS, RDCS, FACEP Staff Physician, Emergency Department, Kaiser Permanente James Quan-Yu Hwang, MD, RDMS, RDCS, FACEP is a member of the following medical societies: American Academy of Emergency Medicine, American College of Emergency Physicians, American Institute of Ultrasound in Medicine, and Society for Academic Emergency Medicine Disclosure: 3rd Rock Ultrasound, LLC Salary Speaking and teaching; Schlesinger Associates Consulting fee Consulting; Philips Ultrasound Consulting fee Consulting Bartholomew Kwan, MBBS, FRCPC, FRCR Staff Radiologist, Department of Medical Imaging, WOHC Brampton Civic Hospital Bartholomew Kwan, MBBS, FRCPC, FRCR is a member of the following medical societies: American Roentgen Ray Society, Cardiovascular and Interventional Radiological Society of Europe, Radiological Society of North America, Royal College of Physicians and Surgeons of Canada, Royal College of Radiologists, and Society of Interventional Radiology Disclosure: Nothing to disclose. William C Manson, MD Director of Emergency Ultrasound, Department of Emergency Medicine, Emory University School of Medicine William C Manson, MD is a member of the following medical societies: American College of Emergency Physicians, American Institute of Ultrasound in Medicine, Emergency Medicine Residents Association, and Society for Academic Emergency Medicine Disclosure: The Emergency Ultrasound Course Honoraria Speaking and teaching Girish R Mood, MBBS, MD, MRCS Fellow, Department of Vascular Medicine, Cleveland Clinic Foundation Disclosure: Nothing to disclose. James Naidich, MD Residency Director, North Shore University Hospital; Professor, Department of Radiology, New York University School of Medicine Disclosure: Nothing to disclose. Jason J Naidich, MD Assistant Professor of Radiology, New York University School of Medicine; Attending Physician, Division of Vascular and Interventional Radiology, North Shore University Hospital Disclosure: Nothing to disclose. Vincent Lopez Rowe, MD Associate Professor of Surgery, Department of Surgery, Division of Vascular Surgery, University of Southern California Medical Center Vincent Lopez Rowe, MD is a member of the following medical societies: American College of Surgeons, American Heart Association, Pacific Coast Surgical Association, Peripheral Vascular Surgery Society, Society for Clinical Vascular Surgery, Society for Vascular Surgery, and Western Vascular Surgical Society Disclosure: Nothing to disclose. Miguel A Schmitz, MD Consulting Surgeon, Department of Orthopedics, Klamath Orthopedic and Sports Medicine Clinic Miguel A Schmitz, MD is a member of the following medical societies: American Academy of Orthopaedic Surgeons, American Orthopaedic Society for Sports Medicine, Arthroscopy Association of North America, and North American Spine Society Disclosure: Nothing to disclose. Donald Schreiber, MD, CM Associate Professor of Surgery (Emergency Medicine), Stanford University School of
15 of 27
05/02/2013 6:21
Deep Venous Thrombosis
http://emedicine.medscape.com/article/1911303-overview
Medicine Donald Schreiber, MD, CM is a member of the following medical societies: American College of Emergency Physicians Disclosure: Abbott Point of Care Inc Research Grant and Speakers Bureau Speaking and teaching; Nanosphere Inc Grant/research funds Research; Singulex Inc Grant/research funds Research; Abbott Diagnostics Inc Grant/research funds None William A Schwer, MD Professor, Department of Family Medicine, Rush Medical College; Chairman, Department of Family Medicine, Rush-Presbyterian-St Luke's Medical Center William A Schwer, MD is a member of the following medical societies: American Academy of Family Physicians Disclosure: Nothing to disclose. Gary Setnik, MD Chair, Department of Emergency Medicine, Mount Auburn Hospital; Assistant Professor, Division of Emergency Medicine, Harvard Medical School Gary Setnik, MD is a member of the following medical societies: American College of Emergency Physicians, National Association of EMS Physicians, and Society for Academic Emergency Medicine Disclosure: SironaHealth Salary Management position; South Middlesex EMS Consortium Salary Management position; ProceduresConsult.com Royalty Other Gary P Siskin, MD Professor and Chairman, Department of Radiology, Albany Medical College Gary P Siskin, MD is a member of the following medical societies: American College of Radiology, Cardiovascular and Interventional Radiological Society of Europe, Radiological Society of North America, and Society of Interventional Radiology Disclosure: Nothing to disclose. Francisco Talavera, PharmD, PhD Adjunct Assistant Professor, University of Nebraska Medical Center College of Pharmacy; Editor-in-Chief, Medscape Drug Reference Disclosure: Medscape Salary Employment Wai Hong Wilson Tang, MD Associate Professor of Medicine, Section of Heart Failure and Cardiac Transplantation Medicine, Cleveland Clinic Foundation Wai Hong Wilson Tang, MD is a member of the following medical societies: American College of Cardiology, American Heart Association, Heart Failure Society of America, and International Society for Heart and Lung Transplantation Disclosure: Abbott Laboratories Grant/research funds Research Supplies; Medtronic Inc Consulting fee Consulting; St Jude Medical Consulting fee Consulting Anthony Watkinson, MD Professor of Interventional Radiology, The Peninsula Medical School; Consultant and Senior Lecturer, Department of Radiology, The Royal Devon and Exeter Hospital, UK Anthony Watkinson, MD is a member of the following medical societies: Radiological Society of North America, Royal College of Radiologists, and Royal College of Surgeons of England Disclosure: Nothing to disclose.
References
1. Haeger K. Problems of acute deep venous thrombosis. I. The interpretation of signs and symptoms. Angiology. Apr 1969;20(4):219-23. [Medline]. 2. MCLACHLIN J, RICHARDS T, PATERSON JC. An evaluation of clinical signs in the diagnosis of venous thrombosis. Arch Surg. Nov 1962;85:738-44. [Medline]. 3. Meignan M, Rosso J, Gauthier H, Brunengo F, Claudel S, Sagnard L, et al. Systematic lung scans reveal a high frequency of silent pulmonary embolism in patients with proximal deep venous thrombosis. Arch Intern Med. Jan 24 2000;160(2):159-64. [Medline]. 4. [Guideline] Snow V, Qaseem A, Barry P, Hornbake ER, Rodnick JE, Tobolic T, et al. Management of venous thromboembolism: a clinical practice guideline from the American College of Physicians and the American
16 of 27
05/02/2013 6:21
Deep Venous Thrombosis
http://emedicine.medscape.com/article/1911303-overview
Academy of Family Physicians. Ann Intern Med. Feb 6 2007;146(3):204-10. [Medline]. 5. Bller HR, Ten Cate-Hoek AJ, Hoes AW, Joore MA, Moons KG, Oudega R, et al. Safely ruling out deep venous thrombosis in primary care. Ann Intern Med. Feb 17 2009;150(4):229-35. [Medline]. 6. Bauersachs R, Berkowitz SD, Brenner B, Buller HR, Decousus H, Gallus AS, et al. Oral rivaroxaban for symptomatic venous thromboembolism. N Engl J Med. Dec 23 2010;363(26):2499-510. [Medline]. [Full Text]. 7. Bller HR, Prins MH, Lensin AW, Decousus H, Jacobson BF, Minar E, et al. Oral rivaroxaban for the treatment of symptomatic pulmonary embolism. N Engl J Med. Apr 5 2012;366(14):1287-97. [Medline]. [Full Text]. 8. Hughes S. Rivaroxaban stands up to standard anticoagulation for VTE treatment. Medscape Medical News. Dec 13, 2012;Accessed January 10, 2013. Available at http://www.medscape.com/viewarticle/776147. 9. Jaff MR, McMurtry MS, Archer SL, Cushman M, Goldenberg N, Goldhaber SZ, et al. Management of Massive and Submassive Pulmonary Embolism, Iliofemoral Deep Vein Thrombosis, and Chronic Thromboembolic Pulmonary Hypertension: A Scientific Statement From the American Heart Association. Circulation. Apr 26 2011;123(16):1788-1830. [Medline]. 10. Silverstein MD, Heit JA, Mohr DN, Petterson TM, O'Fallon WM, Melton LJ 3rd. Trends in the incidence of deep vein thrombosis and pulmonary embolism: a 25-year population-based study. Arch Intern Med. Mar 23 1998;158(6):585-93. [Medline]. 11. Useche JN, de Castro AM, Galvis GE, Mantilla RA, Ariza A. Use of US in the evaluation of patients with symptoms of deep venous thrombosis of the lower extremities. Radiographics. Oct 2008;28(6):1785-97. [Medline]. 12. Chang R, Chen CC, Kam A, Mao E, Shawker TH, Horne MK 3rd. Deep vein thrombosis of lower extremity: direct intraclot injection of alteplase once daily with systemic anticoagulation--results of pilot study. Radiology. Feb 2008;246(2):619-29. [Medline]. 13. Biuckians A, Meier GH 3rd. Treatment of symptomatic lower extremity acute deep venous thrombosis: role of mechanical thrombectomy. Vascular. Sep-Oct 2007;15(5):297-303. [Medline]. 14. Li W, Salanitri J, Tutton S, Dunkle EE, Schneider JR, Caprini JA, et al. Lower extremity deep venous thrombosis: evaluation with ferumoxytol-enhanced MR imaging and dual-contrast mechanism--preliminary experience. Radiology. Mar 2007;242(3):873-81. [Medline]. 15. [Best Evidence] Kakkos SK, Caprini JA, Geroulakos G, Nicolaides AN, Stansby GP, Reddy DJ. Combined intermittent pneumatic leg compression and pharmacological prophylaxis for prevention of venous thromboembolism in high-risk patients. Cochrane Database Syst Rev. Oct 8 2008;CD005258. [Medline]. 16. Araki CT, Back TL, Padberg FT, Thompson PN, Jamil Z, Lee BC, et al. The significance of calf muscle pump function in venous ulceration. J Vasc Surg. Dec 1994;20(6):872-7; discussion 878-9. [Medline]. 17. Wakefield TW, Strieter RM, Schaub R, Myers DD, Prince MR, Wrobleski SK, et al. Venous thrombosis prophylaxis by inflammatory inhibition without anticoagulation therapy. J Vasc Surg. Feb 2000;31(2):309-24. [Medline]. 18. Wakefield TW, Proctor MC. Current status of pulmonary embolism and venous thrombosis prophylaxis. Semin Vasc Surg. Sep 2000;13(3):171-81. [Medline]. 19. GIBBS NM. Venous thrombosis of the lower limbs with particular reference to bed-rest. Br J Surg. Nov 1957;45(191):209-36. [Medline]. 20. Sevitt S. The structure and growth of valve-pocket thrombi in femoral veins. J Clin Pathol. Jul 1974;27(7):517-28. [Medline]. [Full Text]. 21. Aronson DL, Thomas DP. Experimental studies on venous thrombosis: effect of coagulants, procoagulants and vessel contusion. Thromb Haemost. Dec 17 1985;54(4):866-70. [Medline]. 22. WESSLER S, REIMER SM, SHEPS MC. Biologic assay of a thrombosis-inducing activity in human serum. J Appl Physiol. Nov 1959;14:943-6. [Medline]. 23. Sevitt S. The mechanisms of canalisation in deep vein thrombosis. J Pathol. Jun 1973;110(2):153-65. [Medline]. 24. Gandhi RH, Irizarry E, Nackman GB, Halpern VJ, Mulcare RJ, Tilson MD. Analysis of the connective tissue matrix and proteolytic activity of primary varicose veins. J Vasc Surg. Nov 1993;18(5):814-20. [Medline].
17 of 27
05/02/2013 6:21
Deep Venous Thrombosis
http://emedicine.medscape.com/article/1911303-overview
25. Rizzi A, Quaglio D, Vasquez G, Mascoli F, Amadesi S, Cal G, et al. Effects of vasoactive agents in healthy and diseased human saphenous veins. J Vasc Surg. Nov 1998;28(5):855-61. [Medline]. 26. Monreal M, Martorell A, Callejas JM, Valls R, Llamazares JF, Lafoz E, et al. Venographic assessment of deep vein thrombosis and risk of developing post-thrombotic syndrome: a prospective study. J Intern Med. Mar 1993;233(3):233-8. [Medline]. 27. Strandness DE Jr, Langlois Y, Cramer M, Randlett A, Thiele BL. Long-term sequelae of acute venous thrombosis. JAMA. Sep 9 1983;250(10):1289-92. [Medline]. 28. Prandoni P, Lensing AW, Cogo A, Cuppini S, Villalta S, Carta M, et al. The long-term clinical course of acute deep venous thrombosis. Ann Intern Med. Jul 1 1996;125(1):1-7. [Medline]. 29. Meissner MH, Caps MT, Zierler BK, Bergelin RO, Manzo RA, Strandness DE Jr. Deep venous thrombosis and superficial venous reflux. J Vasc Surg. Jul 2000;32(1):48-56. [Medline]. 30. Meissner MH, Caps MT, Zierler BK, Polissar N, Bergelin RO, Manzo RA, et al. Determinants of chronic venous disease after acute deep venous thrombosis. J Vasc Surg. Nov 1998;28(5):826-33. [Medline]. 31. Meissner MH, Manzo RA, Bergelin RO, Markel A, Strandness DE Jr. Deep venous insufficiency: the relationship between lysis and subsequent reflux. J Vasc Surg. Oct 1993;18(4):596-605; discussion 606-8. [Medline]. 32. Caps MT, Manzo RA, Bergelin RO, Meissner MH, Strandness DE Jr. Venous valvular reflux in veins not involved at the time of acute deep vein thrombosis. J Vasc Surg. Nov 1995;22(5):524-31. [Medline]. 33. Johnson BF, Manzo RA, Bergelin RO, Strandness DE Jr. Relationship between changes in the deep venous system and the development of the postthrombotic syndrome after an acute episode of lower limb deep vein thrombosis: a one- to six-year follow-up. J Vasc Surg. Feb 1995;21(2):307-12; discussion 313. [Medline]. 34. Johnson BF, Manzo RA, Bergelin RO, Strandness DE Jr. The site of residual abnormalities in the leg veins in long-term follow-up after deep vein thrombosis and their relationship to the development of the post-thrombotic syndrome. Int Angiol. Mar 1996;15(1):14-9. [Medline]. 35. Haenen JH, Wollersheim H, Janssen MC, Van 't Hof MA, Steijlen PM, van Langen H, et al. Evolution of deep venous thrombosis: a 2-year follow-up using duplex ultrasound scan and strain-gauge plethysmography. J Vasc Surg. Oct 2001;34(4):649-55. [Medline]. 36. Andriopoulos A, Wirsing P, Btticher R. Results of iliofemoral venous thrombectomy after acute thrombosis: report on 165 cases. J Cardiovasc Surg (Torino). Mar-Apr 1982;23(2):123-4. [Medline]. 37. Zheng Y, Zhou B, Pu X. [Frequency of protein C polymorphisms in Chinese population and thrombotic patients]. Zhonghua Yi Xue Za Zhi. Mar 1998;78(3):210-2. [Medline]. 38. Juhan C, Alimi Y, Di Mauro P, Hartung O. Surgical venous thrombectomy. Cardiovasc Surg. Oct 1999;7(6):586-90. [Medline]. 39. Saarinen J, Kallio T, Lehto M, Hiltunen S, Sisto T. The occurrence of the post-thrombotic changes after an acute deep venous thrombosis. A prospective two-year follow-up study. J Cardiovasc Surg (Torino). Jun 2000;41(3):441-6. [Medline]. 40. Elliott G. Thrombolytic therapy for venous thromboembolism. Curr Opin Hematol. Sep 1999;6(5):304-8. [Medline]. 41. Baker WF Jr. Diagnosis of deep venous thrombosis and pulmonary embolism. Med Clin North Am. May 1998;82(3):459-76. [Medline]. 42. Henriksen O, Sejrsen P. Effect of "vein pump" activation upon venous pressure and blood flow in human subcutaneous tissue. Acta Physiol Scand. May 1977;100(1):14-21. [Medline]. 43. Kearon C. Initial treatment of venous thromboembolism. Thromb Haemost. Aug 1999;82(2):887-91. [Medline]. 44. Kakkar VV, Howes J, Sharma V, Kadziola Z. A comparative double-blind, randomised trial of a new second generation LMWH (bemiparin) and UFH in the prevention of post-operative venous thromboembolism. The Bemiparin Assessment group. Thromb Haemost. Apr 2000;83(4):523-9. [Medline]. 45. Heit JA, Mohr DN, Silverstein MD, Petterson TM, O'Fallon WM, Melton LJ 3rd. Predictors of recurrence after deep vein thrombosis and pulmonary embolism: a population-based cohort study. Arch Intern Med. Mar 27 2000;160(6):761-8. [Medline].
18 of 27
05/02/2013 6:21
Deep Venous Thrombosis
http://emedicine.medscape.com/article/1911303-overview
46. Stein PD. Silent pulmonary embolism. Arch Intern Med. Jan 24 2000;160(2):145-6. [Medline]. 47. Lewandowski A, Syska-Suminska J, Dluzniewski M. [Pulmonary embolism suspicion in a young female patient with the Paget-von Schrtter syndrome]. Kardiol Pol. Sep 2008;66(9):969-71. [Medline]. 48. Acharya G, Singh K, Hansen JB, Kumar S, Maltau JM. Catheter-directed thrombolysis for the management of postpartum deep venous thrombosis. Acta Obstet Gynecol Scand. Feb 2005;84(2):155-8. [Medline]. 49. Baarslag HJ, Koopman MM, Hutten BA, Linthorst Homan MW, Bller HR, Reekers JA, et al. Long-term follow-up of patients with suspected deep vein thrombosis of the upper extremity: survival, risk factors and post-thrombotic syndrome. Eur J Intern Med. Dec 2004;15(8):503-507. [Medline]. 50. Joffe HV, Kucher N, Tapson VF, Goldhaber SZ. Upper-extremity deep vein thrombosis: a prospective registry of 592 patients. Circulation. Sep 21 2004;110(12):1605-11. [Medline]. 51. Martinelli I, Battaglioli T, Bucciarelli P, Passamonti SM, Mannucci PM. Risk factors and recurrence rate of primary deep vein thrombosis of the upper extremities. Circulation. Aug 3 2004;110(5):566-70. [Medline]. 52. Beyth RJ, Cohen AM, Landefeld CS. Long-term outcomes of deep-vein thrombosis. Arch Intern Med. May 22 1995;155(10):1031-7. [Medline]. 53. Kistner RL, Ball JJ, Nordyke RA, Freeman GC. Incidence of pulmonary embolism in the course of thrombophlebitis of the lower extremities. Am J Surg. Aug 1972;124(2):169-76. [Medline]. 54. Havig O. Deep vein thrombosis and pulmonary embolism. An autopsy study with multiple regression analysis of possible risk factors. Acta Chir Scand Suppl. 1977;478:1-120. [Medline]. 55. Arfvidsson B, Eklof B, Kistner RL, Masuda EM, Sato DT. Risk factors for venous thromboembolism following prolonged air travel. Coach class thrombosis. Hematol Oncol Clin North Am. Apr 2000;14(2):391-400, ix. [Medline]. 56. Slipman CW, Lipetz JS, Jackson HB, Vresilovic EJ. Deep venous thrombosis and pulmonary embolism as a complication of bed rest for low back pain. Arch Phys Med Rehabil. Jan 2000;81(1):127-9. [Medline]. 57. Ruggeri M, Tosetto A, Castaman G, Rodeghiero F. Congenital absence of the inferior vena cava: a rare risk factor for idiopathic deep-vein thrombosis. Lancet. Feb 10 2001;357(9254):441. [Medline]. 58. Hamoud S, Nitecky S, Engel A, Goldsher D, Hayek T. Hypoplasia of the inferior vena cava with azygous continuation presenting as recurrent leg deep vein thrombosis. Am J Med Sci. Jun 2000;319(6):414-6. [Medline]. 59. Greenfield LJ, Proctor MC. The percutaneous greenfield filter: outcomes and practice patterns. J Vasc Surg. Nov 2000;32(5):888-93. [Medline]. 60. Tsuji Y, Goto A, Hara I, Ataka K, Yamashita C, Okita Y, et al. Renal cell carcinoma with extension of tumor thrombus into the vena cava: surgical strategy and prognosis. J Vasc Surg. Apr 2001;33(4):789-96. [Medline]. 61. Stamatakis JD, Kakkar VV, Sagar S, Lawrence D, Nairn D, Bentley PG. Femoral vein thrombosis and total hip replacement. Br Med J. Jul 23 1977;2(6081):223-5. [Medline]. [Full Text]. 62. Alikhan R, Cohen AT, Combe S, Samama MM, Desjardins L, Eldor A, et al. Risk factors for venous thromboembolism in hospitalized patients with acute medical illness: analysis of the MEDENOX Study. Arch Intern Med. May 10 2004;164(9):963-8. [Medline]. 63. Heit JA, Elliott CG, Trowbridge AA, Morrey BF, Gent M, Hirsh J. Ardeparin sodium for extended out-ofhospital prophylaxis against venous thromboembolism after total hip or knee replacement. A randomized, double-blind, placebo-controlled trial. Ann Intern Med. Jun 6 2000;132(11):853-61. [Medline]. 64. Nordstrm M, Lindblad B, Bergqvist D, Kjellstrm T. A prospective study of the incidence of deep-vein thrombosis within a defined urban population. J Intern Med. Aug 1992;232(2):155-60. [Medline]. 65. Dahlbck B. Inherited thrombophilia: resistance to activated protein C as a pathogenic factor of venous thromboembolism. Blood. Feb 1 1995;85(3):607-14. [Medline]. 66. Anderson FA Jr, Wheeler HB, Goldberg RJ, Hosmer DW, Forcier A. The prevalence of risk factors for venous thromboembolism among hospital patients. Arch Intern Med. Aug 1992;152(8):1660-4. [Medline]. 67. Warlow C, Ogston D, Douglas AS. Deep venous thrombosis of the legs after strokes. Part I--incidence and predisposing factors. Br Med J. May 15 1976;1(6019):1178-81. [Medline]. [Full Text].
19 of 27
05/02/2013 6:21
Deep Venous Thrombosis
http://emedicine.medscape.com/article/1911303-overview
68. Monreal M, Lafoz E, Casals A, Inaraja L, Montserrat E, Callejas JM, et al. Occult cancer in patients with deep venous thrombosis. A systematic approach. Cancer. Jan 15 1991;67(2):541-5. [Medline]. 69. Rickles FR, Levine M, Edwards RL. Hemostatic alterations in cancer patients. Cancer Metastasis Rev. Nov 1992;11(3-4):237-48. [Medline]. 70. Levine MN, Gent M, Hirsh J, Arnold A, Goodyear MD, Hryniuk W, et al. The thrombogenic effect of anticancer drug therapy in women with stage II breast cancer. N Engl J Med. Feb 18 1988;318(7):404-7. [Medline]. 71. Clagett GP, Reisch JS. Prevention of venous thromboembolism in general surgical patients. Results of meta-analysis. Ann Surg. Aug 1988;208(2):227-40. [Medline]. [Full Text]. 72. Clagett GP, Anderson FA Jr, Heit J, Levine MN, Wheeler HB. Prevention of venous thromboembolism. Chest. Oct 1995;108(4 Suppl):312S-334S. [Medline]. 73. Beaty JH. ed. Orthopaedic Knowledge. Ill: AAOS; 1999:63-72. 74. Kakkar VV, Howe CT, Nicolaides AN, Renney JT, Clarke MB. Deep vein thrombosis of the leg. Is there a "high risk" group?. Am J Surg. Oct 1970;120(4):527-30. [Medline]. 75. Dahlbck B. Inherited thrombophilia: resistance to activated protein C as a pathogenic factor of venous thromboembolism. Blood. Feb 1 1995;85(3):607-14. [Medline]. 76. Motykie GD, Caprini JA, Arcelus JI, Zebala LP, Lee CE, Finke NM, et al. Risk factor assessment in the management of patients with suspected deep venous thrombosis. Int Angiol. Mar 2000;19(1):47-51. [Medline]. 77. Motykie GD, Zebala LP, Caprini JA, Lee CE, Arcelus JI, Reyna JJ, et al. A guide to venous thromboembolism risk factor assessment. J Thromb Thrombolysis. Apr 2000;9(3):253-62. [Medline]. 78. Schafer AI. Hypercoagulable states: molecular genetics to clinical practice. Lancet. Dec 24-31 1994;344(8939-8940):1739-42. [Medline]. 79. Meissner MH, Strandness E. Pathophysiology and natural history of acute deep venous thrombosis, Rutherford's Vascular Surgery. 2005:2124-2142. 80. Ho CH, Chau WK, Hsu HC, Gau JP, Yu TJ. Causes of venous thrombosis in fifty Chinese patients. Am J Hematol. Feb 2000;63(2):74-8. [Medline]. 81. Vandenbrouke JP, Bloemenkamp KW, Rosendaal FR, Helmerhorst FM. Incidence of venous thromboembolism in users of combined oral contraceptives. Risk is particularly high with first use of oral contraceptives. BMJ. Jan 1 2000;320(7226):57-8. [Medline]. 82. Tapson VF. Acute pulmonary embolism. N Engl J Med. Mar 6 2008;358(10):1037-52. [Medline]. 83. Cushman M, Tsai AW, White RH, Heckbert SR, Rosamond WD, Enright P, et al. Deep vein thrombosis and pulmonary embolism in two cohorts: the longitudinal investigation of thromboembolism etiology. Am J Med. Jul 1 2004;117(1):19-25. [Medline]. 84. SEVITT S, GALLAGHER N. Venous thrombosis and pulmonary embolism. A clinico-pathological study in injured and burned patients. Br J Surg. Mar 1961;48:475-89. [Medline]. 85. Gorman WP, Davis KR, Donnelly R. ABC of arterial and venous disease. Swollen lower limb-1: general assessment and deep vein thrombosis. BMJ. May 27 2000;320(7247):1453-6. [Medline]. [Full Text]. 86. Kearon C, Crowther M, Hirsh J. Management of patients with hereditary hypercoagulable disorders. Annu Rev Med. 2000;51:169-85. [Medline]. 87. Prandoni P, Mannucci PM. Deep-vein thrombosis of the lower limbs: diagnosis and management. Baillieres Best Pract Res Clin Haematol. Sep 1999;12(3):533-54. [Medline]. 88. Rathbun SW, Raskob GE, Whitsett TL. Sensitivity and specificity of helical computed tomography in the diagnosis of pulmonary embolism: a systematic review. Ann Intern Med. Feb 1 2000;132(3):227-32. [Medline]. 89. Goldhaber SZ. Diagnosis of deep venous thrombosis. Clin Cornerstone. 2000;2(4):29-37. [Medline]. 90. Lensing AW. Anticoagulation in acute ischaemic stroke: deep vein thrombosis prevention and long-term stroke outcomes. Blood Coagul Fibrinolysis. Aug 1999;10 Suppl 2:S123-7. [Medline].
20 of 27
05/02/2013 6:21
Deep Venous Thrombosis
http://emedicine.medscape.com/article/1911303-overview
91. Lensing AW, Prins MH. Recurrent deep vein thrombosis and two coagulation factor gene mutations: quo vadis?. Thromb Haemost. Dec 1999;82(6):1564-6. [Medline]. 92. Deitelzweig S, Jaff MR. Medical management of venous thromboembolic disease. Tech Vasc Interv Radiol. Jun 2004;7(2):63-7. [Medline]. 93. McGarray LJ, Stokes ME, Thompson D. Outcomes of Thromboprophylaxis with enoxaparin vs. Unfractionated Heparin in Medical Inpatients: A Retrospective Database Analysis. Thromb J; 2006:Sep 27;4(1):17. 94. Cosmi B, Palareti G. D-dimer, oral anticoagulation, and venous thromboembolism recurrence. Semin Vasc Med. Nov 2005;5(4):365-70. [Medline]. 95. Perrier A, Desmarais S, Miron MJ, de Moerloose P, Lepage R, Slosman D, et al. Non-invasive diagnosis of venous thromboembolism in outpatients. Lancet. Jan 16 1999;353(9148):190-5. [Medline]. 96. Wells PS, Anderson DR, Rodger M, Forgie M, Kearon C, Dreyer J, et al. Evaluation of D-dimer in the diagnosis of suspected deep-vein thrombosis. N Engl J Med. Sep 25 2003;349(13):1227-35. [Medline]. 97. Bijsterveld NR, Moons AH, Boekholdt SM, van Aken BE, Fennema H, Peters RJ, et al. Ability of recombinant factor VIIa to reverse the anticoagulant effect of the pentasaccharide fondaparinux in healthy volunteers. Circulation. Nov 12 2002;106(20):2550-4. [Medline]. 98. Cohen AT, Dobromirski M. The use of rivaroxaban for short- and long-term treatment of venous thromboembolism. Thromb Haemost. Jun 2012;107(6):1035-43. [Medline]. 99. Romualdi E, Donadini MP, Ageno W. Oral rivaroxaban after symptomatic venous thromboembolism: the continued treatment study (EINSTEIN-extension study). Expert Rev Cardiovasc Ther. Jul 2011;9(7):841-4. [Medline]. 100. [Best Evidence] Prandoni P, Prins MH, Lensing AW, Ghirarduzzi A, Ageno W, Imberti D, et al. Residual thrombosis on ultrasonography to guide the duration of anticoagulation in patients with deep venous thrombosis: a randomized trial. Ann Intern Med. May 5 2009;150(9):577-85. [Medline]. 101. Shulman S, Granqvist S, Holmstrom M, et al. The duration of oral anticoagulation therapy after a second episode of venous thromboembolism. N Engl J Med. 1997;336:393. 102. Lee AY, Levine MN, Baker RI, Bowden C, Kakkar AK, Prins M, et al. Low-molecular-weight heparin versus a coumarin for the prevention of recurrent venous thromboembolism in patients with cancer. N Engl J Med. Jul 10 2003;349(2):146-53. [Medline]. 103. Hull R, Pineo G, Mah A, et al. A randomized trial evaluating long term low molecular weight heparin therapy for three months verses intravenous heparin followed by warfarin sodium. Blood 100. 2002;148a. 104. Pettil V, Kaaja R, Leinonen P, Ekblad U, Kataja M, Ikkala E. Thromboprophylaxis with low molecular weight heparin (dalteparin) in pregnancy. Thromb Res. Nov 15 1999;96(4):275-82. [Medline]. 105. Zidane M, Schram MT, Planken EW, Molendijk WH, Rosendaal FR, van der Meer FJ, et al. Frequency of major hemorrhage in patients treated with unfractionated intravenous heparin for deep venous thrombosis or pulmonary embolism: a study in routine clinical practice. Arch Intern Med. Aug 14-28 2000;160(15):2369-73. [Medline]. 106. Enden T, Haig Y, Klw NE, et al. Long-term outcome after additional catheter-directed thrombolysis versus standard treatment for acute iliofemoral deep vein thrombosis (the CaVenT study): a randomized controlled trial. Lancet. December 2011. 107. Plate G, Akesson H, Einarsson E, Ohlin P, Eklf B. Long-term results of venous thrombectomy combined with a temporary arterio-venous fistula. Eur J Vasc Surg. Oct 1990;4(5):483-9. [Medline]. 108. Eklof B, Kistner RL. Is there a role for thrombectomy in iliofemoral venous thrombosis?. Semin Vasc Surg. Mar 1996;9(1):34-45. [Medline]. 109. Mewissen MW, Seabrook GR, Meissner MH, Cynamon J, Labropoulos N, Haughton SH. Catheter-directed thrombolysis for lower extremity deep venous thrombosis: report of a national multicenter registry. Radiology. Apr 1999;211(1):39-49. [Medline]. 110. Prandoni P, Lensing AW, Prins MH, Frulla M, Marchiori A, Bernardi E, et al. Below-knee elastic compression stockings to prevent the post-thrombotic syndrome: a randomized, controlled trial. Ann Intern Med. Aug 17 2004;141(4):249-56. [Medline].
21 of 27
05/02/2013 6:21
Deep Venous Thrombosis
http://emedicine.medscape.com/article/1911303-overview
111. Partsch H. Ambulation and compression after deep vein thrombosis: dispelling myths. Semin Vasc Surg. Sep 2005;18(3):148-52. [Medline]. 112. Kahn SR, Shrier I, Kearon C. Physical activity in patients with deep venous thrombosis: a systematic review. Thromb Res. 2008;122(6):763-73. [Medline]. 113. Ramos R, Salem BI, De Pawlikowski MP, Coordes C, Eisenberg S, Leidenfrost R. The efficacy of pneumatic compression stockings in the prevention of pulmonary embolism after cardiac surgery. Chest. Jan 1996;109(1):82-5. [Medline]. 114. Skillman JJ, Collins RE, Coe NP, Goldstein BS, Shapiro RM, Zervas NT, et al. Prevention of deep vein thrombosis in neurosurgical patients: a controlled, randomized trial of external pneumatic compression boots. Surgery. Mar 1978;83(3):354-8. [Medline]. 115. Agnelli G, Prandoni P, Santamaria MG, Bagatella P, Iorio A, Bazzan M, et al. Three months versus one year of oral anticoagulant therapy for idiopathic deep venous thrombosis. Warfarin Optimal Duration Italian Trial Investigators. N Engl J Med. Jul 19 2001;345(3):165-9. [Medline]. 116. ALKJAERSIG N, FLETCHER AP, SHERRY S. The mechanism of clot dissolution by plasmin. J Clin Invest. Jul 1959;38(7):1086-95. [Medline]. [Full Text]. 117. American Academy of Family Physicians, American College of Physicians. Current diagnosis of venous thromboembolism in primary care: a clinical practice guideline from the American Academy of Family Physicians and the American College of Physicians. National Guideline Clearinghouse; [Full Text]. 118. Anand SS, Wells PS, Hunt D, Brill-Edwards P, Cook D, Ginsberg JS. Does this patient have deep vein thrombosis?. JAMA. Apr 8 1998;279(14):1094-9. [Medline]. 119. Bauer KA, Eriksson BI, Lassen MR, Turpie AG. Fondaparinux compared with enoxaparin for the prevention of venous thromboembolism after elective major knee surgery. N Engl J Med. Nov 1 2001;345(18):1305-10. [Medline]. 120. Berend KR, Lombardi AV Jr. Multimodal venous thromboembolic disease prevention for patients undergoing primary or revision total joint arthroplasty: the role of aspirin. Am J Orthop (Belle Mead NJ). Jan 2006;35(1):24-9. [Medline]. 121. Bergmann JF, Neuhart E. A multicenter randomized double-blind study of enoxaparin compared with unfractionated heparin in the prevention of venous thromboembolic disease in elderly in-patients bedridden for an acute medical illness. The Enoxaparin in Medicine Study Group. Thromb Haemost. Oct 1996;76(4):529-34. [Medline]. 122. Bjarnason H, Kruse JR, Asinger DA, Nazarian GK, Dietz CA Jr, Caldwell MD, et al. Iliofemoral deep venous thrombosis: safety and efficacy outcome during 5 years of catheter-directed thrombolytic therapy. J Vasc Interv Radiol. May-Jun 1997;8(3):405-18. [Medline]. 123. Boudes PF. The challenges of new drugs benefits and risks analysis: lessons from the ximelagatran FDA Cardiovascular Advisory Committee. Contemp Clin Trials. Oct 2006;27(5):432-40. [Medline]. 124. Breddin HK. Low molecular weight heparins in the prevention of deep-vein thrombosis in general surgery. Semin Thromb Hemost. 1999;25 Suppl 3:83-9. [Medline]. 125. Bulger CM, Jacobs C, Patel NH. Epidemiology of acute deep vein thrombosis. Tech Vasc Interv Radiol. Jun 2004;7(2):50-4. [Medline]. 126. Burke DT. Prevention of deep venous thrombosis: overview of available therapy options for rehabilitation patients. Am J Phys Med Rehabil. Sep-Oct 2000;79(5 Suppl):S3-8. [Medline]. 127. Bller HR, Agnelli G, Hull RD, Hyers TM, Prins MH, Raskob GE. Antithrombotic therapy for venous thromboembolic disease: the Seventh ACCP Conference on Antithrombotic and Thrombolytic Therapy. Chest. Sep 2004;126(3 Suppl):401S-428S. [Medline]. 128. [Best Evidence] Camporese G, Bernardi E, Prandoni P, Noventa F, Verlato F, Simioni P, et al. Low-molecularweight heparin versus compression stockings for thromboprophylaxis after knee arthroscopy: a randomized trial. Ann Intern Med. Jul 15 2008;149(2):73-82. [Medline]. 129. Caprini JA, Arcelus JI, Maksimovic D, Glase CJ, Sarayba JG, Hathaway K. Thrombosis prophylaxis in orthopedic surgery: current clinical considerations. J South Orthop Assoc. Winter 2002;11(4):190-6. [Medline]. 130. Cham MD, Yankelevitz DF, Shaham D, Shah AA, Sherman L, Lewis A, et al. Deep venous thrombosis:
22 of 27
05/02/2013 6:21
Deep Venous Thrombosis
http://emedicine.medscape.com/article/1911303-overview
detection by using indirect CT venography. The Pulmonary Angiography-Indirect CT Venography Cooperative Group. Radiology. Sep 2000;216(3):744-51. [Medline]. 131. Cho JS, Martelli E, Mozes G, Miller VM, Gloviczki P. Effects of thrombolysis and venous thrombectomy on valvular competence, thrombogenicity, venous wall morphology, and function. J Vasc Surg. Nov 1998;28(5):787-99. [Medline]. 132. Coche EE, Hamoir XL, Hammer FD, Hainaut P, Goffette PP. Using dual-detector helical CT angiography to detect deep venous thrombosis in patients with suspicion of pulmonary embolism: diagnostic value and additional findings. AJR Am J Roentgenol. Apr 2001;176(4):1035-9. [Medline]. 133. Colwell C, Mouret P. Ximelagatran for the prevention of venous thromboembolism following elective hip or knee replacement surgery. Semin Vasc Med. Aug 2005;5(3):266-75. [Medline]. 134. Comerota AJ, Throm RC, Mathias SD, Haughton S, Mewissen M. Catheter-directed thrombolysis for iliofemoral deep venous thrombosis improves health-related quality of life. J Vasc Surg. Jul 2000;32(1):130-7. [Medline]. 135. Comp PC, Spiro TE, Friedman RJ, Whitsett TL, Johnson GJ, Gardiner GA Jr, et al. Prolonged enoxaparin therapy to prevent venous thromboembolism after primary hip or knee replacement. Enoxaparin Clinical Trial Group. J Bone Joint Surg Am. Mar 2001;83-A(3):336-45. [Medline]. 136. Deitelzweig S, Jaff MR. Medical management of venous thromboembolic disease. Tech Vasc Interv Radiol. Jun 2004;7(2):63-7. [Medline]. 137. DOULBLE REF141. 138. Dranitsaris G, Stumpo C, Smith R, Bartle W. Extended dalteparin prophylaxis for venous thromboembolic events: cost-utility analysis in patients undergoing major orthopedic surgery. Am J Cardiovasc Drugs. 2009;9(1):45-58. [Medline]. 139. Eklof B, Arfvidsson B, Kistner RL, Masuda EM. Indications for surgical treatment of iliofemoral vein thrombosis. Hematol Oncol Clin North Am. Apr 2000;14(2):471-82. [Medline]. 140. Epstein NE. Efficacy of pneumatic compression stocking prophylaxis in the prevention of deep venous thrombosis and pulmonary embolism following 139 lumbar laminectomies with instrumented fusions. J Spinal Disord Tech. Feb 2006;19(1):28-31. [Medline]. 141. Eriksson BI, Borris LC, Friedman RJ, Haas S, Huisman MV, Kakkar AK, et al. Rivaroxaban versus enoxaparin for thromboprophylaxis after hip arthroplasty. N Engl J Med. Jun 26 2008;358(26):2765-75. [Medline]. 142. Eskeland G, Solheim K, Skjrten F. Anticoagulant prophylaxis, thromboembolism and mortality in elderly patients with hip fractures. A controlled clinical trial. Acta Chir Scand. Jan-Feb 1966;131(1):16-29. [Medline]. 143. Fisher CG, Blachut PA, Salvian AJ, Meek RN, O'Brien PJ. Effectiveness of pneumatic leg compression devices for the prevention of thromboembolic disease in orthopaedic trauma patients: a prospective, randomized study of compression alone versus no prophylaxis. J Orthop Trauma. Feb 1995;9(1):1-7. [Medline]. 144. Francis CW, Berkowitz SD, Comp PC, Lieberman JR, Ginsberg JS, Paiement G, et al. Comparison of ximelagatran with warfarin for the prevention of venous thromboembolism after total knee replacement. N Engl J Med. Oct 30 2003;349(18):1703-12. [Medline]. 145. Gaffney PJ, Creighton LJ, Callus M, Thorpe R. Monoclonal antibodies to crosslinked fibrin degradation products (XL-FDP). II. Evaluation in a variety of clinical conditions. Br J Haematol. Jan 1988;68(1):91-6. [Medline]. 146. Geerts WH, Heit JA, Clagett GP, Pineo GF, Colwell CW, Anderson FA Jr, et al. Prevention of venous thromboembolism. Chest. Jan 2001;119(1 Suppl):132S-175S. [Medline]. 147. Gerotziafas GT, Samama MM. Heterogeneity of synthetic factor Xa inhibitors. Curr Pharm Des. 2005;11(30):3855-76. [Medline]. 148. Gillies TE, Ruckley CV, Nixon SJ. Still missing the boat with fatal pulmonary embolism. Br J Surg. Oct 1996;83(10):1394-5. [Medline]. 149. Ginsberg JS, Turkstra F, Buller HR, MacKinnon B, Magier D, Hirsh J. Postthrombotic syndrome after hip or knee arthroplasty: a cross-sectional study. Arch Intern Med. Mar 13 2000;160(5):669-72. [Medline]. 150. Grossman C, McPherson S. Safety and efficacy of catheter-directed thrombolysis for iliofemoral venous
23 of 27
05/02/2013 6:21
Deep Venous Thrombosis
http://emedicine.medscape.com/article/1911303-overview
thrombosis. AJR Am J Roentgenol. Mar 1999;172(3):667-72. [Medline]. 151. Heit JA, Silverstein MD, Mohr DN, Petterson TM, O'Fallon WM, Melton LJ 3rd. Risk factors for deep vein thrombosis and pulmonary embolism: a population-based case-control study. Arch Intern Med. Mar 27 2000;160(6):809-15. [Medline]. 152. [Guideline] Hirsh J, Guyatt G, Albers GW, Harrington R, Schnemann HJ, American College of Chest Physician. Antithrombotic and thrombolytic therapy: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines (8th Edition). Chest. Jun 2008;133(6 Suppl):110S-112S. [Medline]. 153. Horellou MH, Conrad J, Samama MM. An Evidence-Based Atlas. In: Venous Thromboembolism:. Armonk, NY: Futura; 1996. 154. Hull RD, Pineo GF. Prophylaxis of deep venous thrombosis and pulmonary embolism. Current recommendations. Med Clin North Am. May 1998;82(3):477-93. [Medline]. 155. Hull RD, Pineo GF, Francis C, Bergqvist D, Fellenius C, Soderberg K, et al. Low-molecular-weight heparin prophylaxis using dalteparin extended out-of-hospital vs in-hospital warfarin/out-of-hospital placebo in hip arthroplasty patients: a double-blind, randomized comparison. North American Fragmin Trial Investigators. Arch Intern Med. Jul 24 2000;160(14):2208-15. [Medline]. 156. Hull RD, Pineo GF, Stein PD, Mah AF, MacIsaac SM, Dahl OE, et al. Timing of initial administration of low-molecular-weight heparin prophylaxis against deep vein thrombosis in patients following elective hip arthroplasty: a systematic review. Arch Intern Med. Sep 10 2001;161(16):1952-60. [Medline]. 157. Hull RD, Raskob GE, Brant RF, Pineo GF, Valentine KA. Relation between the time to achieve the lower limit of the APTT therapeutic range and recurrent venous thromboembolism during heparin treatment for deep vein thrombosis. Arch Intern Med. Dec 8-22 1997;157(22):2562-8. [Medline]. 158. Hull RD, Raskob GE, Brant RF, Pineo GF, Valentine KA. The importance of initial heparin treatment on long-term clinical outcomes of antithrombotic therapy. The emerging theme of delayed recurrence. Arch Intern Med. Nov 10 1997;157(20):2317-21. [Medline]. 159. Iskander GA, Nelson RS, Morehouse DL, Tenquist JE, Szlabick RE. Incidence and propagation of infrageniculate deep venous thrombosis in trauma patients. J Trauma. Sep 2006;61(3):695-700. [Medline]. 160. Kakkar AK, Brenner B, Dahl OE, Eriksson BI, Mouret P, Muntz J, et al. Extended duration rivaroxaban versus short-term enoxaparin for the prevention of venous thromboembolism after total hip arthroplasty: a doubleblind, randomised controlled trial. Lancet. Jul 5 2008;372(9632):31-9. [Medline]. 161. Kakkar VV, Adams PC. Preventive and therapeutic approach to venous thromboembolic disease and pulmonary embolism--can death from pulmonary embolism be prevented?. J Am Coll Cardiol. Dec 1986;8(6 Suppl B):146B-158B. [Medline]. 162. Katz DS, Hon M. Current DVT imaging. Tech Vasc Interv Radiol. Jun 2004;7(2):55-62. [Medline]. 163. Kearon C. Epidemiology of venous thromboembolism. Semin Vasc Med. 2001;1(1):7-26. [Medline]. 164. [Best Evidence] Kearon C, Ginsberg JS, Julian JA, Douketis J, Solymoss S, Ockelford P, et al. Comparison of fixed-dose weight-adjusted unfractionated heparin and low-molecular-weight heparin for acute treatment of venous thromboembolism. JAMA. Aug 23 2006;296(8):935-42. [Medline]. 165. Kearon C, Ginsberg JS, Kovacs MJ, Anderson DR, Wells P, Julian JA, et al. Comparison of low-intensity warfarin therapy with conventional-intensity warfarin therapy for long-term prevention of recurrent venous thromboembolism. N Engl J Med. Aug 14 2003;349(7):631-9. [Medline]. 166. Kearon C, Julian JA, Newman TE, Ginsberg JS. Noninvasive diagnosis of deep venous thrombosis. McMaster Diagnostic Imaging Practice Guidelines Initiative. Ann Intern Med. Apr 15 1998;128(8):663-77. [Medline]. 167. Kearon C, Kahn SR, Agnelli G, Goldhaber S, Raskob GE, Comerota AJ. Antithrombotic therapy for venous thromboembolic disease: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines (8th Edition). Chest. Jun 2008;133(6 Suppl):454S-545S. [Medline]. 168. Keeney JA, Clohisy JC, Curry MC, Maloney WJ. Efficacy of combined modality prophylaxis including shortduration warfarin to prevent venous thromboembolism after total hip arthroplasty. J Arthroplasty. Jun 2006;21(4):469-75. [Medline]. 169. Knight LC, Baidoo KE, Romano JE, Gabriel JL, Maurer AH. Imaging pulmonary emboli and deep venous thrombi with 99mTc-bitistatin, a platelet-binding polypeptide from viper venom. J Nucl Med. Jun
24 of 27
05/02/2013 6:21
Deep Venous Thrombosis
http://emedicine.medscape.com/article/1911303-overview
2000;41(6):1056-64. [Medline]. 170. Korelitz BI, Sommers SC. Responses to drug therapy in ulcerative colitis. Evaluation by rectal biopsy and histopathological changes. Am J Gastroenterol. Nov 1975;64(5):365-70. [Medline]. 171. Lachiewicz PF, Kelley SS, Haden LR. Two mechanical devices for prophylaxis of thromboembolism after total knee arthroplasty. A prospective, randomised study. J Bone Joint Surg Br. Nov 2004;86(8):1137-41. [Medline]. 172. Lassen MR, Ageno W, Borris LC, Lieberman JR, Rosencher N, Bandel TJ, et al. Rivaroxaban versus enoxaparin for thromboprophylaxis after total knee arthroplasty. N Engl J Med. Jun 26 2008;358(26):2776-86. [Medline]. 173. Lassen MR, Bauer KA, Eriksson BI, Turpie AG. Postoperative fondaparinux versus preoperative enoxaparin for prevention of venous thromboembolism in elective hip-replacement surgery: a randomised double-blind comparison. Lancet. May 18 2002;359(9319):1715-20. [Medline]. 174. Leizorovicz A, Haugh MC, Chapuis FR, Samama MM, Boissel JP. Low molecular weight heparin in prevention of perioperative thrombosis. BMJ. Oct 17 1992;305(6859):913-20. [Medline]. [Full Text]. 175. [Best Evidence] Leonardi MJ, McGory ML, Ko CY. The rate of bleeding complications after pharmacologic deep venous thrombosis prophylaxis: a systematic review of 33 randomized controlled trials. Arch Surg. Aug 2006;141(8):790-7; discussion 797-9. [Medline]. 176. Levine MN, Hirsh J, Gent M, Turpie AG, Leclerc J, Powers PJ, et al. Prevention of deep vein thrombosis after elective hip surgery. A randomized trial comparing low molecular weight heparin with standard unfractionated heparin. Ann Intern Med. Apr 1 1991;114(7):545-51. [Medline]. 177. Linkins LA, Choi PT, Douketis JD. Clinical impact of bleeding in patients taking oral anticoagulant therapy for venous thromboembolism: a meta-analysis. Ann Intern Med. Dec 2 2003;139(11):893-900. [Medline]. 178. Lotke PA, Lonner JH. The benefit of aspirin chemoprophylaxis for thromboembolism after total knee arthroplasty. Clin Orthop Relat Res. Nov 2006;452:175-80. [Medline]. 179. Loud PA, Katz DS, Bruce DA, Klippenstein DL, Grossman ZD. Deep venous thrombosis with suspected pulmonary embolism: detection with combined CT venography and pulmonary angiography. Radiology. May 2001;219(2):498-502. [Medline]. 180. Loud PA, Katz DS, Klippenstein DL, Shah RD, Grossman ZD. Combined CT venography and pulmonary angiography in suspected thromboembolic disease: diagnostic accuracy for deep venous evaluation. AJR Am J Roentgenol. Jan 2000;174(1):61-5. [Medline]. 181. Meissner MH, Manzo RA, Bergelin RO, Markel A, Strandness DE Jr. Deep venous insufficiency: the relationship between lysis and subsequent reflux. J Vasc Surg. Oct 1993;18(4):596-605; discussion 606-8. [Medline]. 182. Merli GJ. Prophylaxis for deep venous thrombosis and pulmonary embolism in the surgical patient. Clin Cornerstone. 2000;2(4):15-28. [Medline]. 183. Mewissen MW, Seabrook GR, Meissner MH, Cynamon J, Labropoulos N, Haughton SH. Catheter-directed thrombolysis for lower extremity deep venous thrombosis: report of a national multicenter registry. Radiology. Apr 1999;211(1):39-49. [Medline]. 184. Michiels JJ, Oortwijn WJ, Naaborg R. Exclusion and diagnosis of deep vein thrombosis by a rapid ELISA D-dimer test, compression ultrasonography, and a simple clinical model. Clin Appl Thromb Hemost. Jul 1999;5(3):171-80. [Medline]. 185. Michota F, Merli G. Anticoagulation in special patient populations: are special dosing considerations required?. Cleve Clin J Med. Apr 2005;72 Suppl 1:S37-42. [Medline]. 186. [Best Evidence] Mismetti P, Quenet S, Levine M, Merli G, Decousus H, Derobert E, et al. Enoxaparin in the treatment of deep vein thrombosis with or without pulmonary embolism: an individual patient data meta-analysis. Chest. Oct 2005;128(4):2203-10. [Medline]. 187. Muntz JE, Friedman RJ, eds. Case Vignettes: Thromboprophylaxis in Arthroscopic Surgery. Elsevier Excerpta Medica. 2006. 188. Nawaz S, Chan P, Ireland S. Suspected deep vein thrombosis: a management algorithm for the accident and emergency department. J Accid Emerg Med. Nov 1999;16(6):440-2. [Medline]. [Full Text].
25 of 27
05/02/2013 6:21
Deep Venous Thrombosis
http://emedicine.medscape.com/article/1911303-overview
189. O'Brien SH, Haley K, Kelleher KJ, Wang W, McKenna C, Gaines BA. Variation in DVT prophylaxis for adolescent trauma patients: a survey of the Society of Trauma Nurses. J Trauma Nurs. Apr-Jun 2008;15(2):53-7. [Medline]. 190. Prevention of fatal postoperative pulmonary embolism by low doses of heparin. An international multicentre trial. Lancet. Jul 12 1975;2(7924):45-51. [Medline]. 191. Prevention of pulmonary embolism and deep vein thrombosis with low dose aspirin: Pulmonary Embolism Prevention (PEP) trial. Lancet. Apr 15 2000;355(9212):1295-302. [Medline]. 192. Prevention of thromboembolism in spinal cord injury. Consortium for Spinal Cord Medicine. J Spinal Cord Med. Jul 1997;20(3):259-83. [Medline]. 193. Quinlan DJ, McQuillan A, Eikelboom JW. Low-molecular-weight heparin compared with intravenous unfractionated heparin for treatment of pulmonary embolism: a meta-analysis of randomized, controlled trials. Ann Intern Med. Feb 3 2004;140(3):175-83. [Medline]. 194. Ramzi DW, Leeper KV. DVT and pulmonary embolism: Part II. Treatment and prevention. Am Fam Physician. Jun 15 2004;69(12):2841-8. [Medline]. 195. Rhodes JM, Cho JS, Gloviczki P, Mozes G, Rolle R, Miller VM. Thrombolysis for experimental deep venous thrombosis maintains valvular competence and vasoreactivity. J Vasc Surg. Jun 2000;31(6):1193-205. [Medline]. 196. Ridker PM, Goldhaber SZ, Danielson E, Rosenberg Y, Eby CS, Deitcher SR, et al. Long-term, low-intensity warfarin therapy for the prevention of recurrent venous thromboembolism. N Engl J Med. Apr 10 2003;348(15):1425-34. [Medline]. 197. Rosendaal FR. Venous thrombosis: a multicausal disease. Lancet. Apr 3 1999;353(9159):1167-73. [Medline]. 198. Salvati EA, Pellegrini VD Jr, Sharrock NE, Lotke PA, Murray DW, Potter H, et al. Recent advances in venous thromboembolic prophylaxis during and after total hip replacement. J Bone Joint Surg Am. Feb 2000;82(2):252-70. [Medline]. 199. Schiff RL, Kahn SR, Shrier I, Strulovitch C, Hammouda W, Cohen E, et al. Identifying orthopedic patients at high risk for venous thromboembolism despite thromboprophylaxis. Chest. Nov 2005;128(5):3364-71. [Medline]. 200. Schweizer J, Kirch W, Koch R, Elix H, Hellner G, Forkmann L, et al. Short- and long-term results after thrombolytic treatment of deep venous thrombosis. J Am Coll Cardiol. Oct 2000;36(4):1336-43. [Medline]. 201. Shepard RM Jr, White HA, Shirkey AL. Anticoagulant prophylaxis of thromboembolism in postsurgical patients. Am J Surg. Nov 1966;112(5):698-702. [Medline]. 202. Snyder BK. Venous thromboembolic prophylaxis: the use of aspirin. Orthop Nurs. Jul-Aug 2008;27(4):225-30; quiz 231-2. [Medline]. 203. Sors H, Meyer G. Place of aspirin in prophylaxis of venous thromboembolism. Lancet. Apr 15 2000;355(9212):1288-9. [Medline]. 204. Taillefer R, Edell S, Innes G, Lister-James J. Acute thromboscintigraphy with (99m)Tc-apcitide: results of the phase 3 multicenter clinical trial comparing 99mTc-apcitide scintigraphy with contrast venography for imaging acute DVT. Multicenter Trial Investigators. J Nucl Med. Jul 2000;41(7):1214-23. [Medline]. 205. Turpie AG, Bauer KA, Eriksson BI, Lassen MR. Fondaparinux vs enoxaparin for the prevention of venous thromboembolism in major orthopedic surgery: a meta-analysis of 4 randomized double-blind studies. Arch Intern Med. Sep 9 2002;162(16):1833-40. [Medline]. 206. Turpie AG, Gallus AS, Hoek JA. A synthetic pentasaccharide for the prevention of deep-vein thrombosis after total hip replacement. N Engl J Med. Mar 1 2001;344(9):619-25. [Medline]. 207. Turpie AG, Lassen MR, Davidson BL, Bauer KA, Gent M, Kwong LM, et al. Rivaroxaban versus enoxaparin for thromboprophylaxis after total knee arthroplasty (RECORD4): a randomised trial. Lancet. May 16 2009;373(9676):1673-80. [Medline]. 208. U.S. Food and Drug Administration. Communication about an Ongoing Safety ReviewInnohep (tinzaparin sodium injection). U.S. Food and Drug Administration. Available at http://www.fda.gov/cder/drug/early_comm /tinzaparin.htm. Accessed March 12, 2009.
26 of 27
05/02/2013 6:21
Deep Venous Thrombosis
http://emedicine.medscape.com/article/1911303-overview
209. [Best Evidence] van Dongen CJ, MacGillavry MR, Prins MH. Once versus twice daily LMWH for the initial treatment of venous thromboembolism. Cochrane Database Syst Rev. Jul 20 2005;CD003074. [Medline]. 210. Vedantham S, Millward SF, Cardella JF, Hofmann LV, Razavi MK, Grassi CJ, et al. Society of Interventional Radiology position statement: treatment of acute iliofemoral deep vein thrombosis with use of adjunctive catheter-directed intrathrombus thrombolysis. J Vasc Interv Radiol. Apr 2006;17(4):613-6. [Medline]. 211. Verstraete M. Direct thrombin inhibitors: appraisal of the antithrombotic/hemorrhagic balance. Thromb Haemost. Jul 1997;78(1):357-63. [Medline]. 212. Weitz JI, Middeldorp S, Geerts W, Heit JA. Thrombophilia and new anticoagulant drugs. Hematology Am Soc Hematol Educ Program. 2004;424-38. [Medline]. 213. [Best Evidence] Wells PS, Anderson DR, Rodger MA, Forgie MA, Florack P, Touchie D, et al. A randomized trial comparing 2 low-molecular-weight heparins for the outpatient treatment of deep vein thrombosis and pulmonary embolism. Arch Intern Med. Apr 11 2005;165(7):733-8. [Medline]. Medscape Reference 2011 WebMD, LLC
27 of 27
05/02/2013 6:21
You might also like
- Urinary Tract Infections (Utis) : Guidelines For The Prevention and Treatment of in Continuing Care SettingsDocument28 pagesUrinary Tract Infections (Utis) : Guidelines For The Prevention and Treatment of in Continuing Care SettingsRezkyRamadhaniSyarifNo ratings yet
- Choice of Renal Replacement TherapyDocument11 pagesChoice of Renal Replacement TherapyphoechoexNo ratings yet
- Hyponatremia Algorhythm Concept MapDocument2 pagesHyponatremia Algorhythm Concept Mapnursing concept mapsNo ratings yet
- Best Practice & Research Clinical Endocrinology & MetabolismDocument9 pagesBest Practice & Research Clinical Endocrinology & MetabolismaldiansyahraufNo ratings yet
- Ngeyel 2Document1 pageNgeyel 2phoechoexNo ratings yet
- ABSTRAKDocument2 pagesABSTRAKphoechoexNo ratings yet
- Evaluasi Penerapan Perlakuan Akuntansi Psak 24 Pada PT Gudang Garam TBKDocument9 pagesEvaluasi Penerapan Perlakuan Akuntansi Psak 24 Pada PT Gudang Garam TBKphoechoexNo ratings yet
- Diagnosis of HypokalemiaDocument8 pagesDiagnosis of HypokalemiaphoechoexNo ratings yet
- 2010 Article 9216 PDFDocument8 pages2010 Article 9216 PDFphoechoexNo ratings yet
- Management of Febrile NeutropeniaDocument5 pagesManagement of Febrile NeutropeniaphoechoexNo ratings yet
- DVT Work UpDocument18 pagesDVT Work UpphoechoexNo ratings yet
- DVT KlinisDocument18 pagesDVT KlinisphoechoexNo ratings yet
- DVT TreatmentDocument24 pagesDVT TreatmentphoechoexNo ratings yet
- DVT KlinisDocument18 pagesDVT KlinisphoechoexNo ratings yet
- The Hygiene Hypothesis' For Autoimmune and Allergic Diseases - An Update PDFDocument9 pagesThe Hygiene Hypothesis' For Autoimmune and Allergic Diseases - An Update PDFphoechoexNo ratings yet
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5782)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (72)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Self-Management Education Program For Reduce Blood Glucose Type 2 Diabetes Mellitus: A Systematic ReviewDocument9 pagesSelf-Management Education Program For Reduce Blood Glucose Type 2 Diabetes Mellitus: A Systematic ReviewFerry EfendiNo ratings yet
- Marker 2017Document9 pagesMarker 2017Christine SiburianNo ratings yet
- Nutrition and AIDSDocument250 pagesNutrition and AIDSLies Pramana SariNo ratings yet
- Colitis, Ulcerative: Whitney D. Lynch Ronald HsuDocument8 pagesColitis, Ulcerative: Whitney D. Lynch Ronald HsuAlexis DF SanchezNo ratings yet
- Improving Knowledge on Hypertension PreventionDocument9 pagesImproving Knowledge on Hypertension PreventionIntan OktavianiNo ratings yet
- Endo Don TicDocument8 pagesEndo Don TicArmareality Armareality100% (1)
- Sleep Apnea PresentationDocument73 pagesSleep Apnea PresentationChad WhiteheadNo ratings yet
- Natural History of Disease and Infectious Disease Cycle 2Document40 pagesNatural History of Disease and Infectious Disease Cycle 2elsawzgoodNo ratings yet
- 02 IVD-R Deep-Dive Deck NewDocument215 pages02 IVD-R Deep-Dive Deck NewrajiveacharyaNo ratings yet
- Appendix1 MorphineDocument75 pagesAppendix1 Morphine민규강No ratings yet
- Wa0017.Document9 pagesWa0017.CHAMBI MAMANI JESSICA BETTYNo ratings yet
- Space Maintenance: Emma Laing, Paul Ashley, Farhad B. Naini & Daljit S. GillDocument8 pagesSpace Maintenance: Emma Laing, Paul Ashley, Farhad B. Naini & Daljit S. GillAnonymous JR1VNCNo ratings yet
- Maternal NursingDocument16 pagesMaternal NursingJayCesarNo ratings yet
- CT 11 - HPNDocument12 pagesCT 11 - HPNLycah RotoneNo ratings yet
- Inspection Workbook Obstetrics and GynecologyDocument40 pagesInspection Workbook Obstetrics and Gynecologydelap05No ratings yet
- Company Profile 2018Document18 pagesCompany Profile 2018Sarana Renal IndonesiaNo ratings yet
- Subacute Bacterial Endocarditis: Sadewantoro, DR, SP - JPDocument25 pagesSubacute Bacterial Endocarditis: Sadewantoro, DR, SP - JPfelicedaNo ratings yet
- Clinical Features and Diagnosis of Hemophagocytic Lymphohistiocytosis - UpToDateDocument27 pagesClinical Features and Diagnosis of Hemophagocytic Lymphohistiocytosis - UpToDateSalvatore ScutoNo ratings yet
- Hepol4 PDFDocument77 pagesHepol4 PDFajayNo ratings yet
- Ceftriaxone Drug StudyDocument1 pageCeftriaxone Drug Studymilkv71% (7)
- Should We Donate Our Organs or NotDocument6 pagesShould We Donate Our Organs or NotIvanKurniawanSiagianNo ratings yet
- NCP - Pulmonary TuberculosisDocument6 pagesNCP - Pulmonary TuberculosisastrijuNo ratings yet
- Rapid Communication: Spontaneous Abortions and Policies On COVID-19 mRNA Vaccine Use During PregnancyDocument14 pagesRapid Communication: Spontaneous Abortions and Policies On COVID-19 mRNA Vaccine Use During PregnancyStéphane BoucherNo ratings yet
- Professional Portfolio NFDN 2003Document2 pagesProfessional Portfolio NFDN 2003api-319266253No ratings yet
- Management and Outcomes of Placenta Accreta Spectrum (PAS) at Tertiary Hospital in Bali: Descriptive Case Series StudyDocument15 pagesManagement and Outcomes of Placenta Accreta Spectrum (PAS) at Tertiary Hospital in Bali: Descriptive Case Series Studyimamsantos1191No ratings yet
- Bleeding Peripheral Points. An Acupuncture TechniqueDocument6 pagesBleeding Peripheral Points. An Acupuncture TechniqueSanjay PatilNo ratings yet
- Delirium PresentationDocument52 pagesDelirium PresentationmyscribeNo ratings yet
- Vake's Proposal On HepatitisDocument26 pagesVake's Proposal On HepatitisVake MtongaNo ratings yet
- Multiple SclerosisDocument8 pagesMultiple SclerosisNader Smadi100% (1)
- Estate of Dennis Choquette v. Corrections Corporation of America, Et. Al.Document70 pagesEstate of Dennis Choquette v. Corrections Corporation of America, Et. Al.Michael_Lee_RobertsNo ratings yet