You might also like
- Me Desires-Erotic PoetryDocument21 pagesMe Desires-Erotic PoetrygamahucherNo ratings yet
- Chapter 30 Assessment and Management of Patients With Vascular Disorders and Problems of Peripheral CirculationDocument23 pagesChapter 30 Assessment and Management of Patients With Vascular Disorders and Problems of Peripheral CirculationAbel C. Idusma Jr.No ratings yet
- HaemophiliaDocument36 pagesHaemophiliasakharam_gawadeNo ratings yet
- HEMOPHILIADocument74 pagesHEMOPHILIASylvia LoongNo ratings yet
- The New Jewish Wedding by Anita DiamantDocument39 pagesThe New Jewish Wedding by Anita DiamantSimon and Schuster27% (15)
- Benjamin Joel - American Grandmaster. Four Decades of Chess Adventures, 2007-OCR, Everyman, 270p PDFDocument270 pagesBenjamin Joel - American Grandmaster. Four Decades of Chess Adventures, 2007-OCR, Everyman, 270p PDFGabriel Henrique100% (1)
- OLFUPAC Nursing Case Study on Traumatic AmputationDocument13 pagesOLFUPAC Nursing Case Study on Traumatic AmputationKristine Dela Pasion100% (2)
- Flat Foot SurgeryDocument5 pagesFlat Foot SurgeryManoj KandoiNo ratings yet
- Phlebitis, (Inflamed Veins) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandPhlebitis, (Inflamed Veins) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- HemophiliaDocument62 pagesHemophiliamuhirwa Samuel100% (1)
- Bleeding Disorders: HemophiliaDocument21 pagesBleeding Disorders: Hemophiliaعبيدة محمد ابو عابدNo ratings yet
- Knee PainDocument34 pagesKnee Painmanoj ramlal kandoi100% (1)
- Knee PainDocument34 pagesKnee Painmanoj ramlal kandoi100% (1)
- (Traves D. Crabtree) BRS Surgical Specialties PDFDocument254 pages(Traves D. Crabtree) BRS Surgical Specialties PDFCosmin Alexa100% (2)
- Characteristics of An Effective CounselorDocument5 pagesCharacteristics of An Effective CounselorAbbas KhanNo ratings yet
- Gouty ArthritisDocument12 pagesGouty ArthritisManoj KandoiNo ratings yet
- Gouty ArthritisDocument12 pagesGouty ArthritisManoj KandoiNo ratings yet
- Retaining Wall With PilesDocument7 pagesRetaining Wall With PilesEngineering KaizenNo ratings yet
- Lecture Notes: General Surgery, with Wiley E-TextFrom EverandLecture Notes: General Surgery, with Wiley E-TextRating: 3.5 out of 5 stars3.5/5 (4)
- CASE STUDY 80: Rheumatoid ArthritisDocument7 pagesCASE STUDY 80: Rheumatoid Arthritisangelica dizon100% (1)
- Voh Sham Kuch Ajeeb Thi - A Brother Sister Saga (HindiDocument403 pagesVoh Sham Kuch Ajeeb Thi - A Brother Sister Saga (HindiDesi Rocks100% (1)
- Polycythemia Vera CompletedDocument5 pagesPolycythemia Vera CompletedSaro BalberanNo ratings yet
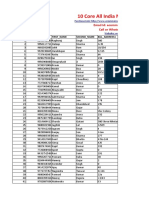
- 5 All India Mobile Database SampleDocument15 pages5 All India Mobile Database Sampleali khan Saifi100% (1)
- Rheumatoid ArthritisDocument18 pagesRheumatoid Arthritismanoj ramlal kandoiNo ratings yet
- Hemophilic Pseudotumors: Natural History and A Case Report of Pseudotumor With Femur Fracture and Swan-Neck DeformityDocument5 pagesHemophilic Pseudotumors: Natural History and A Case Report of Pseudotumor With Femur Fracture and Swan-Neck Deformityyudhi kurniawanNo ratings yet
- Management of Haemorrhage in Oral SurgeryDocument3 pagesManagement of Haemorrhage in Oral SurgeryadikaNo ratings yet
- A Study To Evaluate Effectiveness of Cold Application and Magnesium Sulphate Application On Superficial Thrombophlebitis Among Patients Receiving Intravenous Therapy in Selected Hospitals Amritsar.Document25 pagesA Study To Evaluate Effectiveness of Cold Application and Magnesium Sulphate Application On Superficial Thrombophlebitis Among Patients Receiving Intravenous Therapy in Selected Hospitals Amritsar.Navjot Brar71% (14)
- Arterial UlcersDocument8 pagesArterial Ulcerspka25No ratings yet
- Hemophilic ArthropathyDocument10 pagesHemophilic ArthropathyErnesto GariNo ratings yet
- Hemostasis 19-3-2012Document11 pagesHemostasis 19-3-2012Mateen ShukriNo ratings yet
- Hemorrhage and Shock PresentationDocument33 pagesHemorrhage and Shock PresentationJoy JoycNo ratings yet
- Immune Thrombocytopenic Purpura (ITP) :: A New Look at An Old DisorderDocument6 pagesImmune Thrombocytopenic Purpura (ITP) :: A New Look at An Old DisorderAsri Alifa SholehahNo ratings yet
- Case Study 2Document7 pagesCase Study 2desdav100% (1)
- 15: Peripheral Vascular Disease: Patient Evaluation The Vascular DiseasesDocument15 pages15: Peripheral Vascular Disease: Patient Evaluation The Vascular DiseasespoddataNo ratings yet
- Hemangioma Oral (Gill)Document4 pagesHemangioma Oral (Gill)koizorabigNo ratings yet
- Managing limb oedema with magnesium sulphate and glycerineDocument18 pagesManaging limb oedema with magnesium sulphate and glycerineRichard PremNo ratings yet
- NO Particular Pages 1. 2 2. Problem Statement 3 3. Literature Review 4-6 4. Discussion 7-13 5. Conclusion 14 6. Reference List 15 7. Attachment 16-17Document17 pagesNO Particular Pages 1. 2 2. Problem Statement 3 3. Literature Review 4-6 4. Discussion 7-13 5. Conclusion 14 6. Reference List 15 7. Attachment 16-17Fardzli MatjakirNo ratings yet
- Pain Management in HemophiliaDocument15 pagesPain Management in HemophiliaErnesto GariNo ratings yet
- Whyismypatient Bleedingorbruising?: Natalia Rydz,, Paula D. JamesDocument24 pagesWhyismypatient Bleedingorbruising?: Natalia Rydz,, Paula D. Jamescamila perillaNo ratings yet
- Critical Limb IschemiaDocument2 pagesCritical Limb IschemiaDorin DvornicNo ratings yet
- Nic Noc Risk For Bleeding (MB Anik)Document3 pagesNic Noc Risk For Bleeding (MB Anik)Luthfiy IrfanasruddinNo ratings yet
- Deep Vein Thrombosis: Case PresentationDocument19 pagesDeep Vein Thrombosis: Case PresentationFebriadi RNo ratings yet
- Case Study on Effects of Drugs on Blood PressureDocument6 pagesCase Study on Effects of Drugs on Blood Pressureania ojedaNo ratings yet
- Disseminated Intravascular Coagulation (DIC) CaseDocument5 pagesDisseminated Intravascular Coagulation (DIC) CaseTariqNo ratings yet
- Leech TherapyDocument3 pagesLeech Therapyagung231194No ratings yet
- Bleeding Disorders in Ortho PDFDocument4 pagesBleeding Disorders in Ortho PDFkiran kaurNo ratings yet
- The Venous Ulcer Continues ToDocument8 pagesThe Venous Ulcer Continues ToAsmat BurhanNo ratings yet
- Running Head: Deep Vein ThrombosisDocument7 pagesRunning Head: Deep Vein ThrombosisSUJANABHISEKHNo ratings yet
- OsteomyelitisDocument23 pagesOsteomyelitisGail ZantuaNo ratings yet
- HSHDDocument193 pagesHSHDRianda AkmalNo ratings yet
- Journal of Ayurveda and Integrative Medicine: S. Choudhury, A.R. Khuda-BukhshDocument4 pagesJournal of Ayurveda and Integrative Medicine: S. Choudhury, A.R. Khuda-BukhshNisa AriyantiiNo ratings yet
- Polycythemia Definition.: Low-Dose Aspirin Ruxolitinib BusulfanDocument14 pagesPolycythemia Definition.: Low-Dose Aspirin Ruxolitinib BusulfanArianna Jasmine MabungaNo ratings yet
- Mgso4 and Glycerine For Edema N ThrombophlebitisDocument18 pagesMgso4 and Glycerine For Edema N ThrombophlebitisPreethi IyengarNo ratings yet
- What Is CoagulationDocument6 pagesWhat Is CoagulationKang Wenn LeeNo ratings yet
- RHEUMATOID ARTHRITIS DR DON J SCOTT BERIN G BHMS (MEDICAL OFFICER) PDFDocument6 pagesRHEUMATOID ARTHRITIS DR DON J SCOTT BERIN G BHMS (MEDICAL OFFICER) PDFDr-Don JamesScott BerinGraceNo ratings yet
- HematologyDocument5 pagesHematologytabithaNo ratings yet
- Safe Blood Transfusion PracticeDocument29 pagesSafe Blood Transfusion PracticecollinsmagNo ratings yet
- OsteomyelitisDocument3 pagesOsteomyelitisHabib IrwanNo ratings yet
- Hemorrhage Lec 1Document30 pagesHemorrhage Lec 1balachris64No ratings yet
- MED SURG III- Food for thought reviewDocument24 pagesMED SURG III- Food for thought reviewHannah PerkinsNo ratings yet
- Leg Ulcer, What Do You Stand byDocument2 pagesLeg Ulcer, What Do You Stand byFree PizzaNo ratings yet
- The Incidence of Thrombophlebitis Following The Use of Peripheral Intravenous Cannula in Post-Operative Patients A Prospective Observational StudyDocument4 pagesThe Incidence of Thrombophlebitis Following The Use of Peripheral Intravenous Cannula in Post-Operative Patients A Prospective Observational StudyIOSRjournalNo ratings yet
- Approach to Diagnosing Bleeding DisordersDocument44 pagesApproach to Diagnosing Bleeding DisordersSkAliHassanNo ratings yet
- Recurrent Leg Ulcers in A Young Man With HyperhomoDocument4 pagesRecurrent Leg Ulcers in A Young Man With HyperhomoalfonsoNo ratings yet
- PlebitisDocument5 pagesPlebitisIndra PutraNo ratings yet
- Ulcerated Lower LimbDocument4 pagesUlcerated Lower LimbSelamet SusantoNo ratings yet
- Chapter 30 Important Points MedsurgDocument7 pagesChapter 30 Important Points Medsurgelizabeth100% (1)
- A Simple Guide to Thrombophlebitis, Diagnosis, Treatment and Related ConditionsFrom EverandA Simple Guide to Thrombophlebitis, Diagnosis, Treatment and Related ConditionsNo ratings yet
- Current and Future Issues in Hemophilia CareFrom EverandCurrent and Future Issues in Hemophilia CareEmérito Carlos Rodríguez-MerchánNo ratings yet
- Resume Manoj R.kandoiDocument9 pagesResume Manoj R.kandoiManoj KandoiNo ratings yet
- Anatomy of Shoulder JointDocument65 pagesAnatomy of Shoulder Jointmanoj ramlal kandoi100% (1)
- IACP Clinic Arthroplasty BrochureDocument6 pagesIACP Clinic Arthroplasty Brochuremanoj ramlal kandoiNo ratings yet
- Neuropathic ArthritisDocument5 pagesNeuropathic Arthritismanoj ramlal kandoiNo ratings yet
- Living With ArthritisDocument6 pagesLiving With Arthritismanoj ramlal kandoiNo ratings yet
- OsteoarthritisDocument15 pagesOsteoarthritismanoj ramlal kandoi100% (1)
- Low BackacheDocument23 pagesLow Backachemanoj ramlal kandoiNo ratings yet
- Infectious ArthritisDocument15 pagesInfectious Arthritismanoj ramlal kandoiNo ratings yet
- Juveline ArthritisDocument6 pagesJuveline ArthritisManoj KandoiNo ratings yet
- LS Spanish Year 7 POS-1Document9 pagesLS Spanish Year 7 POS-1NEHALL GOYALNo ratings yet
- 1st International Conference On Foreign Language Teaching and Applied Linguistics (Sarajevo, 5-7 May 2011)Document38 pages1st International Conference On Foreign Language Teaching and Applied Linguistics (Sarajevo, 5-7 May 2011)Jasmin Hodžić100% (2)
- Ich Validation 2qaDocument9 pagesIch Validation 2qaBishal AdhikariNo ratings yet
- Acts that may or may not be delegated to agentsDocument1 pageActs that may or may not be delegated to agentsEarl Vincent VistaNo ratings yet
- Puddu v. 6D Global Tech. - Securities Complaint PDFDocument57 pagesPuddu v. 6D Global Tech. - Securities Complaint PDFMark JaffeNo ratings yet
- Cyber Security Module 1Document4 pagesCyber Security Module 1silentnightNo ratings yet
- The Myth of Scientific Miracles in The KoranDocument13 pagesThe Myth of Scientific Miracles in The KoranDoctor Jones33% (3)
- Philippine Supreme Court Decisions on Constitutionality of LawsDocument64 pagesPhilippine Supreme Court Decisions on Constitutionality of Lawswesternwound82No ratings yet
- The Legend of Magat RiverDocument1 pageThe Legend of Magat RiverMichael Clinton DionedaNo ratings yet
- Left Movement in India Before IndependenceDocument3 pagesLeft Movement in India Before IndependenceMahesh KumarNo ratings yet
- Classroom Management and DisciplineDocument2 pagesClassroom Management and DisciplineMonaida Umpar IbrahimNo ratings yet
- The Role of Social Media On Leisure Preferences - A Research On The Participants of Outdoor Recreation Activities (#263492) - 230009Document10 pagesThe Role of Social Media On Leisure Preferences - A Research On The Participants of Outdoor Recreation Activities (#263492) - 230009Stella PadillaNo ratings yet
- Surviving A Zombie ApocalypseDocument4 pagesSurviving A Zombie ApocalypseSarah SmithNo ratings yet
- Tawassulan Fik TjakrabuanaDocument6 pagesTawassulan Fik TjakrabuanafikditasresNo ratings yet
- MA Urdu Revised Syllabus 2022-23Document35 pagesMA Urdu Revised Syllabus 2022-23Mazhar KhanNo ratings yet
- Using ABAQUS to Reduce Tire Belt Edge StressesDocument10 pagesUsing ABAQUS to Reduce Tire Belt Edge StressesGautam SharmaNo ratings yet
- Ethics in BankingDocument8 pagesEthics in BankingMarwa AleiaiwiNo ratings yet
- Tang Re CIA 2 enDocument20 pagesTang Re CIA 2 enDimitris TsagkoudisNo ratings yet
- The Killing Fields of Assam: Myth and Reality of Its Muslim ImmigrationDocument10 pagesThe Killing Fields of Assam: Myth and Reality of Its Muslim ImmigrationAlHittin100% (1)
- Overexploitation of Parrots in The NeotropicsDocument6 pagesOverexploitation of Parrots in The NeotropicsElenananaNo ratings yet
- List of Intel Core I3 MicroprocessorsDocument3 pagesList of Intel Core I3 MicroprocessorsKing 79100% (1)
- FP1 Proof by Induction MSDocument6 pagesFP1 Proof by Induction MSBrendon MuriraNo ratings yet