You might also like
- 1477 PDFDocument5 pages1477 PDFAjima UkpeNo ratings yet
- 2015 04 20 Visitor Supporting Documents Guide - Final 2 - CLEANDocument8 pages2015 04 20 Visitor Supporting Documents Guide - Final 2 - CLEANSiberNo ratings yet
- 4 - Health Information Management. 2Document106 pages4 - Health Information Management. 2Ajima UkpeNo ratings yet
- This Time QuotesDocument3 pagesThis Time QuotesAjima UkpeNo ratings yet
- Nuclear Magnetic Resonance 2Document17 pagesNuclear Magnetic Resonance 2Ajima UkpeNo ratings yet
- Assay List: Drug Matrix Detection Sample Internal Standard Range LloqDocument2 pagesAssay List: Drug Matrix Detection Sample Internal Standard Range LloqAjima UkpeNo ratings yet
- Assay List: Drug Matrix Detection Sample Internal Standard Range LloqDocument2 pagesAssay List: Drug Matrix Detection Sample Internal Standard Range LloqAjima UkpeNo ratings yet
- NUS List PDFDocument46 pagesNUS List PDFAjima UkpeNo ratings yet
- Brigham Powerpoint ch01Document17 pagesBrigham Powerpoint ch01AhsanNo ratings yet
- Mergers and DivestituresDocument18 pagesMergers and DivestituresAhsanNo ratings yet
- Materials and Methods: 3.1. Pharmacognosy 3.1.1. Collection of Plant MaterialsDocument34 pagesMaterials and Methods: 3.1. Pharmacognosy 3.1.1. Collection of Plant MaterialsAjima UkpeNo ratings yet
- The Basics of Capital Budgeting: Should We Build This Plant?Document31 pagesThe Basics of Capital Budgeting: Should We Build This Plant?AhsanNo ratings yet
- Woodward Fieser Rules PDFDocument5 pagesWoodward Fieser Rules PDFRaymond May100% (1)
- Extinction CoefficientsDocument3 pagesExtinction CoefficientshumusdelombrizNo ratings yet
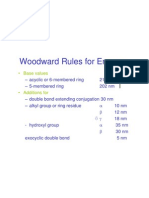
- Woodward Rules For Enones: - Base ValuesDocument1 pageWoodward Rules For Enones: - Base ValuesAjima UkpeNo ratings yet
- Shapes of MoleculesDocument6 pagesShapes of MoleculesAjima UkpeNo ratings yet
- 1997 Stegeman Cyp CBPDocument16 pages1997 Stegeman Cyp CBPAjima UkpeNo ratings yet
- 2013 14 AwardeeDocument4 pages2013 14 AwardeeAjima UkpeNo ratings yet
- PSTD Families eDocument20 pagesPSTD Families eAjima UkpeNo ratings yet
- Infrared SpectrosDocument38 pagesInfrared Spectrosfazraz100% (11)
- Calibration Curve for Artemether HydrolysisDocument1 pageCalibration Curve for Artemether HydrolysisAjima UkpeNo ratings yet
- Session Three - PTSD and Its Impact On The FamilyDocument15 pagesSession Three - PTSD and Its Impact On The FamilyAjima UkpeNo ratings yet
- AntioxDocument5 pagesAntioxAjima UkpeNo ratings yet
- RaddecayDocument5 pagesRaddecayAjima UkpeNo ratings yet
- AntioxDocument5 pagesAntioxAjima UkpeNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (894)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Ipo Exam Revised SyllabusDocument1 pageIpo Exam Revised Syllabusজ্যোতিৰ্ময় বসুমতাৰীNo ratings yet
- Palgrave Handbook of Research in Historical Culture and EducationDocument847 pagesPalgrave Handbook of Research in Historical Culture and EducationGonzalo Garcia100% (1)
- Critique On A Film Director's Approach To Managing CreativityDocument2 pagesCritique On A Film Director's Approach To Managing CreativityDax GaffudNo ratings yet
- A.2.3. Passive Transport Systems MCQsDocument3 pagesA.2.3. Passive Transport Systems MCQsPalanisamy SelvamaniNo ratings yet
- Understanding Culture, Society and PoliticsDocument62 pagesUnderstanding Culture, Society and PoliticsTeds TV89% (84)
- MVJUSTINIANI - BAFACR16 - INTERIM ASSESSMENT 1 - 3T - AY2022 23 With Answer KeysDocument4 pagesMVJUSTINIANI - BAFACR16 - INTERIM ASSESSMENT 1 - 3T - AY2022 23 With Answer KeysDe Gala ShailynNo ratings yet
- PM - Network Analysis CasesDocument20 pagesPM - Network Analysis CasesImransk401No ratings yet
- English Skills BookDocument49 pagesEnglish Skills BookAngela SpadeNo ratings yet
- Presentation On Ich Topics & Guidelines With A Special Reference ToDocument79 pagesPresentation On Ich Topics & Guidelines With A Special Reference ToVidyaNo ratings yet
- IE399 Summer Training ReportDocument17 pagesIE399 Summer Training ReportgokanayazNo ratings yet
- National Products Classification Code For Services in IndiaDocument92 pagesNational Products Classification Code For Services in Indiakalanemi0% (2)
- Moderntheater 170210003221 PDFDocument80 pagesModerntheater 170210003221 PDFDycan MikeNo ratings yet
- SOP for Troubleshooting LT ACB IssuesDocument9 pagesSOP for Troubleshooting LT ACB IssuesAkhilesh Kumar SinghNo ratings yet
- Relay Coordination Using Digsilent PowerFactoryDocument12 pagesRelay Coordination Using Digsilent PowerFactoryutshab.ghosh2023No ratings yet
- Neonatal SepsisDocument87 pagesNeonatal Sepsisyhanne100% (129)
- Zhihua Yao - Dignaga and The 4 Types of Perception (JIP 04)Document24 pagesZhihua Yao - Dignaga and The 4 Types of Perception (JIP 04)Carlos Caicedo-Russi100% (1)
- Digital Citizenship Initiative To Better Support The 21 Century Needs of StudentsDocument3 pagesDigital Citizenship Initiative To Better Support The 21 Century Needs of StudentsElewanya UnoguNo ratings yet
- OLA CAB MARKET ANALYSIS AND TRENDSDocument55 pagesOLA CAB MARKET ANALYSIS AND TRENDSnitin gadkariNo ratings yet
- Where On Earth Can Go Next?: AppleDocument100 pagesWhere On Earth Can Go Next?: Applepetrushevski_designeNo ratings yet
- Ogl422 Milestone Three Team 11 Intro Training Session For Evergreen MGT Audion Recording Due 2022apr18 8 30 PM PST 11 30pm EstDocument14 pagesOgl422 Milestone Three Team 11 Intro Training Session For Evergreen MGT Audion Recording Due 2022apr18 8 30 PM PST 11 30pm Estapi-624721629No ratings yet
- The Slave Trade and The British Empire An Audit of Commemoration in WalesDocument133 pagesThe Slave Trade and The British Empire An Audit of Commemoration in WaleslegoarkeologNo ratings yet
- The Life and Works of Jose RizalDocument20 pagesThe Life and Works of Jose RizalBemtot Blanquig100% (1)
- The Etteilla Tarot: Majors & Minors MeaningsDocument36 pagesThe Etteilla Tarot: Majors & Minors MeaningsRowan G100% (1)
- EQ - Module - Cantilever MethodDocument17 pagesEQ - Module - Cantilever MethodAndrea MalateNo ratings yet
- STERNOL Specification ToolDocument15 pagesSTERNOL Specification ToolMahdyZargarNo ratings yet
- Lesson Plan 2018-2019 Term 1Document205 pagesLesson Plan 2018-2019 Term 1Athlyn DurandNo ratings yet
- Strain Gauge Sensor PDFDocument12 pagesStrain Gauge Sensor PDFMario Eduardo Santos MartinsNo ratings yet
- The Bloodless GospelDocument7 pagesThe Bloodless GospelKJVNo ratings yet
- AJK Newslet-1Document28 pagesAJK Newslet-1Syed Raza Ali RazaNo ratings yet
- Plant Air Centrifugal Compressors: Turbo-Air Series Featuring Oil-Free AirDocument20 pagesPlant Air Centrifugal Compressors: Turbo-Air Series Featuring Oil-Free AirSharad KokateNo ratings yet