You might also like
- Physiology and Pathology of Physical and Psychological StressDocument60 pagesPhysiology and Pathology of Physical and Psychological StressBrunoNo ratings yet
- Prof - Dr.Indumathy Santhanam (ICH) In-Hospital Care of Trauma Patients in Tamil Nadu - Current Systems For Management of ChildrenDocument40 pagesProf - Dr.Indumathy Santhanam (ICH) In-Hospital Care of Trauma Patients in Tamil Nadu - Current Systems For Management of ChildrenBrunoNo ratings yet
- Prof DR Mark Fitzgerald Integrated In-Hospital Trauma Care - Building Blocks That Save LivesDocument42 pagesProf DR Mark Fitzgerald Integrated In-Hospital Trauma Care - Building Blocks That Save LivesBrunoNo ratings yet
- Ms Ellaine Boo Role of Trauma NursingDocument35 pagesMs Ellaine Boo Role of Trauma NursingBrunoNo ratings yet
- Prof DR Amit Gupta AITSC Trauma Registry & Trauma Quality Improvement in IndiaDocument77 pagesProf DR Amit Gupta AITSC Trauma Registry & Trauma Quality Improvement in IndiaBruno50% (2)
- Mrs. Sulochana (RGGGH) Current Status of Trauma Nursing in TNDocument11 pagesMrs. Sulochana (RGGGH) Current Status of Trauma Nursing in TNBrunoNo ratings yet
- Hub and Spoke Model For STEMI Management - Tamil Nadu ModelDocument16 pagesHub and Spoke Model For STEMI Management - Tamil Nadu ModelBrunoNo ratings yet
- DR - Raja S Vignesh (Thoothukudi Medical College) in Hospital Care of Patient by NeurosurgeonDocument25 pagesDR - Raja S Vignesh (Thoothukudi Medical College) in Hospital Care of Patient by NeurosurgeonBrunoNo ratings yet
- DR - Rajesh CMO (RGGGH) In-Hospital Care of Trauma Patients in Tamil Nadu - Current Systems For Management of AdultsDocument32 pagesDR - Rajesh CMO (RGGGH) In-Hospital Care of Trauma Patients in Tamil Nadu - Current Systems For Management of AdultsBruno100% (1)
- DR - Joseph Mathew: Trauma Units and Team WorkDocument39 pagesDR - Joseph Mathew: Trauma Units and Team WorkBrunoNo ratings yet
- DR - Ramana Rao Pre-Hospital Services in Tamil NaduDocument73 pagesDR - Ramana Rao Pre-Hospital Services in Tamil NaduBrunoNo ratings yet
- Prof DR Mark Fitzgerald What Is A Trauma System and Trauma System ComponentsDocument36 pagesProf DR Mark Fitzgerald What Is A Trauma System and Trauma System ComponentsBrunoNo ratings yet
- DR - Thambaiah (Cuddalore GH) in Hospital Care of Patients by OrthopaedicianDocument36 pagesDR - Thambaiah (Cuddalore GH) in Hospital Care of Patients by OrthopaedicianBruno100% (1)
- TAEI NTRI WorkshopDocument16 pagesTAEI NTRI WorkshopBrunoNo ratings yet
- Prof Venkatesh Balasubramanian Current State Road Accident Database and Requirements For Integration of A Trauma RegistryDocument37 pagesProf Venkatesh Balasubramanian Current State Road Accident Database and Requirements For Integration of A Trauma RegistryBrunoNo ratings yet
- DR Joseph Mathew Designation of Trauma Hospitals in A Trauma SystemDocument29 pagesDR Joseph Mathew Designation of Trauma Hospitals in A Trauma SystemBrunoNo ratings yet
- Mr. Dayanand Kataria, IAS Transport Commissioner Road Safety StatusDocument25 pagesMr. Dayanand Kataria, IAS Transport Commissioner Road Safety StatusBruno100% (1)
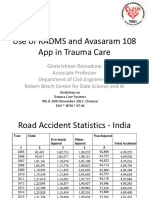
- Prof Gita Krishnan Ramadurai Use of RADAMS and 108 Avasaram App in Trauma CareDocument21 pagesProf Gita Krishnan Ramadurai Use of RADAMS and 108 Avasaram App in Trauma CareBrunoNo ratings yet
- Prof DR Peter Cameron Measuring The Quality of Trauma Systems and In-Hospital Trauma CareDocument46 pagesProf DR Peter Cameron Measuring The Quality of Trauma Systems and In-Hospital Trauma CareBrunoNo ratings yet
- Why Tamil Nadu Model Works Better in Eradicating Organ SaleDocument52 pagesWhy Tamil Nadu Model Works Better in Eradicating Organ SaleBrunoNo ratings yet
- How Tamil Nadu Eradicated Organ SaleDocument108 pagesHow Tamil Nadu Eradicated Organ SaleBrunoNo ratings yet
- Ian Patrick Pre-Hospital Systems in Australia Key Components of The Pre-Hospital System in Australia and Best Buys For Tamil NaduDocument26 pagesIan Patrick Pre-Hospital Systems in Australia Key Components of The Pre-Hospital System in Australia and Best Buys For Tamil NaduBrunoNo ratings yet
- Doctors' Role in Tackling Organ TradeDocument70 pagesDoctors' Role in Tackling Organ TradeBrunoNo ratings yet
- DR - Darez Ahamed Vision For Tamil NaduDocument6 pagesDR - Darez Ahamed Vision For Tamil NaduBrunoNo ratings yet
- AR Rahman PDFDocument405 pagesAR Rahman PDFPitchai BalaNo ratings yet
- TN Gazette 47 of 2013 Part VI Section 4Document84 pagesTN Gazette 47 of 2013 Part VI Section 4BrunoNo ratings yet
- Neurosurgeon For A Social CauseDocument55 pagesNeurosurgeon For A Social CauseBrunoNo ratings yet
- Neurology, Neurosurgery MCQ PointsDocument32 pagesNeurology, Neurosurgery MCQ PointsBruno86% (7)
- NEET PG 2013 Rank List of Eligible CandidatesDocument256 pagesNEET PG 2013 Rank List of Eligible CandidatesBruno75% (8)
- HMIS - Health Management Information System - Government of Tamil NaduDocument12 pagesHMIS - Health Management Information System - Government of Tamil NaduBruno100% (1)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5783)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (72)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Assessment of The Critically Ill PatientsDocument30 pagesAssessment of The Critically Ill Patientsefancoolhand09No ratings yet
- Lung Sounds 5Document1 pageLung Sounds 5Kyle LatayanNo ratings yet
- Bag-Mask Ventillation PDFDocument6 pagesBag-Mask Ventillation PDFHaris PapadopoulosNo ratings yet
- COPD Case PresentationDocument15 pagesCOPD Case PresentationBola Kwentua29% (7)
- Pulmonary Pathophysiology - The Essentials (PULMONARY PATHOPHYSIOLOGY (WEST) ), 8th Edition (2012)Document193 pagesPulmonary Pathophysiology - The Essentials (PULMONARY PATHOPHYSIOLOGY (WEST) ), 8th Edition (2012)Mircea Vleoanga100% (1)
- First Aid and CPR Training GuideDocument73 pagesFirst Aid and CPR Training GuidechimaraiykeNo ratings yet
- Pediatric PneumoniaDocument12 pagesPediatric PneumoniaKrystal Migo Denolo ContrerasNo ratings yet
- Acute Bronchitis Case StudyDocument6 pagesAcute Bronchitis Case Studyulka0750% (2)
- Needle CricothyroidotomyDocument9 pagesNeedle Cricothyroidotomyhatem alsrour100% (2)
- NCP Ineffective Airway Clearance Related To The Accumulation of Exudates in The Alveoli TBDocument3 pagesNCP Ineffective Airway Clearance Related To The Accumulation of Exudates in The Alveoli TBMa. Elaine Carla Tating0% (1)
- I Can'T Breathe If Breathing Is Without: Bronchial AsthmaDocument33 pagesI Can'T Breathe If Breathing Is Without: Bronchial AsthmaklamorenaNo ratings yet
- Key Changes Gold 2023Document15 pagesKey Changes Gold 2023joao cNo ratings yet
- Centrilobular Fibrosis in Fibrotic (Chronic)Document8 pagesCentrilobular Fibrosis in Fibrotic (Chronic)yuriescaidaNo ratings yet
- Chem 40.1 Msds Exer 6Document7 pagesChem 40.1 Msds Exer 6Angela Sietereales RamosNo ratings yet
- Volume Targeted VentilationDocument4 pagesVolume Targeted VentilationAli Mohamed AbdallaNo ratings yet
- Rangkuman Materi: Sekolah Menengah Atas (Sma) Negeri 1 BatuDocument55 pagesRangkuman Materi: Sekolah Menengah Atas (Sma) Negeri 1 BatuHusain AlanNo ratings yet
- Acid Base DisturbancesDocument34 pagesAcid Base DisturbancesTracy100% (1)
- Lower Respiratory Tract InfectionsDocument21 pagesLower Respiratory Tract InfectionsEzekiel ArtetaNo ratings yet
- Physiology Question Bank FinalDocument16 pagesPhysiology Question Bank Finalatefmabood100% (2)
- Case Presentation 1 CopdDocument48 pagesCase Presentation 1 CopdPreeti ChouhanNo ratings yet
- Bronchitis: Edited by Ignacio Martín-LoechesDocument200 pagesBronchitis: Edited by Ignacio Martín-LoechesskilmagNo ratings yet
- Fundamentals of NursingDocument268 pagesFundamentals of Nursinguhta100% (1)
- g6 Science Text 03Document42 pagesg6 Science Text 03a.rodriguezmarcoNo ratings yet
- Chest Tube DrainageDocument3 pagesChest Tube DrainageCyndi Jane Bandin Cruzata100% (1)
- Anatomy and Physiology: The Respiratory SystemDocument82 pagesAnatomy and Physiology: The Respiratory SystemMaria Angelique Ofciar100% (2)
- Nursing Care Plan Assessment Nursing Diagnosis Nursing Goal Nursing Intervention Rationale Outcome Criteria Actual EvaluationDocument4 pagesNursing Care Plan Assessment Nursing Diagnosis Nursing Goal Nursing Intervention Rationale Outcome Criteria Actual EvaluationPabhat Kumar50% (2)
- Adult Demo LungDocument4 pagesAdult Demo LungArtem 521No ratings yet
- Grade 9 Science LM Complete DraftDocument105 pagesGrade 9 Science LM Complete DraftJerimiah Miranda74% (31)
- Clinical Performance Evaluation → Asthma ACR-DIDDocument1 pageClinical Performance Evaluation → Asthma ACR-DIDveronica100% (1)
- Breathing DifficultyDocument13 pagesBreathing DifficultygivamathanNo ratings yet