You might also like
- Essentials of Internal MedicineDocument832 pagesEssentials of Internal MedicineEmanuelMC100% (74)
- LaryngitisDocument24 pagesLaryngitisfatihahannisahumaira100% (1)
- DM Care PlanDocument9 pagesDM Care PlanHarish Kumar KumawatNo ratings yet
- Respiratory and Circulatory SystemsDocument3 pagesRespiratory and Circulatory SystemsJeffrey Costan100% (1)
- Nursing Care Plan for a Diabetic Patient with Dehydration and FatigueDocument9 pagesNursing Care Plan for a Diabetic Patient with Dehydration and FatigueDanica Salinas100% (1)
- Anatomy Supertable PDFDocument14 pagesAnatomy Supertable PDFAlex Ondevilla100% (1)
- Diabetes Mellitus NCPDocument7 pagesDiabetes Mellitus NCPjfgnzls182892% (12)
- NCPDocument7 pagesNCPAbbie TantengcoNo ratings yet
- Self Care DeficitDocument4 pagesSelf Care DeficitEllaine RamirezNo ratings yet
- MI Chest Pain AssessmentDocument5 pagesMI Chest Pain AssessmentDharline Abbygale Garvida AgullanaNo ratings yet
- NGT Enteral Feeding CareDocument8 pagesNGT Enteral Feeding CareSheng GosepNo ratings yet
- NGT Enteral Feeding CareDocument8 pagesNGT Enteral Feeding CareSheng GosepNo ratings yet
- Intermittent Fasting For Women: A Beginner’s Transformation Made EasyFrom EverandIntermittent Fasting For Women: A Beginner’s Transformation Made EasyNo ratings yet
- Cha 24 Tortora Respiratory SystemDocument12 pagesCha 24 Tortora Respiratory Systemsrinivas ceoNo ratings yet
- Optional (AEMT), Optional (Paramedic)Document76 pagesOptional (AEMT), Optional (Paramedic)Mark ReinhardtNo ratings yet
- NCPDocument3 pagesNCPbjhilarioNo ratings yet
- Enteral Feeding Nursing Care PlanDocument2 pagesEnteral Feeding Nursing Care PlanCyrus De Asis93% (15)
- NCLEX Questions PulmDocument27 pagesNCLEX Questions PulmAnthony Hawley100% (2)
- Nursing Care PlanDocument10 pagesNursing Care PlanGinel Laquiores100% (1)
- Drug Study and NCP!Document8 pagesDrug Study and NCP!Abegail Abaygar100% (1)
- ARDS Respiratory Distress SyndromeDocument49 pagesARDS Respiratory Distress Syndromesonam yadav67% (3)
- Diabetic patient wound careDocument7 pagesDiabetic patient wound careMichael Anthony Cardenas Macaballug67% (3)
- NCP and Problems FinalDocument8 pagesNCP and Problems FinalRina CebreroNo ratings yet
- 1) Nursing Careplan For FeverDocument9 pages1) Nursing Careplan For FeverY. Beatrice AbigailNo ratings yet
- Nursing Care Plans for Pancreatitis PatientDocument10 pagesNursing Care Plans for Pancreatitis PatientClaire Alcantara50% (2)
- NCPDocument4 pagesNCPAbegail Abaygar100% (1)
- Care of neonate on ventilatorDocument7 pagesCare of neonate on ventilatorAmy LalringhluaniNo ratings yet
- NCP Risk For FallDocument20 pagesNCP Risk For FallRen Ren Determinado86% (7)
- NCPDocument1 pageNCPAlynna ValbuenaNo ratings yet
- Diabetes Mellitus Type 2 NotesDocument5 pagesDiabetes Mellitus Type 2 NotesAimee Kaye DetablanNo ratings yet
- NCP (Fatigue)Document1 pageNCP (Fatigue)student_019100% (1)
- NCP ImbalancedDocument7 pagesNCP ImbalancedSasha FongNo ratings yet
- Nursing Care PlanDocument9 pagesNursing Care PlanjmichaelaNo ratings yet
- Cues Nursing Diagnosis Scientific Reason Planning Intervention Rationale EvaluationDocument6 pagesCues Nursing Diagnosis Scientific Reason Planning Intervention Rationale EvaluationKatrina Ponce86% (7)
- GastroenteritisDocument8 pagesGastroenteritistanlimdania100% (3)
- NCP FinalDocument18 pagesNCP FinalJessica Medina100% (1)
- NCP For MGDocument1 pageNCP For MGSandra MedinaNo ratings yet
- CBT Sample MCQs - Source Royal Marsden ANSWERSDocument16 pagesCBT Sample MCQs - Source Royal Marsden ANSWERSarchana100% (6)
- Nursing Care PlanDocument3 pagesNursing Care PlanCristina L. JaysonNo ratings yet
- NCPDocument7 pagesNCPBeverLyNo ratings yet
- Nursing Care Plans for Stroke PtDocument13 pagesNursing Care Plans for Stroke PtJuls Flares SycaycoNo ratings yet
- NCP Activity IntoleranceDocument3 pagesNCP Activity Intolerancekeiii_21No ratings yet
- NCPDocument8 pagesNCPJose Benit DelacruzNo ratings yet
- NCPDocument10 pagesNCPNefre Dayap DarrocaNo ratings yet
- Nursing Care PlanDocument7 pagesNursing Care PlantinnnnnnnnnnnnnNo ratings yet
- Actual NCPDocument2 pagesActual NCPbaki0146No ratings yet
- Drug StudyDocument4 pagesDrug StudyHennah ReblandoNo ratings yet
- NCP FinalDocument7 pagesNCP FinalAkira MizukamiNo ratings yet
- Nursing Diagnosis: Fatigue related to decreased muscular strengthDocument2 pagesNursing Diagnosis: Fatigue related to decreased muscular strengthAna Ramos LopezNo ratings yet
- Nursing Care PlansDocument6 pagesNursing Care PlansTwobee Kriz LeghidNo ratings yet
- Dermatomyositis NCPDocument3 pagesDermatomyositis NCPMakki MarcosNo ratings yet
- Assessment Diagnosis Planning Intervention Rationale EvaluationDocument10 pagesAssessment Diagnosis Planning Intervention Rationale EvaluationLean Ashly Tuddao Macarubbo0% (1)
- Nursing Care Plan (CASE STUDY DENGUE)Document10 pagesNursing Care Plan (CASE STUDY DENGUE)NiooleNo ratings yet
- Assessment Data Nursing Diagnosis Planning Intervention Rationale EvaluationDocument2 pagesAssessment Data Nursing Diagnosis Planning Intervention Rationale EvaluationCrystelle MonaresNo ratings yet
- NCPDocument2 pagesNCPJoey PolicarNo ratings yet
- Subjective Cues: Short Term GoalDocument2 pagesSubjective Cues: Short Term GoalcarissagacutnoNo ratings yet
- Managing Diabetes and RisksDocument8 pagesManaging Diabetes and RisksChristopher LontocNo ratings yet
- Imblanced NutritionDocument2 pagesImblanced NutritionCristina L. JaysonNo ratings yet
- NCP Nursing Diagnosis: Activity IntoleranceDocument4 pagesNCP Nursing Diagnosis: Activity IntoleranceAngelica Orbase BelmonteNo ratings yet
- Ix. Nursing Care Plan: Asessment Nursing Diagnosis Scientific Explanation Planning Intervention Rationale EvaluationDocument5 pagesIx. Nursing Care Plan: Asessment Nursing Diagnosis Scientific Explanation Planning Intervention Rationale Evaluationemman_russelNo ratings yet
- Cervical Cancer ChemotherapyDocument6 pagesCervical Cancer ChemotherapyTheeya Quigao0% (1)
- NCPDocument10 pagesNCPannamargie07No ratings yet
- 5ncp AnemiaDocument8 pages5ncp Anemiabeverly_domingoNo ratings yet
- R: This Provides Baseline Measurement For Future Evaluation and Guides TherapyDocument4 pagesR: This Provides Baseline Measurement For Future Evaluation and Guides TherapyTyron ChuaNo ratings yet
- NCP For Impaired MobilityDocument4 pagesNCP For Impaired MobilityBettinaFernandoNo ratings yet
- NCP GrandcaseDocument5 pagesNCP GrandcaseSaima BataloNo ratings yet
- Nursing Care ManagementDocument40 pagesNursing Care ManagementɱΘΟθ CuasitoNo ratings yet
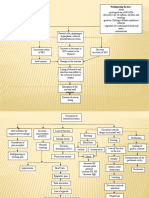
- Concept Map Nursing Care Plan for CVA, DM, HypertensionDocument3 pagesConcept Map Nursing Care Plan for CVA, DM, HypertensionFranklin A. Salaum III0% (2)
- Nourish A Comprehensive Guide to Healthy Eating and Sustainable LivingFrom EverandNourish A Comprehensive Guide to Healthy Eating and Sustainable LivingNo ratings yet
- Viii. Drug Study: Drug Action Indications Containdications Side / Adverse Reactions Nursing ConsiderationDocument18 pagesViii. Drug Study: Drug Action Indications Containdications Side / Adverse Reactions Nursing ConsiderationSheng GosepNo ratings yet
- Myasthemia GravisDocument11 pagesMyasthemia GravisSheng GosepNo ratings yet
- Gastroenteritis OverviewDocument5 pagesGastroenteritis OverviewSheng GosepNo ratings yet
- Hydralazine hydrochloride: Antihypertensive drug generic name, brand name, indications, adverse effectsDocument1 pageHydralazine hydrochloride: Antihypertensive drug generic name, brand name, indications, adverse effectsSheng Gosep100% (3)
- Anatomy of The Central Nervous SystemDocument3 pagesAnatomy of The Central Nervous SystemSheng GosepNo ratings yet
- Vitamin K3 Drug Generic Name, Brand, Uses, Side EffectsDocument2 pagesVitamin K3 Drug Generic Name, Brand, Uses, Side EffectsSheng GosepNo ratings yet
- Facts About Myasthenia GravisDocument14 pagesFacts About Myasthenia GravisSheng GosepNo ratings yet
- Personality Development NotesDocument11 pagesPersonality Development Notesvasantha_btechNo ratings yet
- Invasive Ductal Carcinoma: Group 13 ADocument3 pagesInvasive Ductal Carcinoma: Group 13 ASheng GosepNo ratings yet
- Heart Failure: Marvick F. Galima RNDocument42 pagesHeart Failure: Marvick F. Galima RNSheng GosepNo ratings yet
- Bpud, PathoDocument2 pagesBpud, PathoSheng GosepNo ratings yet
- 1.introduction To GeriatricsDocument45 pages1.introduction To Geriatricsbookstore wormNo ratings yet
- Understanding How Density Affects Weight in Different MediumsDocument72 pagesUnderstanding How Density Affects Weight in Different MediumsJiaYing WinNo ratings yet
- Home Based CareDocument34 pagesHome Based CaremewselectionsNo ratings yet
- 03 - Diffuse Pulmonary NodulesDocument13 pages03 - Diffuse Pulmonary NodulesOmar Guerrero Soto100% (1)
- Lore BookDocument131 pagesLore BookMárcio Machado Ribeiro (Jamesfoxbr)No ratings yet
- Hand Out 2 NCM 103 PrelimDocument3 pagesHand Out 2 NCM 103 PrelimLouisa Marie MirandaNo ratings yet
- Management of Respiratory Failure Ventilator.17Document9 pagesManagement of Respiratory Failure Ventilator.17Margarida ReisNo ratings yet
- Prone VentilationDocument20 pagesProne VentilationdeepaksolarNo ratings yet
- Mechanical Ventilation Troubleshooting Skill Respiratory Therapy COVID 19 Toolkit - 070420Document8 pagesMechanical Ventilation Troubleshooting Skill Respiratory Therapy COVID 19 Toolkit - 070420Sirgut TesfayeNo ratings yet
- BSC Nursing SyllDocument218 pagesBSC Nursing SyllKiran KhasaNo ratings yet
- Grade 11 Biology (SBI 3U1) Name: - Unit: Internal Systems Lab: Virtual Fetal Pig Dissection DateDocument3 pagesGrade 11 Biology (SBI 3U1) Name: - Unit: Internal Systems Lab: Virtual Fetal Pig Dissection DateSydney Drizis [Student]No ratings yet
- Broncho Ect As IsDocument28 pagesBroncho Ect As Ismeaza rorisaNo ratings yet
- Airway Clearance. Physiology, Pharmacology, Techniques, and Practice - Rubin, Hess 2007Document5 pagesAirway Clearance. Physiology, Pharmacology, Techniques, and Practice - Rubin, Hess 2007Maxi BoniniNo ratings yet
- Review in Science Circulatory System PulmonaryDocument3 pagesReview in Science Circulatory System PulmonaryElvie Jane P. MolatoNo ratings yet
- ASPEN Nutrition Support During Prone PositionDocument5 pagesASPEN Nutrition Support During Prone PositionAlimah YasminNo ratings yet
- The Anesthesia Gas MachineDocument28 pagesThe Anesthesia Gas MachineBianca RotaruNo ratings yet
- Course Outline For 125:355, Physiological Systems For Biomedical EngineersDocument2 pagesCourse Outline For 125:355, Physiological Systems For Biomedical EngineersbillNo ratings yet
- CH 11 Gas Exchange in HumansDocument4 pagesCH 11 Gas Exchange in HumansPranitha RaviNo ratings yet
- NCP Impaired Gas ExchangeDocument2 pagesNCP Impaired Gas ExchangeAlliah MayoNo ratings yet
- Apnea Testing For The Determination of Brain Death A Systematic Scoping ReviewDocument13 pagesApnea Testing For The Determination of Brain Death A Systematic Scoping Reviewrisna sariNo ratings yet