You might also like
- Physical Assessment and GordonsDocument14 pagesPhysical Assessment and GordonsRubelyn Joy LazarteNo ratings yet
- Adult Nasogastric Tube ProcedureDocument0 pagesAdult Nasogastric Tube ProcedureRubelyn Joy LazarteNo ratings yet
- Rom ExercisesDocument12 pagesRom ExercisesSandi Nelson100% (1)
- The Management of Patients With Acute Myocardial Infarction: Pocket GuidelinesDocument21 pagesThe Management of Patients With Acute Myocardial Infarction: Pocket GuidelinesRubelyn Joy LazarteNo ratings yet
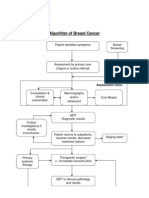
- Algorithm of Breast Cancer: Assessment ClinicDocument2 pagesAlgorithm of Breast Cancer: Assessment ClinicRubelyn Joy LazarteNo ratings yet
- Geriatric NursingDocument10 pagesGeriatric NursingRubelyn Joy LazarteNo ratings yet
- ReactionDocument5 pagesReactionRubelyn Joy LazarteNo ratings yet
- Case StudyDocument5 pagesCase StudyRubelyn Joy LazarteNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5784)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (72)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- How To Do Eyebrows - A Style Guide For Perfect EyebrowsDocument12 pagesHow To Do Eyebrows - A Style Guide For Perfect EyebrowsnatasyaNo ratings yet
- 30 91 1 PBasdjhasjdgasyfgaydgaydgawuDocument10 pages30 91 1 PBasdjhasjdgasyfgaydgaydgawuWilkus ParconNo ratings yet
- Aimcat 6Document22 pagesAimcat 6Shanawaz ArifNo ratings yet
- Supp B RRC 2015 LowResDocument360 pagesSupp B RRC 2015 LowResstoicea catalinNo ratings yet
- Heterocycles Essentials3-2009Document2 pagesHeterocycles Essentials3-2009Aravindan NatarajanNo ratings yet
- Guattari F.-The Machinic Unconscious - Essays in SchizoanalysisDocument366 pagesGuattari F.-The Machinic Unconscious - Essays in SchizoanalysisMiguel NevesNo ratings yet
- Social Self Destruction: A Secret War of Controlled ChaosDocument18 pagesSocial Self Destruction: A Secret War of Controlled ChaosAnthony Forwood80% (10)
- Implementing a Strategic Church PlanDocument3 pagesImplementing a Strategic Church PlanKaso MuseNo ratings yet
- Discover how monoclonal antibodies are produced using hybridoma technologyDocument32 pagesDiscover how monoclonal antibodies are produced using hybridoma technologykhanNo ratings yet
- Narciso D. Isidro JR.: Pamantasang Lungsod NG Manila Mba-Tep Organization and Management Dr. Neri Pescadera, PH.DDocument25 pagesNarciso D. Isidro JR.: Pamantasang Lungsod NG Manila Mba-Tep Organization and Management Dr. Neri Pescadera, PH.DDon87% (15)
- Emailing 11. Dr. Manoj Gupta - Pelvic RT PlanningDocument69 pagesEmailing 11. Dr. Manoj Gupta - Pelvic RT PlanningafshanNo ratings yet
- Pengumuman Hong Kong International Mathematical OlympiadDocument6 pagesPengumuman Hong Kong International Mathematical OlympiadEjaz ElfathNo ratings yet
- Philosophy - Robert Martin 1994 - The Philosophers Dictionary 2Nd Ed TextDocument251 pagesPhilosophy - Robert Martin 1994 - The Philosophers Dictionary 2Nd Ed TextSory WebNo ratings yet
- Integrated Communications Systems Modeling: A Model-Based Engineering ApproachDocument5 pagesIntegrated Communications Systems Modeling: A Model-Based Engineering ApproachRaghavan MuralidharanNo ratings yet
- In Christ Alone-chords-CDocument2 pagesIn Christ Alone-chords-CJill MontañoNo ratings yet
- Ajrak Print of GujratDocument4 pagesAjrak Print of GujratShivamNo ratings yet
- Distillation Column Hydrogen PeroxideDocument6 pagesDistillation Column Hydrogen PeroxideKatiane MesquitaNo ratings yet
- From The Bodies of Bees Classical and Christian Echoes in Surah Al-NahlDocument25 pagesFrom The Bodies of Bees Classical and Christian Echoes in Surah Al-Nahlkiedd_04No ratings yet
- HutcheonDocument8 pagesHutcheonMelanieNo ratings yet
- Job Evaluation Using Hay Method - Additional ClassDocument59 pagesJob Evaluation Using Hay Method - Additional Classanon_157474710100% (4)
- Clinically Important EnzymesDocument29 pagesClinically Important Enzymesonnumilla49No ratings yet
- Duryodhana Sows Seeds of DiscordDocument117 pagesDuryodhana Sows Seeds of DiscordSrikanth VNo ratings yet
- English Grammar & Vocabulary Practice TestDocument22 pagesEnglish Grammar & Vocabulary Practice TestAna Elena MarianNo ratings yet
- Books On Islam Jarir Bookstore KSADocument1 pageBooks On Islam Jarir Bookstore KSAygd4qy468cNo ratings yet
- 3.5 Standard Operations Research Models: Mathematical Modify ModelDocument2 pages3.5 Standard Operations Research Models: Mathematical Modify ModelAnonymous IjhB0kuFNo ratings yet
- The Effects of School Uniforms On Student Behavior and PerceptionDocument106 pagesThe Effects of School Uniforms On Student Behavior and PerceptionJorie GumateNo ratings yet
- Torts (Malicious Prosecution)Document9 pagesTorts (Malicious Prosecution)legalight100% (2)
- SoundsDocument9 pagesSoundssedif2No ratings yet
- Spellforce SubquestDocument28 pagesSpellforce Subquestd4v7dNo ratings yet
- Phlebotomy ManualDocument111 pagesPhlebotomy ManualMyra Buella100% (2)