You might also like
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (894)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Reversing Digestive MiseryDocument160 pagesReversing Digestive MiseryalanbwilliamsNo ratings yet
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- Dysphagia and Swallowing Disorders, MC Carty E. (2021)Document16 pagesDysphagia and Swallowing Disorders, MC Carty E. (2021)Irving Santiago SandovalNo ratings yet
- Effects of ObesityDocument48 pagesEffects of ObesityFairuz KangNo ratings yet
- Stomach-Esophagus MedCosmos Surgery - MCQDocument39 pagesStomach-Esophagus MedCosmos Surgery - MCQMike G100% (1)
- GCHVJKDocument1 pageGCHVJKAroNo ratings yet
- A A LalalalaDocument1 pageA A LalalalaAroNo ratings yet
- DDDD DDDD DDDD DDDD DDDD DDocument1 pageDDDD DDDD DDDD DDDD DDDD DAroNo ratings yet
- Eeeee EeeeeeeeeeeeeeeDocument1 pageEeeee EeeeeeeeeeeeeeeAroNo ratings yet
- Pro09 22Document6 pagesPro09 22AroNo ratings yet
- A Novel Prion Disease Associated With Diarrhea and Autonomic NeuropathyDocument11 pagesA Novel Prion Disease Associated With Diarrhea and Autonomic NeuropathyAroNo ratings yet
- Jurnal NeuroDocument9 pagesJurnal NeuroAroNo ratings yet
- TT TTTTT TTTTT TTTTTDocument1 pageTT TTTTT TTTTT TTTTTAroNo ratings yet
- Ok Ok Ok Ooo Ooookkkkk KDocument1 pageOk Ok Ok Ooo Ooookkkkk KAroNo ratings yet
- The Efficacy of Phonophoresis On Electrophysiological Studies of The Patients With Carpal Tunnel SyndromeDocument9 pagesThe Efficacy of Phonophoresis On Electrophysiological Studies of The Patients With Carpal Tunnel SyndromeAroNo ratings yet
- Epidemiological Characteristics of Acute Disseminated Encephalomyelitis in Nanchang, China: A Retrospective StudyDocument6 pagesEpidemiological Characteristics of Acute Disseminated Encephalomyelitis in Nanchang, China: A Retrospective StudyAroNo ratings yet
- PDFSig QFormal RepDocument1 pagePDFSig QFormal Repanon-549999100% (2)
- 22380488Document11 pages22380488AroNo ratings yet
- Unu UuuuuuuDocument1 pageUnu UuuuuuuAroNo ratings yet
- AaaaaaaDocument1 pageAaaaaaaAroNo ratings yet
- Eula Microsoft Visual StudioDocument3 pagesEula Microsoft Visual StudioqwwerttyyNo ratings yet
- Read Me! Credit! Password! Anything!Document1 pageRead Me! Credit! Password! Anything!masruri123No ratings yet
- Put Unused Plug-Ins in The Optional Directory.Document1 pagePut Unused Plug-Ins in The Optional Directory.andias04No ratings yet
- Heller's Myotomy vs. Balloon DilationDocument10 pagesHeller's Myotomy vs. Balloon DilationHeather PoushayNo ratings yet
- DFZGZDFDocument1 pageDFZGZDFAroNo ratings yet
- Eula Microsoft Visual StudioDocument3 pagesEula Microsoft Visual StudioqwwerttyyNo ratings yet
- AmenorrheaDocument16 pagesAmenorrheaAroNo ratings yet
- Journal of Feline Medicine and Surgery-2007-Baez-411-7Document8 pagesJournal of Feline Medicine and Surgery-2007-Baez-411-7AroNo ratings yet
- Afp - LPR 2Document6 pagesAfp - LPR 2sara ashariNo ratings yet
- Abdullah F. Owayed, MD Douglas M. Campbell, MD Elaine E. L. Wang, MD, FRCPCDocument8 pagesAbdullah F. Owayed, MD Douglas M. Campbell, MD Elaine E. L. Wang, MD, FRCPCadiospernitiNo ratings yet
- PHarma GiDocument28 pagesPHarma GiShahd KhatibNo ratings yet
- Club Life: The Delhi Gymkhana Club General Committee 2019-20Document20 pagesClub Life: The Delhi Gymkhana Club General Committee 2019-20Parvinder AroraNo ratings yet
- Alkaline, Protein, Low-Fat and Low-Acid Diet in Laryngopharyngeal Reflux Disease: Our Experience On 65 PatientsDocument12 pagesAlkaline, Protein, Low-Fat and Low-Acid Diet in Laryngopharyngeal Reflux Disease: Our Experience On 65 PatientsJosé Luis Arellano CorderoNo ratings yet
- Basic Care and Comfort (20 Items)Document11 pagesBasic Care and Comfort (20 Items)Ik-ik MiralNo ratings yet
- Drug StudyDocument8 pagesDrug StudyjovanneyNo ratings yet
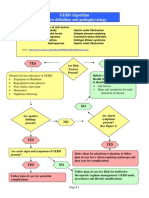
- GERD Algorithm Review Definition and Pathophysiology: NO YESDocument3 pagesGERD Algorithm Review Definition and Pathophysiology: NO YESdianyNo ratings yet
- Medsurg ReviewerDocument6 pagesMedsurg Reviewersherlyn galvanNo ratings yet
- Gastroplicatura en Pacientes Con Reflujo y Gastrectomia VerticalDocument9 pagesGastroplicatura en Pacientes Con Reflujo y Gastrectomia VerticalOoAldoONo ratings yet
- Cough: - Atheer AljthalinDocument15 pagesCough: - Atheer AljthalinAmira AlmutairiNo ratings yet
- Cingultus NeurogenicDocument14 pagesCingultus NeurogenicayunaNo ratings yet
- Pediatric Eating Assessment Tool-10 As An Indicator To Predict Aspirationin Children With Esophageal AtresiaDocument5 pagesPediatric Eating Assessment Tool-10 As An Indicator To Predict Aspirationin Children With Esophageal AtresiaANGIE GRAJALESNo ratings yet
- MS Gi7Document5 pagesMS Gi7Amiel Francisco ReyesNo ratings yet
- Esophagus Anatomy, Physiology and DiseasesDocument14 pagesEsophagus Anatomy, Physiology and DiseasesRyan Chistopher UyNo ratings yet
- SMK 01Document12 pagesSMK 01FathiyaNo ratings yet
- Esophageal DisorderDocument82 pagesEsophageal DisorderMimo HemadNo ratings yet
- Gastroenterology Clinical Focus High Yield Gi and HepatologyDocument426 pagesGastroenterology Clinical Focus High Yield Gi and HepatologyAhana MukherjeeNo ratings yet
- List of Drugs For MimsDocument11 pagesList of Drugs For MimsJoanna Maiden GaciasNo ratings yet
- Tipdil Sentence CompletionDocument51 pagesTipdil Sentence CompletionYasar TepeNo ratings yet
- GIT Dr. Osama Mahmoud PDFDocument78 pagesGIT Dr. Osama Mahmoud PDFRaouf Ra'fat Soliman100% (3)
- GERD Chronic CoughDocument3 pagesGERD Chronic CoughNocK's NicK'sNo ratings yet
- Little Mermaid 1Document12 pagesLittle Mermaid 1Marsh MallowNo ratings yet
- Sas 1-11Document10 pagesSas 1-11boomer SeargeNo ratings yet
- Hiatal Hernia: BY Sojobi Akeem OladimejiDocument16 pagesHiatal Hernia: BY Sojobi Akeem OladimejiMAMA LALANo ratings yet
- NCM 116 Alterations in Nutri and GI Rev5Document100 pagesNCM 116 Alterations in Nutri and GI Rev5JxshxzsNo ratings yet