You might also like
- Psychiatry and The Heart PDFDocument9 pagesPsychiatry and The Heart PDFTaylor AshermanNo ratings yet
- Carter Adjustment DisorderDocument15 pagesCarter Adjustment DisorderTaylor AshermanNo ratings yet
- Pharmacology For Panic Disorder PDFDocument1 pagePharmacology For Panic Disorder PDFTaylor AshermanNo ratings yet
- Schizophrenia and Violence PDFDocument10 pagesSchizophrenia and Violence PDFTaylor AshermanNo ratings yet
- Confusion Assessment Method (CAM) - 1Document2 pagesConfusion Assessment Method (CAM) - 1Iris De La CalzadaNo ratings yet
- Borderline ManagementDocument6 pagesBorderline ManagementTaylor AshermanNo ratings yet
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (894)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Conflict Resolution Lesson Plan PDFDocument2 pagesConflict Resolution Lesson Plan PDFapi-448873912No ratings yet
- Pabasari Ginige: January 20 THDocument28 pagesPabasari Ginige: January 20 THJagath NissankaNo ratings yet
- 4.4 Antibiotics IV To Oral Switch Guidelines For Pharmacists Southern HealthDocument5 pages4.4 Antibiotics IV To Oral Switch Guidelines For Pharmacists Southern HealthditaokkyNo ratings yet
- #2&3 - 18 Street, West Bajac-Bajac, Olongapo City Telefax: (047) 6023200 Mobile: (+63) 920 9020591Document10 pages#2&3 - 18 Street, West Bajac-Bajac, Olongapo City Telefax: (047) 6023200 Mobile: (+63) 920 9020591Leo Arcillas Pacunio100% (1)
- The Drug Interaction Probability ScaleDocument2 pagesThe Drug Interaction Probability ScaleAta07No ratings yet
- Steroid in EntDocument113 pagesSteroid in Entdrazmy2006100% (1)
- Overview of Skin Aging and PhotoagingDocument7 pagesOverview of Skin Aging and PhotoagingtissanNo ratings yet
- Anti-Drug Campaign SpeechDocument2 pagesAnti-Drug Campaign SpeechGracel Gonzaga Eviota91% (11)
- Beyond The Manual: The Insider's Guide To Prolonged Exposure Therapy For PTSDDocument9 pagesBeyond The Manual: The Insider's Guide To Prolonged Exposure Therapy For PTSDmakolla007No ratings yet
- Treatment of Child Victims of Abuse and NeglectDocument18 pagesTreatment of Child Victims of Abuse and NeglectSri Harsha KothapalliNo ratings yet
- Psych Turner SyndromeDocument13 pagesPsych Turner SyndromeJerson CadigalNo ratings yet
- Ifu Somatom DriveDocument600 pagesIfu Somatom DriveImc Muati100% (1)
- Depression: A Global Public Health ConcernDocument3 pagesDepression: A Global Public Health ConcernanalailaNo ratings yet
- Kaac 002Document20 pagesKaac 0027 MNTNo ratings yet
- Sustained Release Dosage FormsDocument9 pagesSustained Release Dosage FormsJasdeep KaurNo ratings yet
- Individual PsychologyDocument5 pagesIndividual PsychologyRessie Joy Catherine FelicesNo ratings yet
- Intestinal DisordersDocument11 pagesIntestinal DisorderspulmonologistNo ratings yet
- Electrical Stimulation: Prepared By: Floriza P. de LeonDocument49 pagesElectrical Stimulation: Prepared By: Floriza P. de LeonFloriza de Leon75% (4)
- Glutathione and Its Antiaging and Antimelanogenic EffectsDocument7 pagesGlutathione and Its Antiaging and Antimelanogenic EffectsG. I.No ratings yet
- Self-motivation quiz tipsDocument1 pageSelf-motivation quiz tipsRose D GuzmanNo ratings yet
- Competences Required For Effective Systemic TherapiesDocument27 pagesCompetences Required For Effective Systemic TherapiesJosé BernalNo ratings yet
- COPD and Pneumonia Case ReportDocument23 pagesCOPD and Pneumonia Case ReportbahrinaNo ratings yet
- Randomized trial therapy worksheetDocument2 pagesRandomized trial therapy worksheetmermerytaNo ratings yet
- On Being Alone: Guide For Widowed PersonsDocument12 pagesOn Being Alone: Guide For Widowed PersonsWinterSpringNo ratings yet
- DPT Doctor of Physiotherapy Program at Abu Zafar InstituteDocument44 pagesDPT Doctor of Physiotherapy Program at Abu Zafar InstituteAbdul basit KaleemNo ratings yet
- Chapter 1 - Psychology As A ScienceDocument21 pagesChapter 1 - Psychology As A Sciencevarunas_250% (2)
- Clinical Manual - Part 2 - Drug Infusion Guidelines Revised - July 2015 - V7.11Document58 pagesClinical Manual - Part 2 - Drug Infusion Guidelines Revised - July 2015 - V7.11Jayaprakash KuppusamyNo ratings yet
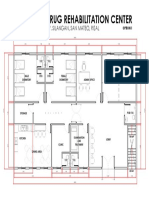
- Proposed Drug Rehabilitation Center: Monterey Sudb., Brgy. Silangan, San Mateo, RizalDocument1 pageProposed Drug Rehabilitation Center: Monterey Sudb., Brgy. Silangan, San Mateo, RizalJonathan MazonNo ratings yet
- Dialog EFN2 Sudarmi 30140114040Document2 pagesDialog EFN2 Sudarmi 30140114040sudarmiNo ratings yet
- SWOT Analysis of The Emergency ServiceDocument20 pagesSWOT Analysis of The Emergency ServiceScribdTranslationsNo ratings yet