You might also like
- GMFM (GMFM-66 & GMFM-88) User's Manual, 2nd editionFrom EverandGMFM (GMFM-66 & GMFM-88) User's Manual, 2nd editionRating: 1 out of 5 stars1/5 (1)
- Appendix: Motor Control Training Intervention ManualDocument32 pagesAppendix: Motor Control Training Intervention Manualgonchodiaz1703No ratings yet
- Measure Joint Range of Motion (ROMDocument5 pagesMeasure Joint Range of Motion (ROMNinoe CueyNo ratings yet
- Diagnostic Value of Five Clinical Tests in Patellofemoral Pain SyndromeDocument9 pagesDiagnostic Value of Five Clinical Tests in Patellofemoral Pain Syndromesridhar100% (1)
- The Relationship of Static Foot Structure To Dynamic Foot FunctionDocument8 pagesThe Relationship of Static Foot Structure To Dynamic Foot FunctionminasNo ratings yet
- Aetiology of Idiopathic Scoliosis. Current Concepts, BurwellDocument34 pagesAetiology of Idiopathic Scoliosis. Current Concepts, BurwellJeanne MalizardNo ratings yet
- Mike ReinoldDocument20 pagesMike ReinoldVikas Kashnia0% (1)
- Strengthening Versus Stabilisation Exercise Programmes for Preventing and Reducing Low Back Pain in FemalesFrom EverandStrengthening Versus Stabilisation Exercise Programmes for Preventing and Reducing Low Back Pain in FemalesNo ratings yet
- Evaluation of The Lumbar Multifidus in Rowers During Espinal Estabilizacion ExercisesDocument7 pagesEvaluation of The Lumbar Multifidus in Rowers During Espinal Estabilizacion ExercisesAline KreiNo ratings yet
- Mulligan Bent Leg Raise Technique - A Preliminary Randomized Trial of Immediate Effects After A Single InterventionDocument6 pagesMulligan Bent Leg Raise Technique - A Preliminary Randomized Trial of Immediate Effects After A Single InterventionBayron EspósitoNo ratings yet
- Manual Therapy: Ottar Vasseljen, Anne Margrethe FladmarkDocument8 pagesManual Therapy: Ottar Vasseljen, Anne Margrethe FladmarkSara AguiarNo ratings yet
- Limiting Factors in Lumbar Spine MotionDocument9 pagesLimiting Factors in Lumbar Spine MotionAni Fran SolarNo ratings yet
- Activacion AbdominalDocument7 pagesActivacion AbdominalArmandoRiosNo ratings yet
- 3 Transversus Abdominis A Different View of The ElepDocument6 pages3 Transversus Abdominis A Different View of The Elepbarros6No ratings yet
- A Kinetic Chain Approach For Shoulder RehabDocument9 pagesA Kinetic Chain Approach For Shoulder RehabRicardo QuezadaNo ratings yet
- Effect of Age On Task Complexity, Exercise and Ambulation: Group 8Document17 pagesEffect of Age On Task Complexity, Exercise and Ambulation: Group 8PreciousShaizNo ratings yet
- How to Use Plug In GaitDocument70 pagesHow to Use Plug In GaitJobin VargheseNo ratings yet
- 2012 Scapular-Focused Treatment in Patients With ShoulderDocument13 pages2012 Scapular-Focused Treatment in Patients With ShoulderIsrael Matías Chandia Ramírez100% (1)
- Piriformis Syndrome (Silvanna)Document9 pagesPiriformis Syndrome (Silvanna)Jonathan QuirogaNo ratings yet
- Chapter 1: Basic Principles of Resistance Training andDocument12 pagesChapter 1: Basic Principles of Resistance Training andLuis Eduardo Barbosa Ortega100% (1)
- (BAL) What Is A Balance BoardDocument2 pages(BAL) What Is A Balance Boardapi-3695814No ratings yet
- Lumbar Spine AssessmentDocument26 pagesLumbar Spine Assessmentyoyo_pt2007100% (1)
- Walking AidsDocument38 pagesWalking AidsMurad KurdiNo ratings yet
- Activation of Deep AbdominalsDocument8 pagesActivation of Deep AbdominalsJosé Guillermo PalominoNo ratings yet
- The Effect of Stance On Muscle Activation in The SquatDocument5 pagesThe Effect of Stance On Muscle Activation in The Squatapi-320703111100% (1)
- The Functional Anatomy of Tensor Fascia Latae and Gluteus Medius and Minimus. Janat00044-0181Document11 pagesThe Functional Anatomy of Tensor Fascia Latae and Gluteus Medius and Minimus. Janat00044-0181Itai IzhakNo ratings yet
- KneeDocument2 pagesKneedrkmsk100% (1)
- Kibler Et Al 2012 Scapula Dyskinesis and Its Relation To Shoulder Injury PDFDocument9 pagesKibler Et Al 2012 Scapula Dyskinesis and Its Relation To Shoulder Injury PDFPamela DíazNo ratings yet
- Muscle Activation in Suspension TrainingDocument22 pagesMuscle Activation in Suspension TrainingRodrigo AlbuquerqueNo ratings yet
- Staged Approach For Rehabilitation ClassificationDocument10 pagesStaged Approach For Rehabilitation ClassificationCambriaChicoNo ratings yet
- Gait in Children With Cerebral PalsyDocument5 pagesGait in Children With Cerebral PalsyvarahamihirNo ratings yet
- Biomechanics of MovementDocument17 pagesBiomechanics of Movements_chandrubioNo ratings yet
- Balance TestDocument21 pagesBalance TestSyazaWajihahZulkefliNo ratings yet
- Joint Mobilizations PDFDocument1 pageJoint Mobilizations PDFErik TellezNo ratings yet
- The Elbow ComplexDocument12 pagesThe Elbow ComplextafelaNo ratings yet
- GAIT 2 - Clinical Gait Analysis - HandoutDocument32 pagesGAIT 2 - Clinical Gait Analysis - Handoutj100% (1)
- Clinical Evaluation of Scapular DysfunctionDocument6 pagesClinical Evaluation of Scapular DysfunctionRudolfGerNo ratings yet
- Neck PainDocument1 pageNeck PainHasan RahmanNo ratings yet
- The Hamstrings Anatomic and Physiologic Variations and Their Potential Relationships With Injury RiskDocument22 pagesThe Hamstrings Anatomic and Physiologic Variations and Their Potential Relationships With Injury RiskHugo TintiNo ratings yet
- Rehabilitation ProtocolDocument9 pagesRehabilitation ProtocolMukesh YadavNo ratings yet
- Blood Flow Restriction Training CAT PDFDocument13 pagesBlood Flow Restriction Training CAT PDFKelly HunterNo ratings yet
- Spinal Injury HockeyDocument65 pagesSpinal Injury HockeyTaniaR.BernalNo ratings yet
- Disability Evaluation: Radhika ChintamaniDocument58 pagesDisability Evaluation: Radhika ChintamaniBhavya Amin0% (1)
- Theme 3. Lumbopelvic Motor Control, Instability and PainDocument9 pagesTheme 3. Lumbopelvic Motor Control, Instability and PainThéo BattalianNo ratings yet
- Isokinetics Report - Leg Strength Test Results and AnalysisDocument1 pageIsokinetics Report - Leg Strength Test Results and Analysis200802588No ratings yet
- Asana Based Exercises Low Back PainDocument14 pagesAsana Based Exercises Low Back PainAutumn Carter100% (1)
- Normal Human LocomotionDocument16 pagesNormal Human LocomotionWendy NgNo ratings yet
- Lecture No. 1 Vertebral Motion DynamicsDocument67 pagesLecture No. 1 Vertebral Motion DynamicsSYED ALI HUSSAIN100% (1)
- Kaltenborn Evjenth Concept of OMTDocument34 pagesKaltenborn Evjenth Concept of OMTJaan100% (1)
- Jurnal Frozen ShoulderDocument21 pagesJurnal Frozen ShoulderMega Mulya Dwi FitriyaniNo ratings yet
- Physical Therapy Management of Congenital Muscular.2Document47 pagesPhysical Therapy Management of Congenital Muscular.2Katherine Valeska Sánchez MuñozNo ratings yet
- CONCEPTS OF MOVEMENtDocument40 pagesCONCEPTS OF MOVEMENtCliff LentoNo ratings yet
- Biomechanics of The Shoulder ComplexDocument83 pagesBiomechanics of The Shoulder ComplexpiciliviNo ratings yet
- (OS 203) Basic Biomechanics of Musculoskeletal System PDFDocument3 pages(OS 203) Basic Biomechanics of Musculoskeletal System PDFSham David PTNo ratings yet
- Cardio Pulmonary AssessmentDocument8 pagesCardio Pulmonary AssessmentSHAIK SHABEENANo ratings yet
- PRI Integration For Geriatrics - Complete FileDocument159 pagesPRI Integration For Geriatrics - Complete Filezhang yangNo ratings yet
- MMT 6-1Document20 pagesMMT 6-1Mughal ZadiiNo ratings yet
- Therapeutic Management of Knee Osteoarthritis: BY PT H N AbdullateefDocument96 pagesTherapeutic Management of Knee Osteoarthritis: BY PT H N AbdullateefMaida FitrianiNo ratings yet
- Quality Policy and Quality ObjectivesDocument2 pagesQuality Policy and Quality ObjectivesrabiulfNo ratings yet
- Impulse Valve Operator Kit IV.1.09.01Document2 pagesImpulse Valve Operator Kit IV.1.09.01eduardo gonzalezav0% (1)
- CV - Alok Singh - Tech HSE & Loss Prevention Engineer (May-2018)Document5 pagesCV - Alok Singh - Tech HSE & Loss Prevention Engineer (May-2018)toalok4723No ratings yet
- High Efficiency Battery Charger Using DC-DC ConverterDocument4 pagesHigh Efficiency Battery Charger Using DC-DC ConvertersanilNo ratings yet
- Introduction to Concrete Components and ClassificationDocument29 pagesIntroduction to Concrete Components and ClassificationUsama AliNo ratings yet
- DC Components Co., LTD.: Rectifier SpecialistsDocument3 pagesDC Components Co., LTD.: Rectifier SpecialistsPICVIONo ratings yet
- 3 Instant Ways To Make Money From People Around You: by Oluwatoyin OmotosoDocument21 pages3 Instant Ways To Make Money From People Around You: by Oluwatoyin Omotosoobisesan phillipNo ratings yet
- Amcor 2016Document69 pagesAmcor 2016Romulo AlvesNo ratings yet
- 2013 Midterm 3Document16 pages2013 Midterm 3billbyoag123No ratings yet
- CZ-RTC4 - Service ManualDocument68 pagesCZ-RTC4 - Service ManualAnonymous 31Airw50% (2)
- Wind Energy - University QuesDocument2 pagesWind Energy - University QuesKsn Hari100% (2)
- JCM Hybrid Controller User ManualDocument13 pagesJCM Hybrid Controller User ManualMtvc LbNo ratings yet
- Ground Improvement TechniquesDocument29 pagesGround Improvement TechniquesMeEr AahilNo ratings yet
- TDFC Global Engineering Solutions CompanyDocument189 pagesTDFC Global Engineering Solutions CompanyplanningNo ratings yet
- Introduction To Pressure TransducersDocument2 pagesIntroduction To Pressure TransducersTEUKUNo ratings yet
- ST Series Servo Motor: Beijing KND CNC Technique Co.,Ltd. 01.2012Document21 pagesST Series Servo Motor: Beijing KND CNC Technique Co.,Ltd. 01.2012Dinos ArhNo ratings yet
- Valve RecessionDocument26 pagesValve RecessionHamid HasanNo ratings yet
- 2013 Renault ZOE PresskitDocument34 pages2013 Renault ZOE PresskitDidelisNo ratings yet
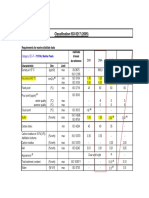
- Classification ISO 8217 (2005)Document5 pagesClassification ISO 8217 (2005)Salah JallaliNo ratings yet
- MeasurementDocument4 pagesMeasurementJemason100% (1)
- Euler-Ship Mast LocationDocument61 pagesEuler-Ship Mast LocationzeldaikNo ratings yet
- More power in less space with SMA SUNNY CENTRAL UPDocument4 pagesMore power in less space with SMA SUNNY CENTRAL UPBrahadeesh Perinkolam MuraliNo ratings yet
- APFC Epcos 6Document8 pagesAPFC Epcos 6Sriman ChinnaduraiNo ratings yet
- Water Level IndicatorDocument5 pagesWater Level IndicatorRahul JadhavNo ratings yet
- Sungris BrochureDocument8 pagesSungris Brochurechemasi123No ratings yet
- Boundary Layer ThicknessDocument23 pagesBoundary Layer ThicknessPridhar ThiagarajanNo ratings yet
- Samsung 2800mah ICR18650-28ADocument17 pagesSamsung 2800mah ICR18650-28AStreet_skNo ratings yet
- 24th Annual International Pittsburgh Coal 2007 WixDocument10 pages24th Annual International Pittsburgh Coal 2007 WixAmauche OgeNo ratings yet
- Sany HBT8018C-5S (T3) Trailer Pump - 004118Document2 pagesSany HBT8018C-5S (T3) Trailer Pump - 004118اهى عيشه وبن عشها just a lifeNo ratings yet
- DPDC MaintenanceDocument5 pagesDPDC MaintenanceArfana Akter BanogirNo ratings yet