Professional Documents
Culture Documents
Transition Theory Overview
Uploaded by
Hazel RoseOriginal Description:
Original Title
Copyright
Available Formats
Share this document
Did you find this document useful?
Is this content inappropriate?
Report this DocumentCopyright:
Available Formats
Transition Theory Overview
Uploaded by
Hazel RoseCopyright:
Available Formats
20
PR SA O M PE PL R E TY C O O F N E TE L N SE T V - N IE O R T FI N
Transition Theory
Eun-Ok Im
Alligood 978-0-323-05641-0/0029
C H A PT E R
Afaf Ibrahim Meleis
AL
I believe very strongly that, while knowledge is universal, the agents for developing knowledge must reflect the nature of the questions that are framed and driven by the different disciplines about the health and well-being of individuals or populations (Meleis, 2007, ix).
CREDENTIALS AND BACKGROUND OF THE THEORIST
Afaf Ibrahim Meleis was born in Alexandria, Egypt. In personal communications with Meleis (December 29, 2007), she reckons that nursing has been part of her life since she was born. Her mother is considered the Florence Nightingale of the Middle East; she was the rst person in Egypt to obtain a BSN degree from Syracuse University, and the rst nurse in Egypt who obtained an MPH and a PhD from an Egyptian university. Meleis considered nursing to be in her blood, and she admired her mothers dedication and commitment to the profession. Under the inuence of her mother, Meleis became interested in nursing and loved the potential of developing the discipline. Yet, when she chose to pursue nursing, her parents 416
objected to her choice because they knew how much nurses struggle in having a voice and affecting quality of care. However, they eventually approved of her choice and had faith that Meleis could do it. Meleis completed her nursing degree at the University of Alexandria, Egypt. She came to the United States to pursue graduate education as a Rockefeller Fellow in order to become an academic nurse (Meleis, personal communication, December 29, 2007). From the University of California, Los Angeles, she received an MS in nursing in 1964, an MA in sociology in 1966, and a PhD in medical and social psychology in 1968. Her career combined academic and administrative positions. After getting her doctoral degree, she worked as an acting instructor at the University of California, Los Angeles, from 1966 to 1968, and as an
Chapter 20
Afaf Ibrahim Meleis
417
Assistant Professor at the same university from 1968 to 1971. In 1971, she moved to the University of California, San Francisco (UCSF), where she spent the next 34 years, and where her Transition Theory was rst developed. In 2002, she was nominated the Margret Bond Simon Dean of Nursing, and became the Dean of the School of Nursing at the University of Pennsylvania. Meleis, a prominent nurse sociologist, is a soughtafter theorist, researcher, and speaker on the topics of womens health and development, immigrant healthcare, international healthcare, and knowledge and theoretical development. She is currently on the Counsel General of the International Council on Womens Health Issues. Meleis received numerous honors and awards as well as honorary doctorates and distinguished and honorary professorships around the world. She received the Medal of Excellence for professional and scholarly achievements from Egyptian President Hosni Mubarak in 1990. In 2000, she received the Chancellors Medal from the University of Massachusetts, Amherst. In 2001, she received the UCSFs Chancellor Award for the Advancement of Women in recognition of her role as a worldwide activist on behalf of womens issues. In 2004, she received the Pennsylvania Commission for Women Award in celebration of womens history month and the Special Recognition Award in Human Services from the Arab American Family Support Center in New York. In 2006, she was awarded the Robert E. Davies Award from the Penn Professional Womens Network for her advocacy on behalf of women. Meleis research focuses on global health, immigrant and international health, womens health, and the theoretical development of the nursing discipline. She authored more than 150 articles in social sciences, nursing, and medical journals; 40 chapters; and numerous monographs, proceedings, and books. Her award winning book, Theoretical Nursing: Development and Progress (1985, 1991, 1997, 2007), is used widely throughout the world. The development of Transition Theory began in the mid-1960s, when Meleis was working on her PhD, and can be traced through the years of her
research with students and colleagues. In her book (Meleis, 2007), describes how her theoretical journey started from her practice and research interests. In her masters and PhD dissertation research, Meleis investigated phenomena of planning pregnancies and processes involved in becoming a new parent and mastering parenting roles. She focused on spousal communication and interaction in effective or ineffective planning of the number of children in families (Meleis, 1975), and later reasoned that her earlier ideas were incomplete since she did not consider transitions. Subsequently, her research interests were focused on people who do not make healthy transitions and discovery of interventions that would facilitate healthy transitions. For these research questions, symbolic interactionism played an important role in efforts to conceptualize the symbolic world that shapes interactions and responses. This shift in her theoretical thinking led her to role theories as were referenced in her publications in those years of the 1970s and 1980s. Meleis earliest work with transitions dened unhealthy transitions or ineffective transitions in relation to role insufciency. She dened role insufciency as any difculty in the cognizance and/or performance of a role or of the sentiments and goals associated with the role behavior as perceived by the self or by signicant others (Meleis, 2007). This conceptualization led Meleis to dene the goal of healthy transitions as mastery of behaviors, sentiments, cues, and symbols associated with new roles and identities and non-problematic processes. Meleis believed that knowledge development in nursing should be geared toward nursing therapeutics and not toward understanding the phenomena related to responses to health and illness situations. Consequently, she initiated the development of role supplementation as a nursing therapeutic as seen in her earlier research (Meleis, 1975; Meleis & Swendsen, 1978; Jones, Zhang, & Meleis, 1978). The gist of Meleis works published in the 1970s dened role supplementation as any deliberate process through which role insufciency or potential role insufciency can be identied by the role
PR SA O M PE PL R E TY C O O F N E TE L N SE T V - N IE O R T FI N
Alligood 978-0-323-05641-0/0029
AL
418
UNIT
IV
Nursing Theories
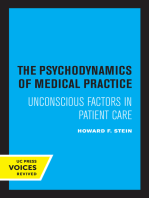
framework was well received by nurse scholars and researchers and began to be used as a conceptual framework in a number of studies that examined the following: Description of immigrant transitions (Meleis, Lipson, & Dallafar, 1998) Womens experience of rheumatoid arthritis (Shaul, 1997) Recovery from cardiac surgery (Shih, et al., 1998) Family caregiving role for patients in chemotherapy (Schumacher, 1995) Early memory loss for patients in Sweden (Robinson, Ekman, Meleis, Wahlund, & Winbald, 1997) Aging transitions (Schumacher, Jones, & Meleis, 1999) African American womens transition to motherhood (Sawyer, 1997) Using the transition framework, a middle range theory for transition was developed by the researchers who had used transition as a conceptual framework. They analyzed their ndings related to transition experiences and responses, identifying similarities and differences in the use of transition; ndings were compared, contrasted, and integrated through extensive reading, reviewing, and dialoguing, and in group meetings. The collective work was published in 2000 (Meleis, Sawyer, Im, Schumacher, & Messias, 2000) and has been widely used in nursing studies. See Figure 20-1 for a diagram of the middle range transition theory. The situation-specic theories based on the transition framework that Meleis (1997) called for, with specics in level of abstraction, degree of specicity, scope of context, and connection to nursing research and practice, were similar to the emerging midrange transition theory by Meleis et al. (Im, 2006; Im & Meleis, 1999a; Im & Meleis, 1999b; Schumacher, Jones, & Meleis, 1999). For example, Im and Meleis (1999b) developed a situation-specic theory of lowincome Korean immigrant womens menopausal transition based on their research ndings, while using the transition framework of Schumacher and Meleis (1994). Schumacher et al. (1999) developed
incumbent and signicant others. Thus, role supplementation includes both role clarication and role taking, which may be preventive and therapeutic. With these changes in her theoretical thinking, role supplementation as a nursing therapeutic entered her research projects. Her main research questions were to further dene the components, the processes, and the strategies related to role supplementation, which she believed would make a difference by helping patients complete a healthy transition. This led Meleis to dene health as mastery, and she tested that denition through proxy outcome variables such as fewer symptoms, perceived well-being, and ability to assume new roles. Her theory of role supplementation was used not only in her studies on the new role of parenting (Meleis & Swendsen, 1978), but in other studies among postmyocardial infarction patients (Dracup, Meleis, Baker, & Edlefsen, 1985), elders (Kaas & Rousseau, 1983), parental caregivers (Brackley, 1992), caregivers of Alzheimers patients (Kelley & Lakin, 1988), and women who were not successful in becoming mothers and who maintained role insufciency (Gaffney, 1992). In these studies using role supplementation theory, Meleis began to question the nature of transitions and the human experience of transitions. Her research population interests shifted to immigrants and their health. This shift led Meleis to look back and question transitions as a concept. Meleis met Norma Chick from Massey University, New Zealand, and they developed transition as a concept that was published in 1985 (Chick & Meleis, 1986). This was actually Meleis rst article on transitions as a major concept of nursing. To further develop this theoretical work, Meleis initiated extensive literature searches with Karen Schumacher, a doctoral student at the University of California, San Francisco, to discover how extensively transition was used as a concept or framework in nursing literature. Three hundred ten articles focused on transitions, so Meleis further developed the transition framework (Schumacher & Meleis, 1994) that was later further developed as a middle range theory. Publication of the transition
PR SA O M PE PL R E TY C O O F N E TE L N SE T V - N IE O R T FI N
Alligood 978-0-323-05641-0/0029
AL
Chapter 20
Afaf Ibrahim Meleis
419
Nature of Transition Types Developmental Situational Health/Illness Organizational
Transition Conditions: Facilitators and Inhibitors Personal Meanings Cultural beliefs & attitudes Socioeconomic status Preparation & knowledge
Patterns of Response Process Indicators Feeling connected Interactions Locating and being situated Developing confidence and coping
PR SA O M PE PL R E TY C O O F N E TE L N SE T V - N IE O R T FI N
Properties Awareness Engagement Change and difference Transition time span Critical points and events Nursing Therapeutics
Patterns Single Multiple Sequential Simultaneous Related Unrelated
Community
Society
Outcome Indicators Mastery Fluid Integrative Identities
F igure 20-1 The Midrange Transition Theory. (From Meleis, A. I., Sawyer, L. M., Im, E. O., Messias, D.
K. H., & Schumacher, K. [2000]. Experiencing transitions: An emerging middle range theory. Advances in Nursing Science, 23[1], 12-28.)
a situation-specic theory of elderly transition. Im (2006) also developed a situation-specic theory of white cancer patients pain experience. These situation-specic theories were derivative of the middle range transition theory.
THEORETICAL SOURCES
Theoretical sources for Transition Theory are multiple. First, Meleis background in nursing, sociology, symbolic interactionism, and role theory and her education led to the development of Transition Theory as described above. Indeed, ndings and experience from research projects, educational programs, and clinical practice in hospital and community settings have been frequent sources for theoretical
development in nursing (Im, 2005). A systematic, extensive literature review was another source for development of Transition Theory. A systematic, extensive literature review has been suggested as a way of compiling currently existing knowledge about a nursing phenomenon and has been used frequently as an excellent source for theory development (Walker & Avant, 1995, 2005). Finally, collaborative efforts among researchers who used the transition theoretical framework and the middle range transition theory in their studies were another source for development of Transition Theory. As Im (2005) asserted, experts in different areas of nursing who are working on the same nursing phenomenon could give different and new views/visions of the same nursing phenomenon.
Alligood
978-0-323-05641-0/0029
AL
420
UNIT
IV
Nursing Theories
MAJOR CONCEPTS & DEFINITIONS
Here, the major concepts and denitions from the most current transition theory, the middle range theory of transition suggested by Meleis et al. (2000), are presented. Some concepts that were briey presented in the middle range theory of transition are dened in greater detail based on the transition framework by Schumacher and Meleis (1994). Major concepts of the middle range theory of transition include the following: (a) types and patterns of transitions; (b) properties of transition experiences; (c) transition conditions (facilitators and inhibitors); (d) process indicators; (e) outcome indicators; and (f) nursing therapeutics. TYPES AND PATTERNS OF TRANSITIONS of overlap among transitions, and the nature of the relationship between the different events that are triggering transitions for a client. PROPERTIES OF TRANSITION EXPERIENCE
Types of transitions include developmental, health and illness, situational, and organizational. Developmental transition includes birth, adolescence, menopause, aging (or senescence), and death. Health and illness transitions include recovery process, hospital discharge, and diagnosis of chronic illness (Meleis & Trangenstein, 1994). Organizational transitions refer to changing environmental conditions that affect the lives of clients, as well as workers within them (Schumacher & Meleis, 1994). Patterns of transitions include multiplicity and complexity (Meleis et al., 2000). Many people are experiencing multiple transitions at the same time rather than experiencing a single transition, which cannot be easily distinguished from the contexts of their daily lives. Indeed, in the article by Meleis et al. (2000), it was noted that each of the studies that were the basis for the theoretical development involved individuals who were experiencing at least two types of transitions at the same time, which could not be discrete or mutually exclusive. Thus, they suggested that important considerations are whether multiple transitions are sequential or simultaneous, the extent
Properties of the transition experience include (a) awareness; (b) engagement; (c) change and difference; (d) time span; and (e) critical points and events. Meleis et al. (2000) asserted that these properties are not necessarily discrete, but are interrelated as a complex process. Awareness is dened as perception, knowledge, and recognition of a transition experience, and level of awareness is often reected in the degree of congruency between what is known about processes and responses and what constitutes an expected set of responses and perceptions of individuals undergoing similar transitions (Meleis et al., 2000). While asserting that a person in transition may have some awareness of the changes that are occurring, Chick and Meleis (1986) posited that an absence of awareness of change could signify that an individual may not have initiated the transition experience; Meleis et al. (2000) later proposed that the lack of manifestation of awareness of changes does not by necessity preclude the onset of a transition experience. However, the tension between transition awareness by clients and nurses knowledge of whether clients are in transition has not been resolved yet (Meleis et al., 2000). Engagement is another property of transition suggested by Meleis et al. (2000). Engagement refers to the degree to which a person demonstrates involvement in the process inherent in the transition. The level of awareness is considered to inuence the level of engagement in that engagement may not happen without awareness. Meleis et al. (2000) suggested that the level of engagement of a person who is aware of physical, emotional,
PR SA O M PE PL R E TY C O O F N E TE L N SE T V - N IE O R T FI N
Alligood 978-0-323-05641-0/0029
AL
Chapter 20
Afaf Ibrahim Meleis
421
MAJOR CONCEPTS & DEFINITIONScontd
social, or environmental changes would differ from that of a person unaware of these changes. Changes and differences are a property of transitions (Meleis et al., 2000). Changes in identities, roles, relationships, abilities, and patterns of behavior are supposed to bring a sense of movement or direction to internal processes, as well as external processes (Schumacher & Meleis, 1994). Meleis et al. (2000) asserted that all transitions involve change, whereas not all change is related to transition. Then, they suggested that to fully understand a transition process, it is necessary to uncover and describe the effects and meanings of the changes involved and the dimensions of changes (e.g., nature, temporality, perceived importance or severity, personal, familial, and societal norms and expectations). Differences are also suggested as a property of transitions. Meleis et al. (2002) believed that confronting differences could be exemplied by unmet or divergent expectations, feeling different, being perceived as different, or seeing the world and others in different ways, and suggested that it might be useful for nurses to consider a clients level of comfort and mastery in dealing with changes and differences. Time span is also a property of transitionsall transitions may be characterized as owing and moving over time (Meleis et al., 2000). According to the assertion by Bridges (1980, 1991), in the middle range theory of transition, transition is dened as a span of time with an identiable starting point, extending from the rst signs of anticipation, perception, or demonstration of change; moving through a period of instability, confusion, and distress; to an eventual ending with a new beginning or period of stability. However, Meleis et al. (2000) also made the point that it might be difcult or impossible, and perhaps even counterproductive, to put boundaries on the time span of certain transition experiences. Critical points and events are the nal property of transitions suggested by Meleis et al. (2000). Critical points and events are dened as markers such as birth, death, the cessation of menstruation, or the diagnosis of an illness. Meleis et al. (2000) also acknowledge that specic marker events might not be evident for some transitions, although transitions usually have critical points and events. Critical points and events are usually associated with increasing awareness of changes or differences or more active engagement in dealing with transition experiences. Also, Transition Theory conceptualizes that there are nal critical points that are characterized by a sense of stabilization in new routines, skills, lifestyles, and selfcare activities, and that a period of uncertainty is marked by uctuation, continuous change, and disruption of reality. TRANSITION CONDITIONS
PR SA O M PE PL R E TY C O O F N E TE L N SE T V - N IE O R T FI N
Alligood 978-0-323-05641-0/0029
Transition conditions are those circumstances that inuence the way a person moves through a transition, and that facilitate or hinder progress toward achieving a healthy transition (Schumacher & Meleis, 1994). Transition conditions include personal, community, or societal factors that may facilitate or constrain the processes and outcomes of healthy transitions. Personal conditions include meanings, cultural beliefs and attitudes, socioeconomic status, preparation, and knowledge. Meleis et al. (2000) considered that the meanings attributed to events precipitating a transition and to the transition process itself may facilitate or hinder healthy transitions. Cultural beliefs and attitudes such as stigma attached to a transition experience (e.g., Chinese stigmatization of cancer) would inuence the transition experience. Socioeconomic status could inuence peoples transition experiences. Anticipatory preparation or lack of preparation
Continued
AL
422
UNIT
IV
Nursing Theories
MAJOR CONCEPTS & DEFINITIONScontd
could facilitate or inhibit peoples transition experiences. Community conditions (e.g., community resources) or societal conditions (e.g., marginalization of immigrants in the host country) could be facilitators or inhibitors for transitions. Compared with personal transition conditions, the subconcepts of community conditions and societal conditions tend to be underdeveloped. PATTERNS OF RESPONSE OR PROCESS AND OUTCOME INDICATORS whether the person is turned in the direction of a healthy transition. The extent to which there is a pattern indicating that the people involved are experiencing an increase in their levels of condence is another important process indicator of a healthy transition. The outcome indicators suggested by Meleis et al. (2000) include mastery and uid integrative identities. A healthy completion of a transition can be determined by the extent to which people demonstrate mastery of the skills and behaviors needed to manage their new situations or environments. Identity reformulation can also represent a healthy completion of a transition. NURSING THERAPEUTICS
PR SA O M PE PL R E TY C O O F N E TE L N SE T V - N IE O R T FI N
Indicators of healthy transitions in the framework by Schumacher and Meleis (1994) were replaced by patterns of response in the middle range theory of transitions. Patterns of response are conceptualized as process indicators and outcome indicators. These process indicators and outcome indicators characterize healthy responses. Process indicators that move clients in the direction of healthy or toward vulnerability and risk allow early assessment and intervention by nurses to facilitate healthy outcomes. Also, outcome indicators may be used to check if a transition is a healthy one or not, but Meleis et al. (2000) warned that outcome indicators may be related to other events in peoples lives if they are examined too soon in a transition process. The process indicators suggested by Meleis et al. (2000) include feeling connected, interacting, being situated, and developing condence and coping. The need to feel and stay connected is a process indicator of a healthy transition; if immigrants make new contacts and continue old connections with extended family and friends, they are usually in a healthy transition. Through interaction, the meaning of the transition and the behaviors developed in response to the transition can be uncovered, claried, and acknowledged, which usually leads to a healthy transition. Location and being situated in terms of time, space, and relationships are usually important in most transitions; these indicate
Alligood 978-0-323-05641-0/0029
Schumacher and Meleis (1994) conceptualized nursing therapeutics as three measures that are widely applicable to therapeutic intervention during transitions. First, they proposed assessment of readiness as a nursing therapeutic. Assessment of readiness needs to be a multidisciplinary endeavor and requires a comprehensive understanding of the client; it requires assessment of each of the transition conditions in order to create an individual prole of client readiness, and to enable clinicians and researchers to identify various patterns of the transition experience. Second, the preparation for transition is suggested as a nursing therapeutic. The preparation of transition includes education as the primary modality for creating optimal conditions in preparation for transition. Third, role supplementation was proposed as a nursing therapeutic. Role supplementation was introduced theoretically and empirically by Meleis (1975) and was used by many researchers (Brackley, 1992; Dracup, Clark, Meleis Clyburn, Shields, & Stanley 1985; Gaffney, 1992; Meleis & Swendsen, 1978). Yet, in the middle range theory of transitions, no further development of the concept of nursing therapeutics was made.
AL
Chapter 20
Afaf Ibrahim Meleis
423
USE OF EMPIRICAL EVIDENCE
In the development of the transition framework by Schumacher and Meleis (1994), a systematic extensive literature review of more than 300 articles related to transitions provided empirical evidence of the conceptualization and theorizing. Then, as mentioned above, the transition framework was tested in a number of studies to describe immigrants transitions (Meleis et al., 1998), womens experiences with rheumatoid arthritis (Shaul, 1997), recovery from cardiac surgery (Shih et al., 1998), development of the family caregiving role for patients in chemotherapy (Schumacher, 1995), Korean immigrant low income women in menopausal transition (Im, 1997; Im & Meleis, 2000, 2001; Im, Meleis, & Lee, 1999), early memory loss for patients in Sweden (Robinson, Ekman, Meleis, Wahlund, & Winbald, 1997), the aging transition (Schumacher, Jones, & Meleis, 1999), African American womens transition to motherhood (Sawyer, 1997), and adult medical-surgical patients perceptions of their readiness for hospital discharge (Weiss et al., 2007). In the process of developing the middle range theory of transition, ve research studies provided empirical evidence for conceptualization and theorizing (Sawyer, 1997; Im, 1997; Messias, Gilliss, Sparacino, Tong, & Foote, 1995; Messias, 1997; Schumacher, 1994). These studies were conducted among culturally diverse groups of people in transition, including African American mothers, Korean immigrant midlife women, parents of children diagnosed with congenital heart defects, Brazilian women immigrating to the United States, and family caregivers of persons receiving chemotherapy for cancer. Empirical ndings of these ve studies provided the theoretical basis for the concepts of the middle range theory of transition, and the concepts and their relationships were developed and formulated based on a collaborative process of dialogue, constant comparison of ndings across the ve studies, and analysis of ndings. For example, one of the personal conditions, meanings, was proposed based on the ndings from two studies (Im, 1997; Sawyer, 1997). According to Meleis et al. (2000), in Ims study, although Korean immigrant midlife women
PR SA O M PE PL R E TY C O O F N E TE L N SE T V - N IE O R T FI N
MAJOR ASSUMPTIONS
Alligood 978-0-323-05641-0/0029
had ambivalent feelings toward menopause, menopause itself did not have special meaning attached to it. Im found that most of the participants did not connect any special problems they were having to their menopausal transitions. Rather, women went through their menopause without experiencing or perceiving any problems, which means that no special meaning might have facilitated the womens menopausal transition. Yet, Sawyers study reported that African American women related intense enjoyment of their roles as mothers and described motherhood in terms of being responsible, protecting, supporting, and needed. Thus, Meleis et al. (2000) proposed meanings as a personal transition condition because, in both studies, neutral and positive meanings might have facilitated menopause and motherhood. The middle range theory of transition was used recently in several studies to develop situationspecic theories (Im, 2006; Im & Meleis, 1999b; Schumacher et al., 1999) and to test the theory in a study on relatives experience of the move to a nursing home (Davies, 2005). In turn, these studies also provide empirical evidence for the middle range theory of transition.
Based on Meleis former works on role supplementation, the transition framework by Schumacher and Meleis (1994), and the middle range theory of transitions by Meleis et al. (2000), the following assumptions of Transition Theory could be inferred. Transitions are complex and multidimensional. Transitions have patterns of multiplicity and complexity. All transitions are characterized by ow and movement over time. Transition cause changes in identities, roles, relationships, abilities, and patterns of behavior. Transitions involve a process of movement and changes in fundamental life patterns, which are manifested in all individuals. Change and difference are not interchangeable, nor are they synonymous with transition. Transitions both result in change and are the result of change.
AL
424
UNIT
IV
Nursing Theories
LOGICAL FORM
Transition theory has been formulated and theorized through induction by the use of existing research (a systematic literature review and research ndings). As mentioned earlier, it was initially developed as a central concept of nursing and was further developed as a middle range theory. Transition theory was formulated with the goal of integrating what is known about transition experience across different types of transitions to provide directions for nursing therapeutics for people in transition. This theory provides a framework for seeing how the results of previous research related to various types of transitions t together more clearly, and how concepts can be manipulated for further study.
PR SA O M PE PL R E TY C O O F N E TE L N SE T V - N IE O R T FI N
THEORETICAL ASSERTIONS
Theoretical assertions in transition theory were inferred in the early works of Meleis. This includes her work on role supplementation, the transition framework by Schumacher and Meleis (1994), and the middle range theory of transitions by Meleis et al. (2000). Following are the theoretical assertions made in the theoretical works: Developmental, health and illness, and organizational transitions are central to nursing practice. Patterns of transition include (a) whether the client is experiencing a single transition or multiple transitions; (b) whether multiple transitions are sequential or simultaneous; (c) the extent of overlap among transitions; and (d) the nature of the relationship between the different events that are triggering transitions for a client. Properties of transition experience are interrelated parts of a complex process. The level of awareness inuences the level of engagement, in that engagement may not happen without awareness. Humans perceptions of and meanings attached to health and illness situations are inuenced by and in turn inuence the conditions under which a transition occurs. Healthy transition is characterized by both process and outcome indicators. Negotiating successful transitions depends on the development of an effective relationship between the nurse and the client (nursing therapeutic). This relationship is a highly reciprocal process that affects both the client and the nurse.
ACCEPTANCE BY THE NURSING COMMUNITY
Over the past several decades, transitions have emerged as a central concept of nursing phenomenon, and Transition Theory has been widely used throughout the world. Transition Theory was translated and used extensively in Sweden, Taiwan, and many other places.
Practice
Transition Theory can provide a comprehensive perspective on transition experience while considering the contexts within which people are experiencing a transition. Because of its comprehensiveness, applicability, and afnity with health, Transition Theory has been applied to many human phenomena of interest and concern to nurses, such as illness, recovery, birth, death, and loss, as well as immigration. Transition Theory is useful in explaining health/illness transitions such as the recovery process, hospital discharge, and diagnosis of chronic disease (Meleis & Trangenstein, 1994). Indeed, studies have indicated that Transition Theory could be applied to nursing practice with diverse groups of people, including geriatric populations, psychiatric populations, maternal populations, family caregivers, menopausal
Alligood
978-0-323-05641-0/0029
AL
The daily lives of clients, environments, and interactions are shaped by the nature, conditions, meanings, and processes of their transition experiences. Vulnerability is related to transition experiences, interactions, and environmental conditions that expose individuals to potential damage, problematic or extended recovery, or delayed or unhealthy coping. Nurses are the primary caregivers of clients and their families who are undergoing transitions.
Chapter 20
Afaf Ibrahim Meleis
425
PR SA O M PE PL R E TY C O O F N E TE L N SE T V - N IE O R T FI N
Education
Transition Theory is used widely in graduate education and undergraduate education throughout the world (Meleis, personal communication, December 29, 2007). There is a growing international interest in integrating Transition Theory into nursing curricula across countries (Meleis, personal communication, January 2008). Transition Theory was used as a curriculum framework in a number of places, including the University of Connecticut (Meleis, personal communication, December 29, 2007). At the UCSF, an independent graduate elective course on transitions and health was taught by Meleis in order to respond to an increasing learning need of graduate students. At the University of Pennsylvania, a center called Transitions and Health was established in 2007 with a $5 million dollar endowment (Director: Mary Taylor)this is the rst center on transitions and health endowed anywhere.
women, Alzheimer patients, immigrant women, and people with chronic illness, among others (Aroian & Prater, 1988; Brackley, 1992; Im, 1997; Kaas & Rousseau, 1983; Schumacher, Dodd, & Paul, 1993; Shaul, 1997). Transition Theory could provide direction for nursing practice with people in various types of transitions by providing a comprehensive perspective on the nature and type of transitions, transition conditions, and process and outcome indicators of patterns of response to transitions. Also, Transition Theory will lead to the development of nursing therapeutics that is congruent with the unique experience of clients and their families in transition, thus promoting healthy responses to transition.
often used as a parent theory for situation-specic theories (Im & Meleis, 1999a; Im, 2006; Schumacher et al., 1999).
FURTHER DEVELOPMENT
As mentioned in the article on the middle range theory of transitions (Meleis, 2000), Transition Theory was an emerging framework that could be further developed, tested, and rened, reecting Meleis philosophical position on theory development as cyclic, dynamic, and evolving. Transition theory continues to be rened and tested to explain the major concepts and relationships among the major concepts with diverse groups of populations in various types of transition, which will increase its power to describe nursing phenomena. Also, because sufcient empirical support by a number of studies using Transition Theory as a theoretical basis currently exists, future studies need to aim at design and conduct of intervention studies to test Transition Theorybased interventions, through which Transition Theory will gain power to direct nursing practice. Also, as Meleis (2007) envisioned, a number of situation-specic theories could be developed based on Transition Theory.
CRITIQUE
Clarity and Simplicity
Research
A number of researchers have used Transition Theory in their studies as a theoretical basis for research. Meleis research program is naturally based on Transition Theory, and other researchers have tested the empirical precision of Transition Theory through their studies (Davies, 2005; Weiss et al., 2007). As mentioned earlier, Transition Theory was
Transition Theory is simple and clear to understand. The conceptual denitions are clear and provide a comprehensive understanding of the complexity of transitions. The major concepts are logically linked, and the relationships are obvious in their theoretical assertions. The relationships among the major concepts are clearly depicted in a visually simple diagram (see Figure 3). The variables are independent of each other, yet the interactive effects among the variables are clearly depicted by arrows.
Generality
Transition Theory is a middle range theory in scope. Middle range theories have more limited scope and less abstraction than grand theories, and they
Alligood
978-0-323-05641-0/0029
AL
426
UNIT
IV
Nursing Theories
SUMMARY
Current healthcare systems are frequently characterized by changes, diversities, and complexities. Transition Theory that evolved from research studies among diverse groups of people in various types of transitions could adequately direct nursing practice, education, and practice in the current healthcare system. Meleis made her theoretical journey from the 1960s to now; her journey will continue, and others will follow in her footsteps. Transition Theory will continue to develop through a number of studies that are using the theory, and Meleis visionary leadership throughout the world will continue to inuence nursing practice, education, and research.
PR SA O M PE PL R E TY C O O F N E TE L N SE T V - N IE O R T FI N
Empirical Precision
Transition Theory has been tested and supported by Meleis and others as a framework for explaining the transition experiences of diverse groups of populations in different types of transitions. Transition Theory continues to evolve through planned programs of research, and continued empirical research studies will further refine the theory. With the development of situation-specific theories derived from Transition Theory, its distance from the empirical world will be further reduced as well.
address specic phenomena or concepts, which make them more easily applicable to nursing practice. Yet, because of its limited scope, Transition Theory tends to be generalizable to people in transitions. When the diverse types of transitions are considered, Transition Theory is relevant for any population in transition, depending on what type of transition the population is experiencing. The research used to derive Transition Theory was actually based on the participation of different gender and ethnic groups, in a variety of settings, which makes Transition Theory more easily applicable and generalizable, compared with other theories that were developed based on research among a specic group of people.
C ase S tudy
Derivable Consequences
Transition Theory with a focus on people in diverse types of transitions provides a comprehensive and evolving guide for all health-related disciplines. Health-related disciplines always deal with a type of transition, whether single or multiple. Especially with an increasing need for culturally competent health care for diverse groups of healthcare clients, Transition Theory could provide a more appropriate theoretical t for current health care, because of its inherent consideration of diversities of healthcare clients and its basis in research among diverse groups of people in transition.
Sue Kim, age 49, immigrated from South Korea to the United States 6 years ago. Her family came to the United States to educate their children, and moved in with family members in Los Angeles. Sue and her husband graduated from a top ranked university in South Korea, and her husband also had a masters degree in business. However, their English skills were not adequate for them to get jobs in the United States. Instead, they opened a Korean grocery store with the money that they brought from South Korea, and they managed to settle down in Los Angeles, where a number of Koreans are living. They have two children: Mina, a 25-year-old daughter who is now the manager of a local shop, and Yujun, a 21-year-old son who is a college student. Both children were born in South Korea and moved to the United States with Sue. The children had a hard time, especially Mina, who came to the United States in her senior year of high school. However, the children nally adapted to their new environment. Now, Mina is living alone in a onebedroom apartment near downtown LA, and Yujun is living in a university dormitory. The Kims are a religious family and attend their communitys
Alligood
978-0-323-05641-0/0029
AL
Chapter 20
Afaf Ibrahim Meleis
427
Protestant church regularly. They are involved in many church activities. Sue and her husband have been too busy to have regular annual checkups for the past 6 years. About 1 year ago, Sue began to have serious indigestion, nausea, vomiting, and upper abdominal pain; she took some over-the-counter medicine and tried to tolerate the pain. Last month, her symptoms became more serious; she visited a local clinic and was referred to a larger hospital. Recently, she was diagnosed with stomach cancer after a series of diagnostic tests and had surgery; she now is undergoing chemotherapy. You are the nurse who is taking care of Sue during this hospitalization. Sue is very polite and modest whenever you approach her. Sue is very quiet and never complains about any symptoms or pain. However, on several occasions, you think that Sue is in serious pain, when considering her facial expressions and sweating forehead. You think that Sues English skills may not allow her to adequately communicate with healthcare providers. Also, you nd that Sue does not have many visitorsonly her husband and two children. You frequently nd Sue praying while listening to some religious songs. You also nd Sue sobbing silently. About 2 weeks is left until Sue nishes her chemotherapy, and you think that you should do something for Sue, so she will not suffer through easily controlled pain and symptoms. Now, you begin some preliminary planning. 1. Describe your assessment of the transition(s) that Sue is experiencing. What types of transition(s) is Sue experiencing? What are the patterns of the transition(s)? What properties of transitions can you identify from her case? 2. Describe your assessment of the personal, community, and societal transition conditions that may have inuenced Sues experience. What are the cultural meanings attached to cancer, cancer pain, and symptoms accompanying chemotherapy, in this situation? What are Sues cultural attitudes toward cancer and cancer patients? How is Sues preparation for the transition(s) going? What are other factors that may facilitate her transition(s)? What are other factors that may inhibit her transition(s)?
PR SA O M PE PL R E TY C O O F N E TE L N SE T V - N IE O R T FI N
CRITICAL THINKING
Activities
1.
2.
3.
4.
Consider one specic transition that you are engaged in now. Identify characteristics of the transition as dened in Transition Theory, and observable in the transition that you are experiencing. Think about other transitions that you may be engaged in now. Think about why you chose the specic transition over other transitions that you are simultaneously experiencing. Analyze the changes that you are experiencing due to the specic transition. Think about how your level of awareness of these changes inuences your transition experience. Think about how you have been engaged in the transition and its relationship with your level of awareness of the changes. Think about how long the transition has been, and what have been the landmark events and critical points of the transition. Analyze personal, community, and societal conditions that may have inuenced the transition that you are experiencing. Think about the inuences of the meanings attached to the transition, cultural beliefs and attitudes related to the transition, socioeconomic status, and the level of your preparation for the transition and your knowledge of the transition. Describe your responses to the transition and any patterns in the responses. Ask ve friends or family members to describe what
Alligood
978-0-323-05641-0/0029
AL
3. Describe your assessment of the patterns of response that Sue is showing. What are the indicators of healthy transition(s)? What are the indicators of unhealthy transition(s)? 4. State how Transition Theory could help your assessment and nursing care for Sue. 5. As Sues nurse, what would be your rst action/ interaction to take? Describe your plan for nursing care for Sue.
428
UNIT
IV
Nursing Theories
Gaffney, K. F. (1992). Nurse practice-model for maternal role sufciency. Advances in Nursing Sciences, 15(2), 76-84. Im, E. O. (1997). Negligence and ignorance of menopause within gender multiple transition context: Low income Korean immigrant women. Unpublished doctoral dissertation, University of California, San Francisco. Im, E. O. (2005). Development of situation-specic theories: An integrative approach. Advances in Nursing Science, 28(2), 137-151. Im, E. O. (2006). A Situation-Specic Theory of Caucasian Cancer Patients Pain Experience. Advances in Nursing Science, 29(3), 232-244. Im, E. O., & Meleis, A. I. (1999a). Situation-specic theories: Philosophical roots, properties, and approach. Advances in Nursing Science, 22(2), 11-24. Im, E., & Meleis, A. I. (1999b). A situation-specic theory of Korean immigrant womens menopausal transition. Journal of Nursing Scholarship, 31(4), 333-338. Im, E., & Meleis, A. I. (2000). Meanings of menopause: low-income Korean immigrant women. Western Journal of Nursing Research, 22(1), 84-102. Im, E., & Meleis, A. I. (2001). Womens work and symptoms during midlife: Korean immigrant women. Women and Health, 33(1/2), 83-103. Im, E., Meleis, A. I., & Lee, K. (1999). Symptom experience of low-income Korean immigrant women during menopausal transition. Women and Health, 29(2), 53-67. Jones, P. S., Zhang, X. E., & Meleis, A. I. (1978). Transforming Vulnerability. Western Journal of Nursing Research, 25 (7), 835-853. Kaas,.M.J., Rousseau, G. K., (1983). Geriatric sexual conformity: assessment and intervention. Clinical Gerontologist, 2(1), 31-44. Kelley, L. S., Lakin, J. A. (1988). Role supplementation as a nursing intervention for Alzheimers disease: a case study. Public Health Nursing, 5(3), 146-152. Meleis, A. I. (1975). Role insufciency and role supplementation: A conceptual framework. Nursing Research, 24, 264-271. Meleis, A. I. (1985). Theoretical Nursing: Development and Progress (1st Ed). Philadelphia: Lippincott Williams & Wilkins. Meleis, A. I. (1991). Theoretical Nursing: Development and Progress (2nd Ed). Philadelphia: Lippincott Williams & Wilkins. Meleis, A. I. (1997). Theoretical Nursing: Development and Progress (3rd Ed). Philadelphia: Lippincott Williams & Wilkins. Meleis, A. I. (2007). Theoretical Nursing: Development and Progress (4th Ed). Philadelphia: Lippincott Williams & Wilkins. Meleis, A. I., Lipson, J., & Dallafar, A. (1998). The reluctant immigrant: immigration experiences among Middle Eastern groups in Northern California. In Baxter, D.
5.
PR SA O M PE PL R E TY C O O F N E TE L N SE T V - N IE O R T FI N
POINTS FOR
Further Study
Meleis, A. I. (2007). Theoretical Nursing: Development and Progress (4th Ed.). Philadelphia: Lippincott Williams & Wilkins. To respond to researchers increasing interest in Transition Theory, a website was established at the University of Pennsylvania: http://www.nursing.upenn.edu/dean/ transitions/
REFERENCES
Aroian, K., & Prater, M., (1988). Transitions entry groups: easing new patients adjustment to psychiatric hospitalization. Hospital and Community Psychiatry, 39, 312-313. Brackley, M. H. (1992). A role supplementation group pilot study: a nursing therapy for potential parental caregivers. Clinical Nurse Specialist, 6(1), 14-19. Bridges, W. (1980). Transitions. Reading, MA: Addison-Wesley. Bridges, W. (1991). Managing transition: Making the most of change. Menlo Park, CA: Addison Wesley. Chick, N., & Meleis, A. I. (1986). Transitions: a nursing concern. In: Chin P. L. ed. Nursing Research Methodology: Issues and Implantation. Gainsburg, MD: Aspen Publishers. Davies, S. (2005). Meleiss theory of nursing transitions and relatives experiences of nursing home entry. Journal of Advanced Nursing, 52(6), 658-671. Dracup, K., & Meleis, A. I. (1982) Compliance: an interactionist approach. Nursing Research, 31, 31-36. Dracup, K., Meleis, A. T. Baker, K , & Edlefsen, P. (1985). Familyfocused cardiac rehabilitation: a role supplementation program for cardiac patients and spouses. Nursing Clinics of North America, 19(1), 113-124. Dracup, K., Meleis, A. I., Clark, S., Clyburn, A., Shields, L., & Staley, M. (1985). Group counseling in cardiac rehabilitation: effect on patient compliance. Patient Education and Counseling, 6(4), 169-177.
Alligood
978-0-323-05641-0/0029
AL
would be their responses to the transition. Compare the descriptions given by individuals with different ages and backgrounds (e.g., ethnicity, gender, socioeconomic status). Describe what would be your outcomes of the transition. What would facilitate successful outcomes of the transition? What would inhibit successful outcomes of the transition?
Chapter 20
Afaf Ibrahim Meleis
429
& Krulfeld, R. (Eds.), Selected Papers on Refugees and Immigrants, Vol. V, (pp. 214-230). American Anthropological Association, Arlington, VA. Meleis, A. I., Sawyer, L., Im, E., Schumacher, K., & Messias, D. (2000) Experiencing transitions: an emerging middle range theory. Advances in Nursing Science, 23(1), 12-28. Meleis, A. I., & Swendsen, L. (1978). Role supplementation: an empirical test of a nursing intervention. Nursing Research, 27, 11-18. Meleis, A. I., & Trangenstein, P. A. (1994). Facilitating transitions: re-denition of the nursing mission. Nursing Outlook, 42, 255-259. Messias, D. K. H. (1997). Narratives of transnational migration, work, and health: the lived experiences of Brazilian women in the United States. Unpublished doctoral dissertation, University of California, San Francisco. Messias, D. K. H., Gilliss, C. L., Sparacino, P. S. A., Tong, E. M., & Foote, D. (1995). Stories of transition: Parents recall the diagnosis of congenital heart defects. Family Systems Medicine, 3(3/4), 367-377. Robinson, P. R., Ekman, S. L., Meleis, Al, Wahlund, L. O., & Winbald, B. (1997). Suffering in silence: the experience of early memory loss. Health Care in Later Life, 2(2), 107-120. Sawyer, L. (1997). Effects of racism on the transition to motherhood for African-American women. Unpublished doctoral dissertation, University of California, San Francisco. Schumacher, K. L. (1994). Shifting patterns of self-care and caregiving during chemotherapy. Unpublished doctoral dissertation, University of California, San Francisco. Schumacher, K. L. (1995). Family caregiver role acquisition: role-making through situated interaction. Scholarly Inquiry for Nursing Practice, 9, 211-271. Schumacher, K. L., Dodd, M. J., & Paul, S. M. (1993). The stress process in family caregivers of persons receiving chemotherapy. Research in Nursing & Health,16, 395-404. Schumacher, K. L., Jones, P. S., & Meleis, A. I. (1999). Helping elderly persons in transition: a framework for research and practice. In L. Swanson & T. Tripp Reimer (Eds.), Advances in Gerontological nursing: Life transitions in the older adult, (vol 3), (pp. 1-26). New York: Springer Publishing. Schumacher, K. L., & Meleis, A. I. (1994). Transitions: a central concept in nursing. Image: Journal of Nursing Scholarship, 26(2), 119-127. Shaul, M. P. (1997). Transition in chronic illness: rheumatoid arthritis in women. Rehabilitation Nursing, 22, 199-205. Shih, F. J., Meleis, A. I., Yu, P. J., Hu, W. Y., Lou, M. F., & Huang, G. S. (1998). Taiwanese patients concerns and coping strategies: transitions to cardiac surgery. Heart and Lung, 27(2):82-98 Walker, L. O., & Avant, K. C. (1995). Strategies for theory construction in nursing (3rd ed.). Norwalk, CT: Appleton & Lange.
Walker, L. O., & Avant, K. C. (2005). Strategies for theory construction in nursing (4th ed.). Norwalk, CT: Appleton & Lange. Weiss, M. E., Piacentine, L. B., Lokken, L., Ancona, J., Archer, J., Gresser, S., Holmes, S. B., Toman, S., Toy, A., & Vega-Stromberg, T. (2007). Perceived readiness for hospital discharge in adult medical-surgical patients. Clin Nurse Spec, 21(1), 31-42.
PR SA O M PE PL R E TY C O O F N E TE L N SE T V - N IE O R T FI N
Book Chapters
Alligood 978-0-323-05641-0/0029
BIBLIOGRAPHY Primary Sources Books
Meleis, A. I. (2007). Theoretical Nursing: Development and Progress (4th Ed). Philadelphia: Lippincott Williams & Wilkins. Brooten, D., & Naylor, M. D. (1999). Transitional Environments. In A. S. Hinshaw, S. L. Feetham, & J. Shaver (Eds), Handbook of clinical nursing research (pp. 641-654). Thousand Oaks: Sage Publications. Chick, N., & Meleis, A. I. (1986). Transitions: a nursing concern. In P. L. Chinn (Ed.), Nursing research methodology, (pp. 237-257). Boulder, CO: Aspen Publication. Lipson, J. G., & Meleis, A. I. (1999). Research with immigrants and refugees. In A. S. Hinshaw, S. L. Feetham, & J. Shaver (Eds), Handbook of clinical nursing research, (pp.87-106). Thousand Oaks: Sage Publications. Meleis, A. I. (1997). On transitions and knowledge development. Nursing Beyond Art and Science: Annotated Edition. Japan: Japan Academy of Nursing Science. Meleis, A. I. (1998). Research on role supplementation. In J. J. Fitzpatrick (Ed), Encyclopedia of Nursing Research. New Jersey: Springer Publishing. Meleis, A. I., Lipson, J., & Dallafar, A. (1998). The reluctant immigrant: immigration experiences among Middle Eastern groups in Northern California. In D., Baxter, & Krulfeld, R. (Eds.), Selected Papers on Refugees and Immigrants, Vol. V, (pp. 214-230). American Anthropological Association, Arlington, VA. Meleis, A. I., Lipson, J.G., Muecke, M., & Smith, G. (1998). Immigrant women and their health: an olive paper. Indianapolis: Sigma Theta Tau International Center Nursing Press. Meleis, A. I., & Schumacher, K. L. (1998). Transitions and health. In J. J. Fitzpatrick (Ed.), Encyclopedia of Nursing Research, (pp. 570-571). New Jersey: Springer Publishing. Meleis, A. I., & Swendsen, L. (1977). Does nursing intervention make a difference? A test of the ROSP. Communicating Nursing Research: Nursing Research Priorities: Choice or Chance, vol. 8, 308-324. Boulder, CO: Western Interstate Commission for Higher Education.
AL
430
UNIT
IV
Nursing Theories
Journal Articles
Aroian, K., Prater, M. (1988). Transitions entry groups: easing new patients adjustment to psychiatric hospitalization. Hospital and Community Psychiatry, 39, 312-313. Brackley, M. H. (1992). A role supplementation group pilot study: a nursing therapy for potential parental caregivers. Clinical Nurse Specialist, 6(1), 14-19. Dracup, K., & Meleis, A. I. (1982). Compliance: an interactionist approach. Nursing Research, 31, 31-36. Dracup, K., Meleis, Al, Baker, K., & Edlefsen, P. (1985). Family-focused cardiac rehabilitation: a role supplementation program for cardiac patients and spouses. Nursing Clinics of North America, 19(1), 113-124. Dracup, K., Meleis, A. I., Clark, S., Clyburn, A., Shields, L., & Staley, M. (1985). Group counseling in cardiac rehabilitation: effect on patient compliance. Patient Education and Counseling, 6(4), 169-177. Gaffney, K. F. (1992). Nurse practice-model for maternal role sufciency. Advances in Nursing Sciences, 15(2), 76-84. Im, E. O. (2006). A Situation-Specic Theory of Caucasian Cancer Patients Pain Experience. Advances in Nursing Science, 29(3), 232-244. Im, E., & Meleis, A. I. (1999). A situation-specic theory of Korean immigrant womens menopausal transition. Journal of Nursing Scholarship, 31(4), 333-338. Im, E., Meleis, Al, & Lee, K. (1999). Symptom experience of low-income Korean immigrant women during menopausal transition. Women and Health, 29(2), 53-67. Im, E., & Meleis, A. I. (2000). Meanings of menopause: low-income Korean immigrant women. Western Journal of Nursing Research, 22(1), 84-102. Im, E., & Meleis, A. I. (2001). Womens work and symptoms during midlife: Korean immigrant women. Women and Health, 33(1/2), 83-103. Kaas, M.J., Rousseau, G.K. (1983). Geriatric sexual conformity: assessment and intervention. Clinical Gerontologist, 2(1), 31-44. Kelley, L.S., Lakin, J.A. (1988). Role supplementation as a nursing intervention for Alzheimers disease: a case study. Public Health Nursing, 5(3), 146-152. Meleis, A. I. (1975). Role/insufciency and role supplementation: a conceptual framework. Nursing Research, 24, 264-271. Meleis, A. I. (1987). Role transition and health. Kango Kenkyo: The Japanese Journal of Nursing Research, 20(1), 81, 69-89. Meleis, A. I. (1991). Between two cultures: identity, roles, and health. Health Care For Women International, 12, 365-378. Meleis, A. I. (1997). Immigrant transitions and health care: an action plan. Nursing Outlook, 45(1), 42. Meleis, A. I., & Rogers, S. (1987). Women in transition: being vs. becoming or being and becoming. Health Care for Women International, 8, 199-217.
PR SA O M PE PL R E TY C O O F N E TE L N SE T V - N IE O R T FI N
Dissertations
Almendarez, B. L. (2007). Mexican American elders and nursing home transition. Unpublished doctoral dissertation, University of Texas Health Science Center at San Antonio, TX. Batty, M. L. E. (1999). Pattern identication and expanding consciousness during the transition of low-risk pregnancy. A study embodying Newmans health as expanding consciousness. Unpublished doctoral dissertation, University of New Brunswick, Canada. Fowles, E. R. (1994). The relationship between prenatal maternal attachment, postpartum depressive symptoms, and maternal role attainment. Loyola University of Chicago, Chicago, IL. Im, E-O. (1997). Negligence and ignorance of menopause within gender multiple transition context: Low income Korean immigrant women. Unpublished doctoral dissertation, University of California, San Francisco, CA. Kelly, C. (1997). Restructuring public health nursing: experiences in Northern California. Unpublished doctoral dissertation, University of California, San Francisco, CA. Lenz, B. K. (2002). Correlates of tobacco use and non-use among college students at a large university: Application of a transition framework. Unpublished doctoral dissertation, University of Minnesota, MN. McMillan, E. S. (2002). Education to practice questionnaire: A content analysis. Unpublished doctoral dissertation, Wilmington College Division of Nursing, Delaware. Missal, B. E. (2003). The Gulf Arb womans transition to motherhood. Unpublished doctoral dissertation, University of Minnesota. OBrien-Barry, P. (2003). The contribution of sex-role orientation and role commitment to interrole conict in working rst-time mothers at 6 to 9 months postpartum. Unpublished doctoral dissertation, New York University, New York. Sawyer, L. (1997). Effects of racism on the transition to motherhood for African-American women. Unpublished doctoral dissertation, University of California, San Francisco.
Alligood 978-0-323-05641-0/0029
Meleis, A. I., Swendsen, L., & Jones, D. (1980). Preventive role supplementation: a grounded conceptual framework. In M.H. Miller and B. Flynn (Eds.), Current perspectives in nursing: Social issues and trends, (vol. 2), (pp. 3-14). St. Louis, MO: C.V. Mosby. Schumacher, K. L., Jones, P. S., & Meleis, A. I. (1998). The elderly in transition: need and issues of care. In L. Swanson & T. Tripp Reimer, Advances in Gerentological Nursing. New York: Springer Publishing Comp. Schumacher, K. L., Jones, P.S., & Meleis, A. I. (1999). Helping elderly persons in transition: a framework for research and practice. In L. Swanson & T. Tripp Reimer (Eds.), Advances in Gerontological nursing: Life transitions in the older adult, (vol 3), (pp. 1-26). New York: Springer Publishing.
AL
Chapter 20
Afaf Ibrahim Meleis
431
PR SA O M PE PL R E TY C O O F N E TE L N SE T V - N IE O R T FI N
Book Chapters Journal Articles Secondary Sources Books
Meleis, A. I. (2001). Guest editor of a special issue on News From The International Council On Womens Health Issues for Health Care for Women International, 22(3). Meleis, A. I. (2001). Guest editor of a special issue on women and violence for Health Care for Women International, 22(4).
Alligood 978-0-323-05641-0/0029
Meleis, A. I., Sawyer L., Im, E., Schumacher, K., & Messias, D. (2000). Experiencing transitions: an emerging middle range theory. Advances in Nursing Science, 23(1), 12-28. Meleis, A. I., & Swendsen, L. (1978). Role supplementation: an empirical test of a nursing intervention. Nursing Research, 27, 11-18. Meleis, A. I., & Trangenstein, P. A. (1994). Facilitating transitions: redenition of a nursing mission. Nursing Outlook, 42(6), 255-259. Messias, D. K. H. (2002). Transnational health resources, practices, and perspectives: Brazilian immigrant womens narratives. Journal of Immigrant Health, (4)4, 183-200. Messias, D. K. H., Gilliss, C. L., Sparacino, P. S. A , Tong, E. M., and Foote, D. (1995). Stories of transition: Parents recall the diagnosis of congenital heart defect. Family Systems Medicine, 13(3;4), 367-277. Robinson, P. R., Ekman, S. L., Meleis, AI, Wahlund, L.O., & Winbald, B. (1997). Suffering in silence: the experience of early memory loss. Health Care in Later Life, 2(2), 107-120. Schumacher, K. L. (1995). Family caregiver role acquisition: role-making through situated interaction. Scholarly Inquiry for Nursing Practice, 9, 211-271. Schumacher, K. L. (1996). Reconceptualizing family caregiving: family-based illness care during chemotherapy. Research in Nursing & Health, 19, 261-272. Schumacher, K. L., Dodd, M. J., & Paul, S. M. (1993). The stress process in family caregivers of persons receiving chemotherapy. Research in Nursing & Health, 16, 395-404. Schumacher, K. L., & Meleis, A. I. (1994). Transitions: a central concept in nursing. Image: Journal of Nursing Scholarship, 26(2), 119-127. Schumacher, K. L., Stewart, B. J., & Archbold, P.G. (1998). Conceptualizing and measurement of doing family caregiving well. Image: Journal of Nursing Scholarship, 30(1): 63-69 Shaul, M. P. (1997). Transition in chronic illness: rheumatoid arthritis in women. Rehabilitation Nursing, 22, 199-205. Shih, F. J., Meleis, A. I., Yu, P. J., Hu, W. Y., Lou, M. F., & Huang, G. S. (1998). Taiwanese patients concerns and coping strategies: transitions to cardiac surgery. Heart and Lung, 27(2):82-98 Swendsen, L., Meleis, A. I., & Jones, D. (1978). Role supplementation for new parents: a role mastery plan. The American Journal of Maternal Child Nursing, 3, 84-91.
Meleis, A. I. (2001) (Ed.). Womens work, health and quality of life. Binghamton: Haworth Press, Inc. Meleis, A. I., Isenberg, M., Koerner, J. E., Lacey, B., & Stern, P. (1995). Diversity, marginalization, and culturally competent health care: Issues in knowledge development. Washington: American Academy of Nursing. Meleis, A. I., Lipson, J. G., Muecke, M., & Smith, G. (1998). Immigrant Women and their Health: An Olive Paper. Indianapolis, IN: Center for Nursing Press, Sigma Theta Tau. St. Hill, P.,Lipson, J., & Meleis, A. I. (2002)(Eds.). Caring for Women Cross-Culturally: A Portable Guide, Philadelphia: F.A. Davis. Meleis, A. I. (2002). Egyptians. In P. St. Hill, J. Lipson, & A. Meleis (Eds.). Caring for Women Cross-Culturally: A Portable Guide, Philadelphia: F. A. Davis. [AJN Book of the Year Award 2004] Meleis, A. I., Lipson, J., & Dallafar, A. The reluctant immigrant: immigration experiences among Middle Eastern groups in Northern California. In D. Baxter, & Krulfeld, R. (Eds.), Selected Papers on Refugees and Immigrants, Vol. V, (pp. 214-230). American Anthropological Association, Arlington, VA. Arruda, E. N., Larson, & Meleis A. I. (1992). Comfort: Immigrant Hispanic patients views. Cancer Nursing, 15(6), 387-394. Barnes, D., Eribes, C., Juarbe, T., Nelson, M., Proctor, S., Sawyer, L., Shaul, M., & Meleis, A. I. (1995). Primary health care and primary care: A Confusion of philosophies. Nursing Outlook, 43, 7-16. Bernal, P., & Meleis, A. I. (1995). Being a mother and a por dia domestic worker: Companionship and deprivation. Western Journal of Nursing Research, 17(4), 365-382. Bernal, P., & Meleis, A. I. (1995). Self care actions of Colombian por da domestic workers: On prevention and care. Women and Health, 22(4), 77-95. Budman, C.L., Lipson, J.G. & Meleis, A. I. (1992). The cultural consultant in mental health care: The case of an Arab adolescent. American Journal of Orthopsychiatry, 62(3), 359-370. Davidson, P., Meleis, A. I., Daly, J., & Douglas, M. (2003). Globalization as we enter the 21st century: Reections and directions for nursing education, science, research and clinical practice. Contemporary Nurse, 15(3), 162-174. Davis, L.H., Flaherty, S., & Meleis, A. I., et al. (1992). Culturally competent health care. Nursing Outlook, 40(6), 277-283. Douglas, M. K., Meleis, A. I., Eribes, C. and Kim, S. (1996). The work of auxiliary nurses in Mexico: Stressors, satisers and coping strategies, Journal of International Nursing Studies, 33(5), 495-505.
AL
432
UNIT
IV
Nursing Theories
Jones, P. S., Jaceldo, K. B., Lee, J. R., Zhang, X. E., & Meleis, A. I. (2001). Role integration and perceived health in Asian American women caregivers. Research in Nursing and Health, 24, 133-144. Jones, P. S. & Meleis, A. I. (1993). Health is empowerment. Advances in Nursing Science, 15(3), 1-14. Jones, P. S., Zhang, X. E., & Meleis, A. I. (1978). Transforming Vulnerability. Western Journal of Nursing Research, 25(7), 835-853. Meleis, A. I. (1992). Community participation and involvement: Theoretical and empirical issues. Health Services Management Research, 5(10), 5-16. Meleis, A. I. (1992). Directions for nursing theory development in 21st century. Nursing Science Quarterly, 5(3), 112-117. Meleis, A. I. (1992). On the way to scholarship: From masters to doctorate. Journal of Professional Nursing, 8(6), 328-334. Meleis, A. I. (1992, June). Nursing: A caring science with a distinct domain. Sairaanhoitaja, pp. 8, 10, 11 & 12. Meleis, A. I. (1996). Culturally competent scholarship: Substance and rigor. Advances in Nursing Science, 19(2), 1-16. Meleis, A. I. (2001). Small steps and giant hopes: violence on women is more than wife battering. Health Care For Women International, 23, 313-315 (Editorial). Meleis, A. I. (2001). Womens work, health and quality of life: It is time we redene womens work. Women and Health, 33(1/2), xv-xviii. Meleis, A. I. (2002). Whither international research? Journal of Nursing Scholarship, First Quarter 4-5 (Editorial). Meleis, A. I. (2003). Brain Drain or Empowerment. Journal of Nursing Scholarship, 35(2), 105. (Guest Editorial). Meleis, A. I. (2005). Shortage of nurses means a shortage of nurse scientists. (Editorial). Journal of Advanced Nursing, 49, (2), 111. Meleis, A. I. (2005). Safe womanhood is not safe motherhood: policy implications. Health Care for Women International, 26(2), 464-471. Meleis, A. I. Arabs. In J. Lipson, & S. Dibble, (Eds.). (2005). Culture and Clinical Care: A Practical Guide. San Francisco: UCSF Nursing Press. (pp. 42-57). Meleis, A. I. Human Capital in Health Care: A Resource Crisis of a Caring Crisis? (2006, June-July). Global Health Link, (139), 6-7, 21-22. Meleis, A. I., Arruda, E.N., Lane, S. & Bernal, P. (1994). Veiled, voluminous and devalued: Narrative stories about lowincome women from Brazil, Egypt & Colombia. Advances in Nursing Science, 17(2), 1-15. Meleis, A. I. & Bernal, P. (1994). Domestic workers in Colombia as spouses: Security and servitude. Holistic Nursing, 8(4), 33-43. Meleis, A. I. & Bernal, P. (1995). The paradoxical world of muchacha de por da in Colombia. Human Organization, 54, 393-400.
Douglas, M. K., Meleis, A. I., & Paul, S. M. (1997). Auxiliary nurses in Mexico: Impact of multiple roles on their health. Health Care for Women International, 18(44), 355-368. Dracup, K., Cronenwett, L., Meleis, A. I., & Benner, P.E. (2005). Reections on the Doctorate of Nursing Practice. Nursing Outlook, 53(4), 177-182. Dracup, K., Cronenwett, L., Meleis, A. I. & Benner, P.E. (2005). Reply to Letter to the Editor on Reections on the Doctorate of Nursing Practice. Nursing Outlook, 53(6), 269. Facione, N. C., Dodd, M., Holzemer, W., & Meleis, A. I. (1997). Help seeking for self discovered breast symptoms: Implications for early detection. Cancer Practice, 5(4), 220-227. Hall, J. M., Stevens, P. E. & Meleis, A. I. (1992). Developing the construct of role integration: A narrative analysis of women clerical workers daily lives. Research in Nursing & Health, 15(6), 447-457. Hall, J. M., Stevens, P. E., & Meleis, A. I. (1992). Experiences of women clerical workers in patient care areas. Journal of Nursing Administration, 22(5), 11-17. Hall, J. M., Stevens, P. E. & Meleis, A. I. (1994). Marginalization: A guiding concept for valuing diversity in nursing knowledge development. Advances in Nursing Science, 16(4), 23-41. Hattar-Pollara, M. & Meleis, A. I. (1995). Stress of immigration and the daily lived experience of Jordanian immigrant women. Western Journal of Nursing Research, 17(5), 521-539. Hattar-Pollara, M., & Meleis, A. I. (1995). Parenting adolescents: The experiences of Jordanian immigrant women in California. Health Care for Women International, 16(3), 195-211. Hattar-Pollara, M., Meleis, A. I. & Nagib, H. (2000). A study of the spousal role of Egyptian women in clerical jobs. Health Care For Women International, 21(4), 305-317. Hattar-Pollara, M., Meleis, A. I., & Nagib, H. (2003). Multiple role stress and patterns of coping of Egyptian Women in Clerical Jobs. Transcultural Nursing, 14(2), 125-133. Im, E., Meleis, A. I. & Lee, K. A. (1999). Cultural competence of measurement scales of menopausal symptoms: use in research among Korean women. International Journal of Nursing Studies, 36 455-463. Im, E., Meleis, A. I. & Park, Y. S. (1999). A feminist critique of the research on menopausal experience of Korean women. Research In Nursing and Health, 22 410-420. Im, E., & Meleis, A. I. (2001). An international imperative for gender-sensitive theories in womens health. Journal of Nursing Scholarship, 33(4), 309-314. Jones, P., & Meleis, A. I. (2002). Caregiving Between Two Cultures: An Integrative Experience. Journal of Transcultural Nursing, 13(3), 202-209.
PR SA O M PE PL R E TY C O O F N E TE L N SE T V - N IE O R T FI N
Alligood 978-0-323-05641-0/0029
AL
Chapter 20
Afaf Ibrahim Meleis
433
PR SA O M PE PL R E TY C O O F N E TE L N SE T V - N IE O R T FI N
Alligood 978-0-323-05641-0/0029
Meleis, A. I., Douglas, M., Eribes, C., Shih, F., & Messias, D. (1996). Employed Mexican women as mothers and partners: Valued, empowered and overloaded. Journal of Advanced Nursing, 23, 82-90. Meleis, A. I. & Dracup, K. (2005, September 30). The Case Against the DNP: History, Timing, Substance, and Marginalization. Online Journal of Issues in Nursing. 10(3), Manuscript 2: www.nursingworld.org/ojin/topic28/ tpc28_2.htm Meleis, A. I. & Fishman, J. (2001). Rethinking the work in health: gendered and cultural expectations. Health Care For Women International, 22, 195-197 (Editorial). Meleis, A. I., Hall, J. M. Stevens, P. E. (1994). Scholarly caring in doctoral nursing education: Promoting diversity and collaborative mentorship. Image: Journal of Nursing Scholarship, 26(3), 177-180. Meleis, A. I., & Im, E. (1999). Transcending marginalization in knowledge development. Nursing Inquiry, 6(2), 94-102. Meleis, A. I., & Im, E. (2002). Grandmothers and womens health: For Integrative and coherent models of womens health. Health Care for Women International. 23, (2), 207-224. Meleis, A. I. & Lindgren, T. (2001). Show me a woman who does not work! Journal of Nursing, Third Quarter, 209-210. Meleis, A. I. & Lipson, J. (2003). Cross-cultural health and strategies to lead development of nursing practice. In J. Daly, S. Speedy, & D. Jackson (Eds.). (2003). Nursing Leadership, (pp. 69-88). Philadelphia: Churchill Livingstone. Meleis, A. I., Lipson J.G., & Paul, S.M. (1992). Ethnicity and health among ve Middle Eastern immigrant groups. Nursing Research, 41(2), 98-103. Meleis, A. I. & Messias, D. K. H., & Arruda, E. N. (1995). Womens work environment and health: Clerical workers in Brazil. Research in Nursing and Health, 19, 53-62. Meleis, A. I. & Stevens, P. E. (1992). Women in clerical jobs: Spousal role satisfaction stress and coping. Women & Health, 18(1), 23-40.
Messias, D. K. H., Hall, J. M., Meleis, A. I. (1996). Voices of impoverished Brazilian women: Health implications of roles and resources. Women and Health, 24(1), 1-20. Messias, D.K.H., Im, E., Page, A., Regev, H., Spiers, J., & Meleis, A. I. (1997). Dening and redening work: Implications for womens health. Gender and Society, 11(3), 296-323. Messias, D.H., Regev, H., Im, E., Spiers, J., Van, P., & Meleis, A. I. (1997). Expanding the visibility of womens work: Policy implications. Nursing Outlook, 45, 258-264. Nelson, M., Proctor, S., Regev, H., Barnes, D., Sawyer, L., Messias, D., Yoder, L., & Meleis, A. I. (1996). The Cairo action plan: A challenge to nursing. Image: Journal of Nursing Scholarship, 28(1), 75-80. Sawyer, L., Regev, H., Proctor, S., Nelson, M., Messias, D., Barnes, D., Meleis, A. I. (1995). Matching vs. cultural competence in research a methodological note. Research in Nursing and Health, 18, 531-541. Siantz, M.L. & Meleis, A. I. (2007). Integrating Cultural Competence into Nursing Education & Practice: 21st Century Action Steps. Journal of Transcultural Nursing, 18(1), 86-90. Stevens, P.E., Hall, J.M., & Meleis, A. I. (1992). Examining vulnerability of women clerical workers from ve ethnic racial groups. Western Journal of Nursing Research, 14(6), 754-774. Stevens, P.E., Hall, J. M. & Meleis, A. I. (1992). Narratives as a basis for culturally relevant holistic care: Ethnicity and everyday experiences of women clerical workers. Holistic Nursing Practice, 6(3), 49-58. Van, P. & Meleis, A. I. (2003). Coping with grief after involuntary pregnancy loss: perspectives of African-American Women. Journal of Obstetric, Gynecological & Neonatal Nursing, 32(1), 28-39.
AL
You might also like
- Chapter 20 - Transitions TheoryDocument18 pagesChapter 20 - Transitions Theoryslb_21100% (3)
- BSN 1-D Nursing Theorists and ModelsDocument6 pagesBSN 1-D Nursing Theorists and ModelsRenzy Mayven Pedriña LobatonNo ratings yet
- Transition TheoryDocument36 pagesTransition TheoryMatty Jolbitado100% (1)
- Madeleine Leininger's BiographyDocument3 pagesMadeleine Leininger's BiographyDennis Nabor Muñoz, RN,RM100% (6)
- Final Wiki - Martha RogersDocument4 pagesFinal Wiki - Martha Rogerslms93093No ratings yet
- Ray's Theory of Bureaucratic CaringDocument12 pagesRay's Theory of Bureaucratic CaringGladys YaresNo ratings yet
- Examples of Abdellah's Publications: TestabilityDocument3 pagesExamples of Abdellah's Publications: TestabilityleewfNo ratings yet
- Madeleine LeiningerDocument10 pagesMadeleine LeiningerDanica MerinNo ratings yet
- Martha Rogers: Katelyn Brooks, Sarah Enke, Lexie Scribner, Alyssa JasperDocument5 pagesMartha Rogers: Katelyn Brooks, Sarah Enke, Lexie Scribner, Alyssa JasperKatelyn BrooksNo ratings yet
- Theory CritiqueDocument16 pagesTheory CritiqueArceo AbiGailNo ratings yet
- TheoristDocument130 pagesTheoristLucelle MacahiligNo ratings yet
- Reva Rubin Dan Ramona MercerDocument8 pagesReva Rubin Dan Ramona MercerFifi FruitasariNo ratings yet
- Dorothea Orem Research PaperDocument8 pagesDorothea Orem Research Paperefdvje8d100% (3)
- Rosemarie Rizzo Parse's Human Becoming TheoryDocument6 pagesRosemarie Rizzo Parse's Human Becoming TheoryAmeng GosimNo ratings yet
- CoffmanNsgtheoristandtheirworkfor8thed April2012Document37 pagesCoffmanNsgtheoristandtheirworkfor8thed April2012Cyntia Theresia LumintangNo ratings yet
- Transcultural Nursing TheoryDocument20 pagesTranscultural Nursing TheoryAna VitanzosNo ratings yet
- TFN - RosaDocument18 pagesTFN - RosaRosemarie AngelesNo ratings yet
- Modeling and Role Modeling TheoryDocument18 pagesModeling and Role Modeling Theorypam11867% (3)
- Biography of Nola PenderDocument3 pagesBiography of Nola PenderKarleen Marie AlbinoNo ratings yet
- Critique of TheoryDocument3 pagesCritique of Theorykookai8100% (1)
- 1111Document6 pages1111Suoth, Eudia EukaristyNo ratings yet
- Group 3Document10 pagesGroup 3alyssajairaaNo ratings yet
- Joyce Travelbee: Human To Human Relationship ModelDocument3 pagesJoyce Travelbee: Human To Human Relationship ModelKarlo Gil ConcepcionNo ratings yet
- Roscelferrer Assignment2 ScholarlypaperDocument9 pagesRoscelferrer Assignment2 Scholarlypaperapi-520011052No ratings yet
- Module 3: Theoretical Foundations of NursingDocument7 pagesModule 3: Theoretical Foundations of NursingJennifer SpoonerNo ratings yet
- Nursing Theory of Ramona T. Mercer MaterDocument8 pagesNursing Theory of Ramona T. Mercer MaterMark Norriel Cajandab100% (1)
- Module 7 2023Document56 pagesModule 7 2023jamsineNo ratings yet
- Dr. Jean Watson's Caring Theory GuideDocument19 pagesDr. Jean Watson's Caring Theory GuideKomal RamzaanNo ratings yet
- Ramona T MercerDocument14 pagesRamona T MercerSyanti Dewi Tamher Jusuf100% (2)
- Feminist Therapy 1Document44 pagesFeminist Therapy 1mancerajellagNo ratings yet
- Transcultural Nursing Theory OverviewDocument33 pagesTranscultural Nursing Theory OverviewWinter SonataNo ratings yet
- Cultural CareDocument10 pagesCultural Caresasmita putriNo ratings yet
- Ramona Mercer's Maternal Role TheoryDocument21 pagesRamona Mercer's Maternal Role TheoryNanda LaiyaaNo ratings yet
- Maternal Role AttainmentDocument6 pagesMaternal Role AttainmentRudhy RizalNo ratings yet
- Jean Watson (TFN-3)Document11 pagesJean Watson (TFN-3)Bel EspañolaNo ratings yet
- Jean Watson (TFN-3)Document11 pagesJean Watson (TFN-3)Bel EspañolaNo ratings yet
- Current Trends in Nursing Theories: ProfessionandsocietyDocument10 pagesCurrent Trends in Nursing Theories: ProfessionandsocietyDeff HaningNo ratings yet
- 00 Health Promotion ModelDocument21 pages00 Health Promotion Modelapi-313117831100% (1)
- Edited by James Gillett - Health and Society - Critical Perspectives-Oxford University Press (2016)Document298 pagesEdited by James Gillett - Health and Society - Critical Perspectives-Oxford University Press (2016)Pari RanaNo ratings yet
- Theoretical Framework For Nursing PracticeDocument55 pagesTheoretical Framework For Nursing PracticeMara Mae de GorostizaNo ratings yet
- The Psychodynamics of Medical Practice: Unconscious Factors in Patient CareFrom EverandThe Psychodynamics of Medical Practice: Unconscious Factors in Patient CareNo ratings yet
- Biography of Madeleine LeiningerDocument15 pagesBiography of Madeleine LeiningerSamantha Perez DumukNo ratings yet
- Katie Eriksson (Theory of Caritative Caring) 1943-2019Document9 pagesKatie Eriksson (Theory of Caritative Caring) 1943-2019guadalupedeamargaretNo ratings yet
- Trancultural Theory in Nursing Theory of Culture Care Diversity and UniversalityDocument17 pagesTrancultural Theory in Nursing Theory of Culture Care Diversity and UniversalityKara Kristine Tuano NarismaNo ratings yet
- Lazarus TheoryDocument10 pagesLazarus TheoryAlwiNo ratings yet
- Candace Merl E. Gahisan BSN 1 - A Nursing Theorist: Katharine Kolcaba Title of Theory: Theory of Comfort Nursing Background: EducationDocument14 pagesCandace Merl E. Gahisan BSN 1 - A Nursing Theorist: Katharine Kolcaba Title of Theory: Theory of Comfort Nursing Background: EducationCandace Merl E. GahisanNo ratings yet
- Health Promotion Model V.1Document21 pagesHealth Promotion Model V.1Roshin TejeroNo ratings yet
- TheoristsDocument7 pagesTheoristsastraia celesteNo ratings yet
- Transcultural Nursing Care Concepts Text Provides FrameworkDocument5 pagesTranscultural Nursing Care Concepts Text Provides FrameworkkaymaileNo ratings yet
- 337 366Document59 pages337 366mickshaw555No ratings yet
- Martha Rogers: Presented By: Lyndsi Byers, Geena Griffin, Chelsea Hoy and Mallory ShepardDocument18 pagesMartha Rogers: Presented By: Lyndsi Byers, Geena Griffin, Chelsea Hoy and Mallory ShepardChelsea Hoy100% (2)
- Dorothyjohnson 160309200153 PDFDocument7 pagesDorothyjohnson 160309200153 PDFBheru LalNo ratings yet
- Virginia Henderson Biography and Need TheoryDocument15 pagesVirginia Henderson Biography and Need TheoryDazell VarronNo ratings yet
- Credentials and Background of The TheoristDocument13 pagesCredentials and Background of The TheoristRHUBY ABENOJANo ratings yet
- TFN Dorothy JohnsonDocument6 pagesTFN Dorothy JohnsonHershel GalinatoNo ratings yet
- Newman's Theory of Health as Expanding ConsciousnessDocument13 pagesNewman's Theory of Health as Expanding ConsciousnessJun ManNo ratings yet
- Dorothea Orem's Self-Care Deficit TheoryDocument12 pagesDorothea Orem's Self-Care Deficit TheoryMarlouAgananNo ratings yet
- DES Daughters, Embodied Knowledge, and the Transformation of Women's Health Politics in the Late Twentieth CenturyFrom EverandDES Daughters, Embodied Knowledge, and the Transformation of Women's Health Politics in the Late Twentieth CenturyNo ratings yet
- Patients and Healers in the Context of Culture: An Exploration of the Borderland between Anthropology, Medicine, and PsychiatryFrom EverandPatients and Healers in the Context of Culture: An Exploration of the Borderland between Anthropology, Medicine, and PsychiatryRating: 4 out of 5 stars4/5 (4)
- Chapter 2 and 3 (Edited)Document30 pagesChapter 2 and 3 (Edited)Hazel RoseNo ratings yet
- Research LocaleDocument2 pagesResearch LocaleHazel RoseNo ratings yet
- CDEDocument16 pagesCDEHazel RoseNo ratings yet
- Kendall W PaperDocument20 pagesKendall W PapercliffyeungNo ratings yet
- A. Skills 30 % B. Knowledge A. Requirements 20% B. Exam 30% C. Attitude 10% A. Attendance 10% 100%Document1 pageA. Skills 30 % B. Knowledge A. Requirements 20% B. Exam 30% C. Attitude 10% A. Attendance 10% 100%Hazel RoseNo ratings yet
- Psychiatric Nursing SlidesDocument27 pagesPsychiatric Nursing SlidesHazel RoseNo ratings yet
- ReferencesDocument1 pageReferencesHazel RoseNo ratings yet
- Table ThesisDocument12 pagesTable ThesisHazel RoseNo ratings yet
- HTTPDocument1 pageHTTPHazel RoseNo ratings yet
- Psych OtherDocument27 pagesPsych OtherHazel RoseNo ratings yet
- APPENDICITISDocument6 pagesAPPENDICITISHazel RoseNo ratings yet
- Clinical Teaching Plan On Ncm-105 Psyhciatric NursingDocument13 pagesClinical Teaching Plan On Ncm-105 Psyhciatric NursingHazel RoseNo ratings yet
- Respiratory: Common Lab Tests For Respiratory DisordersDocument27 pagesRespiratory: Common Lab Tests For Respiratory DisordersGlenn Daryll SantosNo ratings yet
- SWOT AnalysisDocument9 pagesSWOT AnalysisAshraf Ali Smadi88% (24)
- NCM 105 SyllabusDocument5 pagesNCM 105 SyllabusHazel Rose0% (1)
- 01797johari WindowDocument23 pages01797johari WindowAjay Kumar ChoudharyNo ratings yet
- Segmentation of Shoppers Using Their Behaviour: A Research Report ONDocument68 pagesSegmentation of Shoppers Using Their Behaviour: A Research Report ONpankaj_20082002No ratings yet
- The Lost Art of Lama Fera Tibetan HealingDocument5 pagesThe Lost Art of Lama Fera Tibetan HealingAnonymous A1LQIfKNo ratings yet
- Witch Wars Defense Manual PDFDocument99 pagesWitch Wars Defense Manual PDFAlrica NeshamaNo ratings yet
- Max Weber's Insights on Science as a ProfessionDocument21 pagesMax Weber's Insights on Science as a ProfessionVivek Nemana100% (2)
- Principles of Management - PSOCCDocument32 pagesPrinciples of Management - PSOCCEden EscaloNo ratings yet
- Vagabond PhilosophiesDocument5 pagesVagabond Philosophiesarpitaniruddh2007No ratings yet
- Edward T. Hall - Beyond Culture-Doubleday (1976)Document384 pagesEdward T. Hall - Beyond Culture-Doubleday (1976)Tristan ZarateNo ratings yet
- Intelligence PDFDocument19 pagesIntelligence PDFmiji_ggNo ratings yet
- They Say I SayDocument12 pagesThey Say I Sayapi-235243278No ratings yet
- Announcement SoalDocument8 pagesAnnouncement SoalirmansyahNo ratings yet
- The Happiness EffectDocument2 pagesThe Happiness EffectClaudene GellaNo ratings yet
- PGDUPDL Assignments (2018 July and 2019 January Sessions)Document4 pagesPGDUPDL Assignments (2018 July and 2019 January Sessions)santoshspavNo ratings yet
- Ecosoc Chair ReportDocument9 pagesEcosoc Chair Reportapi-408542393No ratings yet
- The Fun They HadDocument2 pagesThe Fun They HadAdit Bohra VIII BNo ratings yet
- 1 - Looking at Language Learning StrategiesDocument18 pages1 - Looking at Language Learning StrategiesTami MolinaNo ratings yet
- Coxj Ogl321 Mod1 Paper Final For 481Document5 pagesCoxj Ogl321 Mod1 Paper Final For 481api-561877895No ratings yet
- Formulating Specific Research QuestionsDocument4 pagesFormulating Specific Research Questionsaan_9No ratings yet
- What I Need To Know: Learning ObjectivesDocument10 pagesWhat I Need To Know: Learning ObjectivesManuelo VangieNo ratings yet
- CV Summary for Ilona Nadasdi-NiculaDocument3 pagesCV Summary for Ilona Nadasdi-NiculaCarmen ZaricNo ratings yet
- Final MBBS Part I Lectures Vol I PDFDocument82 pagesFinal MBBS Part I Lectures Vol I PDFHan TunNo ratings yet
- The Veldt by Ray Bradbury: JavierDocument5 pagesThe Veldt by Ray Bradbury: Javierapi-334247362No ratings yet
- Unwinding AnxietyDocument11 pagesUnwinding Anxietylim hwee lingNo ratings yet
- Adjudication Considerations For British Parliamentary Debate PDFDocument20 pagesAdjudication Considerations For British Parliamentary Debate PDFAcbel Rnuco100% (1)
- Acc EducationalDocument42 pagesAcc EducationalDian AdvientoNo ratings yet
- Modul Q Gradder Class PDFDocument446 pagesModul Q Gradder Class PDFbudimanheryantoNo ratings yet
- Group 2 ReportDocument77 pagesGroup 2 ReportZhelParedesNo ratings yet
- Marketing Yourself Handout (1) : Planning Phase Situation AnalysisDocument6 pagesMarketing Yourself Handout (1) : Planning Phase Situation AnalysisSatya Ashok KumarNo ratings yet
- Mr Collins' proposal rejectedDocument5 pagesMr Collins' proposal rejectedabhishek123456No ratings yet
- 17 Tips Taking Initiative at WorkDocument16 pages17 Tips Taking Initiative at WorkHarshraj Salvitthal100% (1)