You might also like
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- The Predominantly Plant-Based Pregnancy GuideDocument179 pagesThe Predominantly Plant-Based Pregnancy GuidePriscila Tobar Alcántar100% (1)
- Hiper Hipoparatir NejmDocument13 pagesHiper Hipoparatir NejmPriscila Tobar AlcántarNo ratings yet
- Ajuste de Dosis de Medicamentos en Paciente RenalDocument46 pagesAjuste de Dosis de Medicamentos en Paciente RenalThelma Cantillo RochaNo ratings yet
- La Teta Cansada - Montserrat Reverte PDFDocument4 pagesLa Teta Cansada - Montserrat Reverte PDFIpNo ratings yet
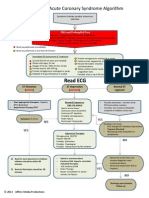
- ACS Algorithm DiagramDocument1 pageACS Algorithm DiagramPriscila Tobar Alcántar100% (1)
- Diabetic KetoacidosisDocument16 pagesDiabetic Ketoacidosisdrtpk100% (2)
- Breastfeeding Medicine Protocol on GalactogoguesDocument8 pagesBreastfeeding Medicine Protocol on GalactogoguespaulinaovNo ratings yet
- MayoClinProc Anemia in Adults A Contemporary Approach To DiagnosisDocument7 pagesMayoClinProc Anemia in Adults A Contemporary Approach To DiagnosisBarbarita Alvarado CamposNo ratings yet
- Acute Appendicitis in Adults ManagementDocument16 pagesAcute Appendicitis in Adults ManagementPriscila Tobar AlcántarNo ratings yet
- Myxedema AscitesDocument4 pagesMyxedema AscitesPriscila Tobar AlcántarNo ratings yet
- Acute Appendicitis in AdultsDocument20 pagesAcute Appendicitis in AdultsPriscila Tobar AlcántarNo ratings yet
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (894)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- HCC GuidebookDocument153 pagesHCC Guidebookleadmonkeyboy100% (2)
- Deteksi Dini Kegawatdaruratan Maternal Dan Neonatal (RS Persada Medika Cikampek) PEBDocument10 pagesDeteksi Dini Kegawatdaruratan Maternal Dan Neonatal (RS Persada Medika Cikampek) PEBindra pradjaNo ratings yet
- Magic Wave July 2011 PDF 69Document19 pagesMagic Wave July 2011 PDF 69Budi TurmokoNo ratings yet
- Marketing Plan LKDFNDDocument3 pagesMarketing Plan LKDFNDapi-392259592No ratings yet
- Nutrition ManualDocument405 pagesNutrition ManualRaghavendra Prasad100% (1)
- Acanthosis NigricansDocument32 pagesAcanthosis NigricansZeliha TürksavulNo ratings yet
- Anatomia SufletuluiDocument1 pageAnatomia SufletuluiAlexandrina DeaşNo ratings yet
- Genetically Engineered Insulin and Its Pharmaceutical AnaloguesDocument11 pagesGenetically Engineered Insulin and Its Pharmaceutical AnaloguesNatália ZeninNo ratings yet
- DR Sibli PDFDocument19 pagesDR Sibli PDFIva Dewi Permata PhilyNo ratings yet
- Diabetes and Stroke RisksDocument26 pagesDiabetes and Stroke RisksPrecious SantayanaNo ratings yet
- Shoulder DystociaDocument13 pagesShoulder Dystociarolla_hiraNo ratings yet
- Risk Factors for PeriodontitisDocument174 pagesRisk Factors for PeriodontitisdevikaNo ratings yet
- National Geographic March 2016Document148 pagesNational Geographic March 2016Anonymous Azxx3Kp9No ratings yet
- Step 1 UworldDocument25 pagesStep 1 UworldKarl Abiaad100% (23)
- Dietary Management of Indian Vegetarian Diabetics: M. Viswanathan and V. MohanDocument2 pagesDietary Management of Indian Vegetarian Diabetics: M. Viswanathan and V. Mohanrockingtwo07No ratings yet
- Hemo Glucose TestDocument3 pagesHemo Glucose TestrocheNo ratings yet
- FIT UK Recommendations For Injection TechniqueDocument48 pagesFIT UK Recommendations For Injection TechniqueMadeleine OchianuNo ratings yet
- The UK Prospective Diabetes Study (UKPDS) : Clinical and Therapeutic Implications For Type 2 DiabetesDocument6 pagesThe UK Prospective Diabetes Study (UKPDS) : Clinical and Therapeutic Implications For Type 2 DiabetesLaila KurniaNo ratings yet
- AAHA Diabetes Guidelines - FinalDocument21 pagesAAHA Diabetes Guidelines - FinalKátia SouzaNo ratings yet
- Benefits of Carrot JuiceDocument0 pagesBenefits of Carrot JuiceeQualizerNo ratings yet
- Natural Medicines Used in The Traditional Chinese Medical System For Therapy of Diabetes MellitusDocument21 pagesNatural Medicines Used in The Traditional Chinese Medical System For Therapy of Diabetes MellitusparibashaiNo ratings yet
- International Nursing Conference Abstracts - AINEC 2018Document42 pagesInternational Nursing Conference Abstracts - AINEC 2018Rika Fatmadona100% (1)
- Insulin Therapy in Type 1 Diabetes UpdateDocument83 pagesInsulin Therapy in Type 1 Diabetes UpdateasupicuNo ratings yet
- Diabetic NephropathyDocument7 pagesDiabetic NephropathyPlot BUnniesNo ratings yet
- Form 4 - Graphic Stimuli and Short TextsDocument3 pagesForm 4 - Graphic Stimuli and Short TextsRupert Quentin William Kingston PNo ratings yet
- Change Management in ActionDocument28 pagesChange Management in Actionsikkim blossomsNo ratings yet
- Interactive Patient Case Management #1Document33 pagesInteractive Patient Case Management #1Luzman HizrianNo ratings yet
- 2015 March 11 Peanut ReviewDocument28 pages2015 March 11 Peanut ReviewEmmanuel AbonNo ratings yet
- Laboratory Tests To Evaluate Fluid StatusDocument52 pagesLaboratory Tests To Evaluate Fluid StatusLester Exconde Alfonso0% (1)
- Katie Humphrey-Freedom From PCOS-lulu - Com (2010)Document131 pagesKatie Humphrey-Freedom From PCOS-lulu - Com (2010)Patricia ReynosoNo ratings yet