You might also like
- CDC Lab 2016 - Hepatitis Testing A-EDocument8 pagesCDC Lab 2016 - Hepatitis Testing A-ERobert G. Gish, MDNo ratings yet
- Hepatitis C Virus As A Systemic Disease: Reaching Beyong The LiverDocument9 pagesHepatitis C Virus As A Systemic Disease: Reaching Beyong The LiverRobert G. Gish, MDNo ratings yet
- Cost of Curing HCVDocument36 pagesCost of Curing HCVRobert G. Gish, MDNo ratings yet
- Stanford Clinic in San FranciscoDocument1 pageStanford Clinic in San FranciscoRobert G. Gish, MDNo ratings yet
- Presentation: SOTA 2015Document140 pagesPresentation: SOTA 2015Robert G. Gish, MDNo ratings yet
- Letter To MHPA Jeff MyersDocument4 pagesLetter To MHPA Jeff MyersRobert G. Gish, MDNo ratings yet
- Cost Effectiveness and Budget Impact of Treating HCVDocument12 pagesCost Effectiveness and Budget Impact of Treating HCVRobert G. Gish, MDNo ratings yet
- Stanford Clinic in SacramentoDocument1 pageStanford Clinic in SacramentoRobert G. Gish, MDNo ratings yet
- Hepatitis C Rallies in San FranciscoDocument1 pageHepatitis C Rallies in San FranciscoRobert G. Gish, MDNo ratings yet
- Centers For Medicare & Medicaid Services Letter To StatesDocument4 pagesCenters For Medicare & Medicaid Services Letter To StatesRobert G. Gish, MDNo ratings yet
- Hepatitis C Policy California MedicaidDocument4 pagesHepatitis C Policy California MedicaidRobert G. Gish, MDNo ratings yet
- CME Conference: Hepatitis C From A To ZDocument2 pagesCME Conference: Hepatitis C From A To ZRobert G. Gish, MDNo ratings yet
- Event: BEYOND THE WALLS OF THE CLINICDocument1 pageEvent: BEYOND THE WALLS OF THE CLINICRobert G. Gish, MDNo ratings yet
- Article: Hepatology - Prevalence of Chronic HBV and HCVDocument3 pagesArticle: Hepatology - Prevalence of Chronic HBV and HCVRobert G. Gish, MDNo ratings yet
- Presentation at The 2015 Liver SummitDocument211 pagesPresentation at The 2015 Liver SummitRobert G. Gish, MDNo ratings yet
- Dr. Gish LectureDocument1 pageDr. Gish LectureRobert G. Gish, MDNo ratings yet
- Message From CEVHAPDocument2 pagesMessage From CEVHAPRobert G. Gish, MDNo ratings yet
- Conference: Focus On The Hepatitis B VirusDocument52 pagesConference: Focus On The Hepatitis B VirusRobert G. Gish, MDNo ratings yet
- HCV Policy Presentation 2015Document18 pagesHCV Policy Presentation 2015Robert G. Gish, MDNo ratings yet
- Changing Nomenclature For PBC: From Cirrhosis' To Cholangitis'Document3 pagesChanging Nomenclature For PBC: From Cirrhosis' To Cholangitis'Robert G. Gish, MDNo ratings yet
- CEVHAP Membership Application FormDocument1 pageCEVHAP Membership Application FormRobert G. Gish, MDNo ratings yet
- Article in The Journal of Medical Practice ManagementDocument5 pagesArticle in The Journal of Medical Practice ManagementRobert G. Gish, MDNo ratings yet
- CEVHAP PamphletDocument2 pagesCEVHAP PamphletRobert G. Gish, MDNo ratings yet
- The Hepatitis C Education and Support Group Assistance ProgramDocument1 pageThe Hepatitis C Education and Support Group Assistance ProgramRobert G. Gish, MDNo ratings yet
- Gish - Et - Al-2015-Hepatology HBV HCV New EstimatesDocument8 pagesGish - Et - Al-2015-Hepatology HBV HCV New EstimatesRobert G. Gish, MDNo ratings yet
- Advisory Letter 2015Document1 pageAdvisory Letter 2015Robert G. Gish, MDNo ratings yet
- Abnormal Liver Tests PresentationDocument63 pagesAbnormal Liver Tests PresentationRobert G. Gish, MD100% (1)
- Gish - Et - Al-2015-Hepatology HBV HCV New EstimatesDocument8 pagesGish - Et - Al-2015-Hepatology HBV HCV New EstimatesRobert G. Gish, MDNo ratings yet
- Press ReleaseDocument3 pagesPress ReleaseRobert G. Gish, MDNo ratings yet
- Final Comments On Medicaid MCO Proposed RuleDocument8 pagesFinal Comments On Medicaid MCO Proposed RuleRobert G. Gish, MDNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5784)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (72)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- K To 12 Nail Care Learning ModuleDocument124 pagesK To 12 Nail Care Learning ModuleHari Ng Sablay92% (97)
- Math1 Q1 Week4 Day2Document7 pagesMath1 Q1 Week4 Day2Mariel Jane IgnaligNo ratings yet
- Lesson Plan EnglishDocument4 pagesLesson Plan EnglishMyra Janairo PalabricaNo ratings yet
- Lesson 2 Values 2 PrelimDocument12 pagesLesson 2 Values 2 Prelimbenny de castroNo ratings yet
- STUDENT FORM-Visa VarunDocument2 pagesSTUDENT FORM-Visa VarunSTUBBORN GAMINGNo ratings yet
- Resurse ProgramareDocument3 pagesResurse ProgramareManase RomeoNo ratings yet
- Earn EASA Part-66 Aircraft Maintenance Licence OnlineDocument4 pagesEarn EASA Part-66 Aircraft Maintenance Licence Onlinetotololo78100% (1)
- Gallup Action Plan For Apex HRDDocument7 pagesGallup Action Plan For Apex HRDshankhashuvraNo ratings yet
- Penulisan Rujukan Mengikut Format Apa Contoh PDFDocument16 pagesPenulisan Rujukan Mengikut Format Apa Contoh PDFzatty kimNo ratings yet
- Work Holiday Pass Application FormDocument4 pagesWork Holiday Pass Application FormAmir SaifuddinNo ratings yet
- Genesee County Interagency Scholarship ApplicationsDocument6 pagesGenesee County Interagency Scholarship ApplicationsWatertown Daily TimesNo ratings yet
- Learning SkillsDocument23 pagesLearning SkillsDr. J. Josephine JACNo ratings yet
- Reviste UMF INDEXATE Isi, Sisi, B+Document3 pagesReviste UMF INDEXATE Isi, Sisi, B+Alina AlinaNo ratings yet
- CV 1Document5 pagesCV 1api-313992212No ratings yet
- SACAP/R0001 Application For Registration As CandidateDocument8 pagesSACAP/R0001 Application For Registration As CandidateThomas Van DeventerNo ratings yet
- Get Outdoors with Family Nature ClubsDocument24 pagesGet Outdoors with Family Nature ClubsNana KawaiiNo ratings yet
- Design brief drives 3D productDocument8 pagesDesign brief drives 3D productCésar MartinsNo ratings yet
- MawallaDocument77 pagesMawallaAgustino WaitihacheNo ratings yet
- Ashu C VDocument3 pagesAshu C VashutoshbalkiNo ratings yet
- Cambridge First Certiíicate in EnglishDocument169 pagesCambridge First Certiíicate in EnglishAL OMNo ratings yet
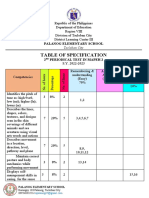
- 2nd Periodical Test in MAPEH 2 ReviewDocument7 pages2nd Periodical Test in MAPEH 2 ReviewJeffNo ratings yet
- Silent Film AssignmentDocument2 pagesSilent Film Assignmentapi-248112013100% (1)
- Econ Exam 1Document3 pagesEcon Exam 1vadarsuperstarNo ratings yet
- An Elegy For TheoryDocument2 pagesAn Elegy For TheoryB RhieNo ratings yet
- New Media 11 Course OutlineDocument3 pagesNew Media 11 Course Outlineapi-319035408No ratings yet
- Career Objective: - Ashok Leyland R&D, Chennai. Project Details: - TOPIC: - Bolted JointsDocument2 pagesCareer Objective: - Ashok Leyland R&D, Chennai. Project Details: - TOPIC: - Bolted JointsVikash JhaNo ratings yet
- O-Level English Essays 1 PDFDocument8 pagesO-Level English Essays 1 PDFAzra NaveedNo ratings yet
- Grade 7 Pre-Algebra SyllabusDocument2 pagesGrade 7 Pre-Algebra Syllabuspatricia.maia8301No ratings yet
- The Lakeville Journal - January 16, 2020Document14 pagesThe Lakeville Journal - January 16, 2020Lakeville Journal0% (1)
- English Form 1 Textbook CoverDocument2 pagesEnglish Form 1 Textbook Coverwan shadiawatie Wawan0% (1)