You might also like
- HIRARC 2 - Hazard Classification Hazard CategoryDocument77 pagesHIRARC 2 - Hazard Classification Hazard CategorySASHI NAIR100% (1)
- Occupational Health Hazards and Workers' Health: Marissa G. Lomuntad - San Jose, MD, MOHDocument86 pagesOccupational Health Hazards and Workers' Health: Marissa G. Lomuntad - San Jose, MD, MOHAviects Avie JaroNo ratings yet
- Fitness For WorkDocument13 pagesFitness For WorkPABLO HUGO CEVALLOS ALEGRIANo ratings yet
- Why businesses should be run ethicallyDocument8 pagesWhy businesses should be run ethicallysoniNo ratings yet
- Manual HandlingDocument18 pagesManual HandlingKarthikeyan Ramasamy100% (1)
- First Aid and Wound Care2Document24 pagesFirst Aid and Wound Care2Clowitzky IsikNo ratings yet
- Fitness For Work PolicyDocument2 pagesFitness For Work Policyjaultry muhuyiNo ratings yet
- Nursing in Occupational HealthDocument7 pagesNursing in Occupational HealthjorgeacctNo ratings yet
- Hirarc SharpDocument29 pagesHirarc Sharpczhong16No ratings yet
- Health and Safety Management in HealthcareDocument6 pagesHealth and Safety Management in HealthcareDr.ManageNo ratings yet
- GL Medic Surv 2001 PDFDocument139 pagesGL Medic Surv 2001 PDFAlief AzizNo ratings yet
- Worksite Hazard Analysis: Presented By: Thomas Dean Georgia TechDocument113 pagesWorksite Hazard Analysis: Presented By: Thomas Dean Georgia TechsahibjotNo ratings yet
- Accident Investigation ReportDocument2 pagesAccident Investigation ReportMichael MiotkNo ratings yet
- Ohsms Awareness & Implementation For ContractorsDocument24 pagesOhsms Awareness & Implementation For ContractorsFadzlli AminNo ratings yet
- 11 Ergonomics in OshDocument9 pages11 Ergonomics in OshMUHAMMAD ASIMNo ratings yet
- Occupational Health and Safety EssentialsDocument51 pagesOccupational Health and Safety EssentialsChloe Olazo100% (1)
- HirarcDocument21 pagesHirarcSaravanan SukumaranNo ratings yet
- Ergonomics: Steps in Deveoping An Ergonomic ProgramDocument4 pagesErgonomics: Steps in Deveoping An Ergonomic ProgramnellramosNo ratings yet
- Ergonomics Risk Assessment PDFDocument2 pagesErgonomics Risk Assessment PDFVictoriaNo ratings yet
- Protocol For Needle Stick Injur1Document1 pageProtocol For Needle Stick Injur1Prem KumarNo ratings yet
- OSHA ManagementDocument9 pagesOSHA ManagementAhmad Wafiuddin100% (1)
- Heat StressDocument10 pagesHeat StressMirza Ibrahim Ali BaigNo ratings yet
- Occupational Health HazardsDocument9 pagesOccupational Health HazardsAswin Magesh100% (1)
- C&C-EHS-P-017 Legal and Other RequirementDocument17 pagesC&C-EHS-P-017 Legal and Other RequirementNajman HamdiNo ratings yet
- Pre-Employment Medical ExaminationDocument4 pagesPre-Employment Medical ExaminationRohit Chaudhary100% (1)
- Medical History and Evaluation FormDocument22 pagesMedical History and Evaluation FormJobelle Fernandez-SantosNo ratings yet
- SOP First Aid TrainingDocument4 pagesSOP First Aid TrainingshreyasNo ratings yet
- Environmental Waste RecyclingDocument10 pagesEnvironmental Waste RecyclingFariq 'BoBo' AzahaNo ratings yet
- Unit-1 Introduction To Occupational Health and SafetyDocument31 pagesUnit-1 Introduction To Occupational Health and SafetysekinNo ratings yet
- Complete Safe@Work General Module TestDocument5 pagesComplete Safe@Work General Module TestcammcbeanNo ratings yet
- Musculoskeletal SystemDocument60 pagesMusculoskeletal Systempetite_chien15No ratings yet
- Report GroupDocument7 pagesReport Groupshafra_zulNo ratings yet
- 13 Needle-Stick InjuriesDocument9 pages13 Needle-Stick InjuriesveraNo ratings yet
- MANUAL HANDLING TILE: Understanding the Regulations and Assessment ToolDocument3 pagesMANUAL HANDLING TILE: Understanding the Regulations and Assessment ToolMuhammad AliNo ratings yet
- GC Risk Assessment 1Document2 pagesGC Risk Assessment 1api-464221711No ratings yet
- OSH-MS Guide to Malaysian Standard 1722Document6 pagesOSH-MS Guide to Malaysian Standard 1722Emiliana BrendaNo ratings yet
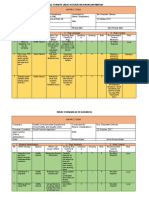
- Hirarc Form: Hirac Form Pejabat Kesihatan Bahagian MukahDocument4 pagesHirarc Form: Hirac Form Pejabat Kesihatan Bahagian MukahIGD RSIISNo ratings yet
- Medical Surveillance: Dr. I.B Adiatmaja Occupational Health - HSSE CorporateDocument22 pagesMedical Surveillance: Dr. I.B Adiatmaja Occupational Health - HSSE CorporateAlwin Anno SastraNo ratings yet
- 1 Introduction To Safety EngineeringDocument5 pages1 Introduction To Safety EngineeringMANNNo ratings yet
- Standard For Old Age PDFDocument65 pagesStandard For Old Age PDFRendani VeleNo ratings yet
- Risk Assessment of OH HazardsDocument21 pagesRisk Assessment of OH HazardsAntonio Jose De Jesus100% (2)
- Safety Education and TrainingDocument40 pagesSafety Education and Trainingkevin punzalan100% (4)
- Guidelines On Hearing Conservation ProgrammeDocument58 pagesGuidelines On Hearing Conservation ProgrammeTammanurRaviNo ratings yet
- DR Azrul Rozaiman Dato HJ Abdullah - An-Nur Specialist HospitalDocument22 pagesDR Azrul Rozaiman Dato HJ Abdullah - An-Nur Specialist Hospitalakubestlah100% (1)
- The Athletic Health Care TeamDocument52 pagesThe Athletic Health Care Teammupt77100% (1)
- Adroz Paramedic Resources Course Schedule: MonthDocument3 pagesAdroz Paramedic Resources Course Schedule: MonthHse Consultancy SgsbNo ratings yet
- Periodic Health ExaminationDocument38 pagesPeriodic Health ExaminationHilma NadhifaNo ratings yet
- Ergonomic HazardsDocument3 pagesErgonomic Hazardsshawalina07No ratings yet
- Ergonomics AssignmentDocument29 pagesErgonomics AssignmentRaja LutfiNo ratings yet
- Application Occupational Safety and Health in IndustryDocument24 pagesApplication Occupational Safety and Health in IndustryVRAM003100% (1)
- Occupational DiseasesDocument29 pagesOccupational DiseasesSubham GattaniNo ratings yet
- Crush Injury of Hand PDFDocument22 pagesCrush Injury of Hand PDFmilananand0% (1)
- Sample Ergonomics Program PDFDocument18 pagesSample Ergonomics Program PDFSyv Consultores AsociadosNo ratings yet
- Assignment-Xbcs3103 (J)Document22 pagesAssignment-Xbcs3103 (J)krubanNo ratings yet
- First Aid Plan ConstructionDocument13 pagesFirst Aid Plan ConstructionUmair KhanNo ratings yet
- Occupational Dermatitis in IndonesiaDocument30 pagesOccupational Dermatitis in IndonesiaAlfina MeidinaNo ratings yet
- ADD Packet With Vanderbilt AssessmentsDocument17 pagesADD Packet With Vanderbilt AssessmentsSundar PrabhuNo ratings yet
- Pediatric Intake Form SampleDocument10 pagesPediatric Intake Form SampleТравма ЮніверсумNo ratings yet
- Breathwork Interview FormDocument14 pagesBreathwork Interview FormAngelo TsakalosNo ratings yet
- Housing Application OHIC 2011Document1 pageHousing Application OHIC 2011Open Hearts Int'l EducationNo ratings yet
- Principles of Research Ethics: Prepared By: Assist. Prof. Dr. Yassin A. AsaadDocument19 pagesPrinciples of Research Ethics: Prepared By: Assist. Prof. Dr. Yassin A. AsaadasdfsNo ratings yet
- Administering Intradermal Injection Skin TestDocument2 pagesAdministering Intradermal Injection Skin TestKrysstal GerongaNo ratings yet
- Edu Adhd PaperDocument8 pagesEdu Adhd Paperapi-534406008No ratings yet
- Checklist For Persons Under Monitoring (PUM) : Eastern VisayasDocument1 pageChecklist For Persons Under Monitoring (PUM) : Eastern VisayasSophie Rose V R-zNo ratings yet
- ULIN 30 Agustus English Laporan PagiDocument15 pagesULIN 30 Agustus English Laporan PagiAhmad FachrurroziNo ratings yet
- PHCmanual 2010Document359 pagesPHCmanual 2010primaryhcNo ratings yet
- Legal Medicine ReviewerDocument13 pagesLegal Medicine ReviewerJernel Janz100% (1)
- Depression Report LayardDocument16 pagesDepression Report LayardwilliamNo ratings yet
- Prosecuting Medicaid Fraud in Texas: Senate Finance Sub-Committee On Medicaid February 15, 2011Document18 pagesProsecuting Medicaid Fraud in Texas: Senate Finance Sub-Committee On Medicaid February 15, 2011GovtfraudlawyerNo ratings yet
- 一个医学叛逆者的自白 CONFESSION OF A MEDICAL HERETICDocument106 pages一个医学叛逆者的自白 CONFESSION OF A MEDICAL HERETICAllan Zhang100% (1)
- Safe Injection Practices ChecklistDocument8 pagesSafe Injection Practices ChecklistrifkizidnyNo ratings yet
- Opioid Conversion Chart 2020 1Document1 pageOpioid Conversion Chart 2020 1aengus42No ratings yet
- Bindiya SIPDocument50 pagesBindiya SIPSukruti SakardeNo ratings yet
- Duty Doctors.Document3 pagesDuty Doctors.sankum7578No ratings yet
- Drug Proving Is The Systematic Process of Acquiring Knowledge of The Instruments Intended For The Cure ofDocument4 pagesDrug Proving Is The Systematic Process of Acquiring Knowledge of The Instruments Intended For The Cure ofKamal PatidarNo ratings yet
- 2ndgfmd Report PDFDocument236 pages2ndgfmd Report PDFSAURABH KUMARNo ratings yet
- Relational Coordination: An Exploration of Nursing Units, An Emergency Department and In-Patient TransfersDocument108 pagesRelational Coordination: An Exploration of Nursing Units, An Emergency Department and In-Patient TransferssaqibshahzadNo ratings yet
- Pontics: Vaishakhi .Y. Baisane (Ivth Year B.D.S) Vaishakhi .Y. Baisane (Ivth Year B.D.S)Document34 pagesPontics: Vaishakhi .Y. Baisane (Ivth Year B.D.S) Vaishakhi .Y. Baisane (Ivth Year B.D.S)Vaishakhi Baisane100% (1)
- Health Declaration FormDocument1 pageHealth Declaration FormWateen DataNocNo ratings yet
- 2016) - The Definition, Diagnostic Testing, and Management of Chronic Inducible Urticarias-The EAACIGA 2 LENEDFUNEV Consensus Recommendations 2016 Update and Revision.Document23 pages2016) - The Definition, Diagnostic Testing, and Management of Chronic Inducible Urticarias-The EAACIGA 2 LENEDFUNEV Consensus Recommendations 2016 Update and Revision.elçinNo ratings yet
- Planet Health - Ratail Marketing CaseDocument44 pagesPlanet Health - Ratail Marketing CaseSrinivasan Chandrasekar80% (5)
- Pharmacy DC Pharmacy Laws and RegulationsDocument430 pagesPharmacy DC Pharmacy Laws and RegulationsTanganGondrongNo ratings yet
- To MS DHQ THQs MIMS Training ScheduleDocument4 pagesTo MS DHQ THQs MIMS Training Schedulesunnykhan bwnNo ratings yet
- 28 April - 1 MEI 2021: Enhancing Patient's Experience in Urogynecology ServicesDocument10 pages28 April - 1 MEI 2021: Enhancing Patient's Experience in Urogynecology ServicesUNS KAMERA BELAKANGNo ratings yet
- Hipofarings PDFDocument10 pagesHipofarings PDFChad CarneyNo ratings yet
- QPMC Liph 2019Document69 pagesQPMC Liph 2019JovelleAnneMondragonNo ratings yet
- Death Obituary Ylrso PDFDocument10 pagesDeath Obituary Ylrso PDFAbbottTerkelsen7No ratings yet
- Rubric On Psyche CaseDocument3 pagesRubric On Psyche CaseJAN MARIELLE GALLARDENo ratings yet
- 21st Edition ALARM Manual 2014Document906 pages21st Edition ALARM Manual 2014dubblewalkerNo ratings yet
- First Aid and Water Survival 1st Exam CoverageDocument13 pagesFirst Aid and Water Survival 1st Exam CoverageNESIL PADASNo ratings yet