You might also like
- GERDDocument17 pagesGERDIntan AnanthaNo ratings yet
- Original ArticleDocument7 pagesOriginal ArticleIntan AnanthaNo ratings yet
- JurnalDocument1 pageJurnalIntan AnanthaNo ratings yet
- An+alternative+therapy+for+drug Resistant+epilepsy:+transcutaneous+auricular+vagus+nerve+stimulationDocument5 pagesAn+alternative+therapy+for+drug Resistant+epilepsy:+transcutaneous+auricular+vagus+nerve+stimulationIntan AnanthaNo ratings yet
- Electroacupuncture Accelerates Solid Gastric Emptying and Improves Dyspeptic Symptoms in Patients With Functional DyspepsiaDocument7 pagesElectroacupuncture Accelerates Solid Gastric Emptying and Improves Dyspeptic Symptoms in Patients With Functional DyspepsiaIntan AnanthaNo ratings yet
- Pharmacology & Therapeutics: Anders LehmannDocument7 pagesPharmacology & Therapeutics: Anders LehmannIntan AnanthaNo ratings yet
- R121 FullDocument11 pagesR121 FullIntan AnanthaNo ratings yet
- Volume 9, Issue 1, April 2008 - Gastroesophageal Reflux Disease in ObesityDocument6 pagesVolume 9, Issue 1, April 2008 - Gastroesophageal Reflux Disease in ObesityIntan AnanthaNo ratings yet
- 1 s2.0 S1525505013005489 MainDocument3 pages1 s2.0 S1525505013005489 MainIntan AnanthaNo ratings yet
- Volume 8, Issue 3, December 2007 - Pathophysiology Gastroesophageal Reflux DiseaseDocument7 pagesVolume 8, Issue 3, December 2007 - Pathophysiology Gastroesophageal Reflux DiseaseIntan AnanthaNo ratings yet
- Res Ieframe - DLL NavcanclDocument1 pageRes Ieframe - DLL NavcanclIntan AnanthaNo ratings yet
- Acupuncture Protected Cerebral Multi-Infarction Rats From Memory Impairment by Regulating The Expression of Apoptosis Related Genes Bcl-2 and Bax in Hippocampus.Document1 pageAcupuncture Protected Cerebral Multi-Infarction Rats From Memory Impairment by Regulating The Expression of Apoptosis Related Genes Bcl-2 and Bax in Hippocampus.Intan AnanthaNo ratings yet
- Acupuncture Protected Cerebral Multi-Infarction Rats From Memory Impairment by Regulating The Expression of Apoptosis Related Genes Bcl-2 and Bax in Hippocampus.Document1 pageAcupuncture Protected Cerebral Multi-Infarction Rats From Memory Impairment by Regulating The Expression of Apoptosis Related Genes Bcl-2 and Bax in Hippocampus.Intan AnanthaNo ratings yet
- Acupuncture in The Treatment ofDocument9 pagesAcupuncture in The Treatment ofIntan AnanthaNo ratings yet
- Biomarkers of Oxidative Stress in Vascular Dementia PatientsDocument2 pagesBiomarkers of Oxidative Stress in Vascular Dementia PatientsIntan AnanthaNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5783)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (72)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Field of NROSDocument3 pagesThe Field of NROSXavier de lucaNo ratings yet
- Lect 3 Trauma CounsellingDocument28 pagesLect 3 Trauma Counsellingumibrahim75% (8)
- Vibrant Blue Beginner Guide To Essential OilsDocument11 pagesVibrant Blue Beginner Guide To Essential OilsTonnie RostelliNo ratings yet
- Eye Exercises For Healthy Eye: September 2015Document3 pagesEye Exercises For Healthy Eye: September 2015spiridon_andrei2011No ratings yet
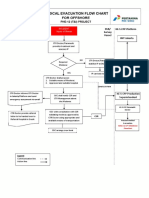
- 3-A4 - Medical Evacuation Flow Chart (Rev.0)Document1 page3-A4 - Medical Evacuation Flow Chart (Rev.0)SiskaNo ratings yet
- 4 ConceptDocument1 page4 ConceptStacey GarciaNo ratings yet
- SinusitisDocument12 pagesSinusitis05-NH-HU-KEVIN JULIO HUAYLLANE SOLISNo ratings yet
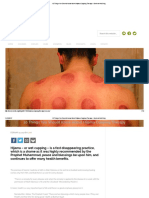
- HijamaDocument10 pagesHijamaGendale Am-isNo ratings yet
- Bio OssDocument4 pagesBio OssVizi AdrianNo ratings yet
- Fractional CO2 Laser Effective for Treating OnychomycosisDocument8 pagesFractional CO2 Laser Effective for Treating OnychomycosismyztNo ratings yet
- Social and Emotional Well Being Framework 2004-2009Document79 pagesSocial and Emotional Well Being Framework 2004-2009MikeJacksonNo ratings yet
- Effectiveness of Failure Modes Effect Analysis (FMEA) To Reduce Medical ErrorDocument5 pagesEffectiveness of Failure Modes Effect Analysis (FMEA) To Reduce Medical ErrorasiyahNo ratings yet
- Breast MassDocument38 pagesBreast MassLester Paul SivilaNo ratings yet
- Cci 300 Na enDocument9 pagesCci 300 Na enSrinivasan Jegan100% (1)
- Compulsive Sexual Behavior Compulsive Sexual Behavior Compulsive Sexual BehaviorDocument3 pagesCompulsive Sexual Behavior Compulsive Sexual Behavior Compulsive Sexual BehaviorAnand KirtiNo ratings yet
- DNC 2Document6 pagesDNC 2Maria VisitacionNo ratings yet
- Correction of Anterior Crossbite with Removable AppliancesDocument3 pagesCorrection of Anterior Crossbite with Removable Applianceschic organizer100% (1)
- Adlerian Therapy Written ReportDocument3 pagesAdlerian Therapy Written ReportEl Jhonna Duyag-MamaNo ratings yet
- Ijoto2016 4817429Document6 pagesIjoto2016 4817429Devi Arnes SimanjuntakNo ratings yet
- Can Mushrooms Really Save The World?Document26 pagesCan Mushrooms Really Save The World?ArabellaNo ratings yet
- Mother and Child Case StudyDocument18 pagesMother and Child Case StudyAlthea Mchanes100% (2)
- Urin The Miracle DrugDocument2 pagesUrin The Miracle DrugDina Malisa Nugraha, MDNo ratings yet
- Water Supply and Sanitary Engineering by Chittaranjan Bibhar 2cfa37 PDFDocument115 pagesWater Supply and Sanitary Engineering by Chittaranjan Bibhar 2cfa37 PDFRahul TomarNo ratings yet
- AMC Recalls 2014Document99 pagesAMC Recalls 2014saleema1175% (4)
- Parkinson DiseaseDocument9 pagesParkinson DiseaseMarco GunawanNo ratings yet
- Drug Price List Updated May 2016Document636 pagesDrug Price List Updated May 2016shajbabyNo ratings yet
- Myasthenia Gravis (MG) : AnatomyDocument12 pagesMyasthenia Gravis (MG) : AnatomyCici Novelia ManurungNo ratings yet
- General Psychology: A DefinitionDocument128 pagesGeneral Psychology: A DefinitionPaul Vincent GalgoNo ratings yet
- CGHS Rates 2014 - Jaipur3Document26 pagesCGHS Rates 2014 - Jaipur3YogendraNo ratings yet
- DOC461 Rev C-Laparoscopic UrologyDocument12 pagesDOC461 Rev C-Laparoscopic UrologyMI Kol EuanNo ratings yet