You might also like
- ASIA WorksheetDocument2 pagesASIA WorksheetDinar Yudistira FirdausNo ratings yet
- Asia Chart IscosDocument2 pagesAsia Chart IscosJeremiah HiiNo ratings yet
- Muscle Function and ASIA Impairment Scale DefinitionsDocument2 pagesMuscle Function and ASIA Impairment Scale DefinitionsIqbal BaryarNo ratings yet
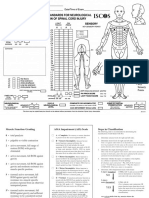
- F0826 International Standards For Neurological Classification of SCI Worksheet HGHDGDocument25 pagesF0826 International Standards For Neurological Classification of SCI Worksheet HGHDGreeves_cool100% (1)
- Asia Score For Vertebra InjuryDocument2 pagesAsia Score For Vertebra InjuryAzwin Kamar100% (1)
- Isncsci Exam Sheet r4Document2 pagesIsncsci Exam Sheet r4akhmadukiNo ratings yet
- Isncsci Asia Iscos LowDocument2 pagesIsncsci Asia Iscos LowmanuelmayoralNo ratings yet
- ASIA Scoring CardDocument2 pagesASIA Scoring CardSomu VictorNo ratings yet
- SEnSORY MOTOR TESTDocument4 pagesSEnSORY MOTOR TESTSergio Navarrete VidalNo ratings yet
- Spinal Cord Injury Assessment Chart (ASIA)Document2 pagesSpinal Cord Injury Assessment Chart (ASIA)cpradheep100% (5)
- ASIADocument2 pagesASIALuis Galván BastidasNo ratings yet
- ASPECTS score used to assess severity of MCA strokeDocument11 pagesASPECTS score used to assess severity of MCA strokeDiah Wardana100% (1)
- ASIA Impairment ScaleDocument10 pagesASIA Impairment Scaleazimahzainal211No ratings yet
- NIH Stroke ScaleDocument8 pagesNIH Stroke Scalepastizal123456No ratings yet
- Klasifikasi Dan Pengukuran ASIADocument8 pagesKlasifikasi Dan Pengukuran ASIAannisayaNo ratings yet
- 05-NIH Stroke ScaleDocument11 pages05-NIH Stroke ScaleMus TikaNo ratings yet
- NIHSSDocument15 pagesNIHSSganiaNo ratings yet
- NIHSSDocument1 pageNIHSSBobet Reña100% (1)
- Nih Stroke ScaleDocument15 pagesNih Stroke Scalemira ariantiNo ratings yet
- NIH Stroke ScaleDocument8 pagesNIH Stroke Scalesridhar100% (2)
- Thang điểm ASIADocument2 pagesThang điểm ASIADiệu My VươngNo ratings yet
- 0 Absent 1 Altered 2 Normal NT Not TestableDocument2 pages0 Absent 1 Altered 2 Normal NT Not Testablepablo lópezNo ratings yet
- NFL Sideline Concussion Assessment TestDocument2 pagesNFL Sideline Concussion Assessment TestRobert LeeNo ratings yet
- chapter-167Document14 pageschapter-167Cluster 1 2023No ratings yet
- Before Sig. (-) Findings. If Palpation Will Trigger 5x in PT., Perform This Test Last During The EvaluationDocument7 pagesBefore Sig. (-) Findings. If Palpation Will Trigger 5x in PT., Perform This Test Last During The Evaluationjoanna gurtizaNo ratings yet
- AT 3112 Lab 1Document6 pagesAT 3112 Lab 1Leigha DaryananiNo ratings yet
- Chapter 4B - Upper Extremity Post Stroke - 0Document22 pagesChapter 4B - Upper Extremity Post Stroke - 0Giga Hasabi AlkaraniNo ratings yet
- SCI Assessment: 5 Key ComponentsDocument24 pagesSCI Assessment: 5 Key ComponentsArslan AslamNo ratings yet
- Glasgow Coma Scale GCSDocument7 pagesGlasgow Coma Scale GCSSSNo ratings yet
- Muscle Testing 1Document39 pagesMuscle Testing 1Rana MubashirNo ratings yet
- Glasgow Coma Scale (GCS) Definition and Assessment of Eye Opening ResponseDocument3 pagesGlasgow Coma Scale (GCS) Definition and Assessment of Eye Opening ResponseLanie Reyes de Guzman0% (1)
- Asia ScaleDocument30 pagesAsia ScaleKavya MittalNo ratings yet
- Manual Muscle TestingDocument28 pagesManual Muscle TestingMuhammad UsmanNo ratings yet
- NFL Concussion Assessment ToolDocument2 pagesNFL Concussion Assessment ToolprotectthebrainNo ratings yet
- Pre-Participation Screening: The Use of Fundamental Movements As An Assessment of Function - Part 2Document8 pagesPre-Participation Screening: The Use of Fundamental Movements As An Assessment of Function - Part 2gogo36No ratings yet
- Neuro Assessment GzwartDocument27 pagesNeuro Assessment GzwartCharan Teja Reddy AvulaNo ratings yet
- Presentasi Nihss NeuroupdateDocument44 pagesPresentasi Nihss NeuroupdatenurdiansyahNo ratings yet
- Use of The NIH Stroke Scale: January 2008Document45 pagesUse of The NIH Stroke Scale: January 2008DewanggaWahyuPrajaNo ratings yet
- Glasgow Coma ScaleDocument4 pagesGlasgow Coma ScaleSajo KappanNo ratings yet
- ASIADocument2 pagesASIASandra GarciaNo ratings yet
- Calculation of GcsDocument5 pagesCalculation of GcsGerald Limo Arap ChebiiNo ratings yet
- Manual Muscle TestingDocument38 pagesManual Muscle TestingNada RonaldNo ratings yet
- Chap 2 Pengukuran Kekuatan OtotDocument64 pagesChap 2 Pengukuran Kekuatan OtottianNo ratings yet
- Abdominal Hollowing ExercisesDocument8 pagesAbdominal Hollowing ExercisesKinesiología TalganteNo ratings yet
- Practicum: MMT 9/13/2021/yfshihDocument6 pagesPracticum: MMT 9/13/2021/yfshihchiendy.yNo ratings yet
- Adhi Lakshmi (MMT)Document35 pagesAdhi Lakshmi (MMT)venkata ramakrishnaiahNo ratings yet
- AIS 2011 ResumeDocument7 pagesAIS 2011 Resumesani widya firnandaNo ratings yet
- Neuroathletics Training for Beginners More Coordination, Agility and Concentration Thanks to Improved Neuroathletics - Incl. 10-Week Plan For Training in Everyday Life.From EverandNeuroathletics Training for Beginners More Coordination, Agility and Concentration Thanks to Improved Neuroathletics - Incl. 10-Week Plan For Training in Everyday Life.No ratings yet
- Length Tension Testing Book 2, Upper Quadrant: A Workbook of Manual Therapy TechniquesFrom EverandLength Tension Testing Book 2, Upper Quadrant: A Workbook of Manual Therapy TechniquesRating: 1 out of 5 stars1/5 (1)
- Length Tension Testing Book 1, Lower Quadrant: A Workbook of Manual Therapy TechniquesFrom EverandLength Tension Testing Book 1, Lower Quadrant: A Workbook of Manual Therapy TechniquesRating: 3.5 out of 5 stars3.5/5 (3)
- Power Flex Stretching - Super Flexibility and Strength for peak performanceFrom EverandPower Flex Stretching - Super Flexibility and Strength for peak performanceRating: 3 out of 5 stars3/5 (3)
- Brain Breakthrough: The Art of Neurological Rehabilitation: Easy and Innovative Techniques, #1From EverandBrain Breakthrough: The Art of Neurological Rehabilitation: Easy and Innovative Techniques, #1No ratings yet
- Intraoperative Neurophysiological Monitoring in Hemifacial Spasm: A Practical GuideFrom EverandIntraoperative Neurophysiological Monitoring in Hemifacial Spasm: A Practical GuideNo ratings yet
- A Simple Guide to Post-stroke Recovery, Diagnosis, Treatment and Related ConditionsFrom EverandA Simple Guide to Post-stroke Recovery, Diagnosis, Treatment and Related ConditionsNo ratings yet
- The Whartons' Strength Book: Upper Body: Total Stability for Shoulders, Neck, Arm, Wrist, and ElbowFrom EverandThe Whartons' Strength Book: Upper Body: Total Stability for Shoulders, Neck, Arm, Wrist, and ElbowRating: 5 out of 5 stars5/5 (1)
- Do Not Give Up Your Favorite Sport For A Shoulder Dislocation !From EverandDo Not Give Up Your Favorite Sport For A Shoulder Dislocation !Rating: 1 out of 5 stars1/5 (1)
- J. Plankton Res. 2009 Yang 647 59Document13 pagesJ. Plankton Res. 2009 Yang 647 59mayones80No ratings yet
- 281 ProtozoanBiologicalIslandDocument8 pages281 ProtozoanBiologicalIslandmayones80No ratings yet
- Colorectal Carcinoma: Haryono YarmanDocument18 pagesColorectal Carcinoma: Haryono Yarmanmayones80No ratings yet
- Acute Stroke ManagementDocument22 pagesAcute Stroke ManagementE=MC2No ratings yet
- Grade 5 PPT English Q4 W3 Day 2Document17 pagesGrade 5 PPT English Q4 W3 Day 2Rommel MarianoNo ratings yet
- Service ManualDocument14 pagesService ManualOlegNo ratings yet
- Boast 98Document19 pagesBoast 98jghleivaNo ratings yet
- Dof Omm Ss Skirting Sk-02Document8 pagesDof Omm Ss Skirting Sk-02Ideal DesignerNo ratings yet
- Lahore School of Economics Operations Management Final Group Project Outline (Weightage 15%) Bba - Iv Instructor: Dr. Saba Fazal FirdousiDocument3 pagesLahore School of Economics Operations Management Final Group Project Outline (Weightage 15%) Bba - Iv Instructor: Dr. Saba Fazal FirdousiAshir HassanNo ratings yet
- What Is InterpolDocument5 pagesWhat Is InterpolJimmy Jr Comahig LapeNo ratings yet
- 1 Osteology (MCQ)Document12 pages1 Osteology (MCQ)Utkarsh MishraNo ratings yet
- Bank 12Document19 pagesBank 12Shivangi GuptaNo ratings yet
- Fundamental Powers of The State (Police Power) Ynot v. IAC Facts: Ermita Malate v. City of Manila 20 SCRA 849 (1967)Document18 pagesFundamental Powers of The State (Police Power) Ynot v. IAC Facts: Ermita Malate v. City of Manila 20 SCRA 849 (1967)Ella QuiNo ratings yet
- Science 7 Module1Document22 pagesScience 7 Module1Hector Panti0% (1)
- Markard Et Al. (2012) PDFDocument13 pagesMarkard Et Al. (2012) PDFgotrektomNo ratings yet
- Xbox - RGH E Ltu: Jogo 3.0 4.0 HD NºDocument11 pagesXbox - RGH E Ltu: Jogo 3.0 4.0 HD NºGabriel DinhaNo ratings yet
- The Minecraft Survival Quest ChallengeDocument4 pagesThe Minecraft Survival Quest Challengeapi-269630780100% (1)
- Activity7 Raptshia DataSetDocument16 pagesActivity7 Raptshia DataSetoneinamillionnamedlunaNo ratings yet
- Accenture Faq For New JoinersDocument4 pagesAccenture Faq For New JoinersBaazinow Hack Brainbaazi Live AnswersNo ratings yet
- The NF and BNF Charts from the Trading RoomDocument23 pagesThe NF and BNF Charts from the Trading RoomSinghRaviNo ratings yet
- Data Structure & Algorithms (TIU-UCS-T201) : Presented by Suvendu Chattaraj (Department of CSE, TIU, WB)Document23 pagesData Structure & Algorithms (TIU-UCS-T201) : Presented by Suvendu Chattaraj (Department of CSE, TIU, WB)Adhara MukherjeeNo ratings yet
- BLDG TECH Juson Assignment Lecture 1Document23 pagesBLDG TECH Juson Assignment Lecture 1Ma. Janelle GoNo ratings yet
- Gas Turbine MaintenanceDocument146 pagesGas Turbine MaintenanceMamoun1969100% (8)
- Tutorial Letter 101/3/2018: Internal Auditing: Theory & PrinciplesDocument39 pagesTutorial Letter 101/3/2018: Internal Auditing: Theory & PrinciplesSAMANTHANo ratings yet
- Vào 10 - Sở L NG Sơn 2022-2023Document5 pagesVào 10 - Sở L NG Sơn 2022-2023Lan HuongNo ratings yet
- Strategies and Methods For Cloud MigrationDocument10 pagesStrategies and Methods For Cloud MigrationVel_stNo ratings yet
- Micro810 Allen Bradley User ManualDocument120 pagesMicro810 Allen Bradley User ManualStefano MontiNo ratings yet
- Next-Generation Widebody Conversion: in Service From 2017 ONWARDSDocument6 pagesNext-Generation Widebody Conversion: in Service From 2017 ONWARDSAgusNo ratings yet
- ISO 22301 Mandatory DocumentDocument2 pagesISO 22301 Mandatory Documenttrackuse100% (1)
- User Interface Analysis and Design TrendsDocument38 pagesUser Interface Analysis and Design TrendsArbaz AliNo ratings yet
- Predict CambodianDocument11 pagesPredict CambodianMd Ibrahim KhalilNo ratings yet
- RMAN Backup and Recovery Strategies with Oracle DatabaseDocument26 pagesRMAN Backup and Recovery Strategies with Oracle DatabaseCristiano Vasconcelos BarbosaNo ratings yet
- TMP 841704 RL 2023-03-13 Relieving LetterDocument1 pageTMP 841704 RL 2023-03-13 Relieving Letterxop0887No ratings yet