You might also like
- 06 Process ReliabilityDocument12 pages06 Process ReliabilitySidney LinsNo ratings yet
- Kaizen - Esp02 221B4 DamperDocument4 pagesKaizen - Esp02 221B4 DamperRakesh Kumar Singh (Phase 1B)No ratings yet
- ENT 416-3-Engineering Design ProcessDocument31 pagesENT 416-3-Engineering Design ProcessRaghulNo ratings yet
- Switchyard Jishu Hozen Fugai SheetDocument8 pagesSwitchyard Jishu Hozen Fugai SheetAnonymous vcadX45TD7No ratings yet
- LINE FEEDING AND QUALITY INSPECTION PROCESSDocument12 pagesLINE FEEDING AND QUALITY INSPECTION PROCESSkvNo ratings yet
- MTPDocument10 pagesMTPmurilocabriniNo ratings yet
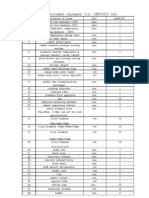
- Test Instrument Equipment List (Sepcoiii Lab)Document2 pagesTest Instrument Equipment List (Sepcoiii Lab)Kuldeep ChakerwartiNo ratings yet
- Rejection Analysis For January 2012: % Age Desending Order Cum. Total % RejDocument7 pagesRejection Analysis For January 2012: % Age Desending Order Cum. Total % RejazadNo ratings yet
- Estimating Measurement ComponentsDocument24 pagesEstimating Measurement ComponentsLuis ConstanteNo ratings yet
- Permanent Change and Temporary Deviation Request FormDocument1 pagePermanent Change and Temporary Deviation Request FormdrustagiNo ratings yet
- Process Improvement in Casting Through Defect Minimization A Case Study1 PDFDocument7 pagesProcess Improvement in Casting Through Defect Minimization A Case Study1 PDFTarun ChakrabortyNo ratings yet
- Xfmea Pfmea PDFDocument8 pagesXfmea Pfmea PDFvinidesoNo ratings yet
- Transportation LabDocument17 pagesTransportation LabIftikhar MughalNo ratings yet
- Agile Scrum at Glance BaselineDocument1 pageAgile Scrum at Glance BaselinedrustagiNo ratings yet
- Icam Related Event and Conditions ChartDocument3 pagesIcam Related Event and Conditions ChartJohn KalvinNo ratings yet
- Variation and DefectsDocument16 pagesVariation and DefectssushmaxNo ratings yet
- Indicators Performances Lafiguie Mars 2023Document1 pageIndicators Performances Lafiguie Mars 2023Yves Crescent AdonNo ratings yet
- Kaizen PF6Document10 pagesKaizen PF6Jeniffer RayenNo ratings yet
- Different Types of Time in ManufacturingDocument15 pagesDifferent Types of Time in ManufacturingkazuNo ratings yet
- Hydraulique BasesDocument165 pagesHydraulique BasesOTHMAN MCHACHTINo ratings yet
- Glowinkowski Customer Service Directors - Behavioural Competency FrameworkDocument12 pagesGlowinkowski Customer Service Directors - Behavioural Competency FrameworkitrejosNo ratings yet
- pure cotton pvt ltd final inspection reportDocument4 pagespure cotton pvt ltd final inspection reportTarun PariharNo ratings yet
- Risk Register Format Example March 2008Document1 pageRisk Register Format Example March 2008Tissa1969No ratings yet
- Final Report TPM PartDocument16 pagesFinal Report TPM PartNikita AwasthiNo ratings yet
- V Buehler Lean Assessment TemplateDocument22 pagesV Buehler Lean Assessment TemplatedrustagiNo ratings yet
- S-44 For DummiesDocument6 pagesS-44 For DummiesgokedaNo ratings yet
- Department Name: Production Department Name: Production: Material ResourcesDocument21 pagesDepartment Name: Production Department Name: Production: Material ResourcesLesly LesNo ratings yet
- Plant Loss Tree DataDocument1 pagePlant Loss Tree DataJoseph OrjiNo ratings yet
- Set Up TimeDocument23 pagesSet Up TimemuneerppNo ratings yet
- 8D ReportDocument2 pages8D Reportgatofelix1980100% (1)
- Quality Assurance SOP TemplateDocument3 pagesQuality Assurance SOP TemplateGAURAV SHARMANo ratings yet
- Corrective Action Board CABDocument28 pagesCorrective Action Board CABSudhagarNo ratings yet
- MTBF - MTTRDocument11 pagesMTBF - MTTRYogesh BadheNo ratings yet
- Defects Reduction in A Pump Manufacturing Industry Using Six Sigma MethodologiesDocument7 pagesDefects Reduction in A Pump Manufacturing Industry Using Six Sigma MethodologiesInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Daily Machine Production ReportDocument1 pageDaily Machine Production ReportimtiazNo ratings yet
- A3 Process Guide for Improving Patient TransportDocument14 pagesA3 Process Guide for Improving Patient TransportJayantRKNo ratings yet
- Customer Special CharacteristicsDocument1 pageCustomer Special Characteristicspundhir12898No ratings yet
- Short Interval Control (SIC)Document1 pageShort Interval Control (SIC)Samuel LambrechtNo ratings yet
- Equipment Rental Action PlanDocument3 pagesEquipment Rental Action PlanKenneth MedinaNo ratings yet
- MTTR and MTBFDocument4 pagesMTTR and MTBFchandrashekharNo ratings yet
- First Piece Apparoval Parameters MG & Motor LineDocument14 pagesFirst Piece Apparoval Parameters MG & Motor LineNeha SharmaNo ratings yet
- Short Interval Control Executive SummaryDocument2 pagesShort Interval Control Executive Summaryaminos85No ratings yet
- Machine Consistancy Test: INSTRUCTIONS - Print This Sheet and Gather Data, or Use This Spreadsheet at The PressDocument2 pagesMachine Consistancy Test: INSTRUCTIONS - Print This Sheet and Gather Data, or Use This Spreadsheet at The Pressm asifNo ratings yet
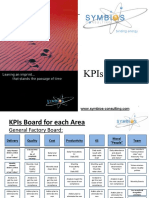
- KPIs boards optimize factory performanceDocument7 pagesKPIs boards optimize factory performanceAhmed HassanNo ratings yet
- An Approach to Dam Safety AssessmentDocument8 pagesAn Approach to Dam Safety AssessmentJavierNo ratings yet
- Production Management Scope and ObjectiveDocument19 pagesProduction Management Scope and ObjectiveBhushan Chinchmalatpure100% (6)
- Barotiwala Factory MFG Score Card 2019Document10 pagesBarotiwala Factory MFG Score Card 2019Ashish MishraNo ratings yet
- List of Production ReportsDocument12 pagesList of Production ReportsSangeeth BhoopaalanNo ratings yet
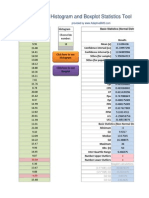
- Histogram Box Plot Statistics AdaptiveBMSDocument13 pagesHistogram Box Plot Statistics AdaptiveBMSashutoshrvNo ratings yet
- Commitment vs. Compliance: Ten Reasons Why You Need Your Workers' Hearts, Not Just Their HandsDocument6 pagesCommitment vs. Compliance: Ten Reasons Why You Need Your Workers' Hearts, Not Just Their HandsMac McIntireNo ratings yet
- Audit Plan: Auditee Eng/Support Top Management CCDocument16 pagesAudit Plan: Auditee Eng/Support Top Management CCRohit SoniNo ratings yet
- Clause Wise Tutorials-7.1.4 Change Control ExplanationDocument2 pagesClause Wise Tutorials-7.1.4 Change Control ExplanationBharathNo ratings yet
- History and Statistics of Different Maintenance StrategiesDocument23 pagesHistory and Statistics of Different Maintenance StrategiesRaj BoligorNo ratings yet
- TPM Pillar Basic Knowledge ImprovementDocument1 pageTPM Pillar Basic Knowledge ImprovementGiö GdlNo ratings yet
- Filter assembly line defect analysis and Pareto chart for February 2022Document2 pagesFilter assembly line defect analysis and Pareto chart for February 2022Iqbal singh DhanjalNo ratings yet
- Kaizen Report Sheet Template for Mechanical Engineering DepartmentDocument1 pageKaizen Report Sheet Template for Mechanical Engineering DepartmentSaravana VigneshNo ratings yet
- Defect Matrix AutosavedDocument23 pagesDefect Matrix AutosavedVikas KashyapNo ratings yet
- Application of Root Cause Analysis in Improvement of Product Quality & ProductivityDocument38 pagesApplication of Root Cause Analysis in Improvement of Product Quality & ProductivityZakNo ratings yet
- Application of Root Cause Analysis in Improvement of Product Quality and ProductivityDocument39 pagesApplication of Root Cause Analysis in Improvement of Product Quality and ProductivityMochammad TaufikNo ratings yet
- Root Cause Analysis: Ruksana Hamid, Medical Officer and Anesthesiologist, JK HealthDocument7 pagesRoot Cause Analysis: Ruksana Hamid, Medical Officer and Anesthesiologist, JK HealthAnar HajiyevNo ratings yet
- EMC TrendsDocument55 pagesEMC TrendsXiang LiuNo ratings yet
- FDA Guidance - Content of Premarket Submissions For Management of Cybersecurity in Medical Devices, Oct 2, 2014Document9 pagesFDA Guidance - Content of Premarket Submissions For Management of Cybersecurity in Medical Devices, Oct 2, 2014Xiang LiuNo ratings yet
- FDA Guidance Documents For Software Contained in Medical DevicesDocument23 pagesFDA Guidance Documents For Software Contained in Medical Deviceschance909100% (1)
- STEM Engineering CampsDocument2 pagesSTEM Engineering CampsXiang LiuNo ratings yet
- Review of The New Y14 5 2009 StandardDocument16 pagesReview of The New Y14 5 2009 StandardPhillip GrimNo ratings yet
- FDA Guidance - Cybersecurity For Networked Medical Devices Containing Off-The-Shelf (OTS) Software, Jan 14, 2005Document7 pagesFDA Guidance - Cybersecurity For Networked Medical Devices Containing Off-The-Shelf (OTS) Software, Jan 14, 2005Xiang LiuNo ratings yet
- FDA Guidance - Mobile Medical Applications - Sept 25, 2013Document43 pagesFDA Guidance - Mobile Medical Applications - Sept 25, 2013Xiang LiuNo ratings yet
- CLAD Sample Exam GuideDocument20 pagesCLAD Sample Exam GuideJie Wei100% (1)
- Mhealth App Developer Economics 2014Document43 pagesMhealth App Developer Economics 2014Xiang LiuNo ratings yet
- CLAD Sample Exam-2Document24 pagesCLAD Sample Exam-2Boda NingNo ratings yet
- Connector Design - Materials and Connector ReliabilityDocument16 pagesConnector Design - Materials and Connector ReliabilityXiang Liu100% (1)
- Labview Design PatternsDocument60 pagesLabview Design PatternsBruke OystenNo ratings yet
- 13F Internal Audit ChecklistDocument5 pages13F Internal Audit ChecklistXiang Liu0% (1)
- Autoclaving SOPDocument4 pagesAutoclaving SOPXiang LiuNo ratings yet
- On Testing Non-Testable ProgramsDocument6 pagesOn Testing Non-Testable ProgramsXiang LiuNo ratings yet
- 6 1standard WorkDocument15 pages6 1standard WorkXiang Liu100% (1)
- Sterile Product Package Integrity TestingDocument104 pagesSterile Product Package Integrity TestingJihad Elias ChahlaNo ratings yet
- Logo System Manual en-US en-USDocument286 pagesLogo System Manual en-US en-USmaobluffNo ratings yet
- Certification Handbook PDFDocument23 pagesCertification Handbook PDFMarvin ArinueloNo ratings yet
- Test Method Validation Case StudyDocument2 pagesTest Method Validation Case StudyXiang LiuNo ratings yet
- Intertek RoHS 2 Services BrochureDocument2 pagesIntertek RoHS 2 Services BrochureXiang LiuNo ratings yet
- LOGO! Modules GuideDocument3 pagesLOGO! Modules GuideJoseNo ratings yet
- ASQ Certification Program Gain Wider RecognitionDocument13 pagesASQ Certification Program Gain Wider RecognitionXiang LiuNo ratings yet
- Systems Engineering (SE) & Project Management: Nick Clemens, PMPDocument37 pagesSystems Engineering (SE) & Project Management: Nick Clemens, PMPcasakaNo ratings yet
- ASQ Certification Program Gain Wider RecognitionDocument13 pagesASQ Certification Program Gain Wider RecognitionXiang LiuNo ratings yet
- Universal Host Controller Interface (UHCI) Design GuideDocument47 pagesUniversal Host Controller Interface (UHCI) Design GuideXiang LiuNo ratings yet
- Certification Exam - Tips, Trips and TrapsDocument7 pagesCertification Exam - Tips, Trips and TrapsXiang LiuNo ratings yet
- Bsi Small Business Guide To Standards en GBDocument24 pagesBsi Small Business Guide To Standards en GBXiang LiuNo ratings yet
- Iso 9001 Self Assessment ChecklistDocument4 pagesIso 9001 Self Assessment ChecklistXiang LiuNo ratings yet
- Probing Technology With Technology ProbesDocument9 pagesProbing Technology With Technology ProbesdiamondoNo ratings yet
- Failure Mode Analysis (FMEA) Technique for Risk AssessmentDocument4 pagesFailure Mode Analysis (FMEA) Technique for Risk AssessmentJohn Robyn HernandezNo ratings yet
- Instruments: Washing Disinfection CatalogueDocument66 pagesInstruments: Washing Disinfection CatalogueGeoemilia1No ratings yet
- Systems DesignDocument21 pagesSystems DesignholocenicNo ratings yet
- Maintenance Inspection and Procedures for Aerospace EquipmentDocument102 pagesMaintenance Inspection and Procedures for Aerospace EquipmentDenny TerhaarNo ratings yet
- Russo 2007 - Improving The Reliability of GSI EstimationsDocument6 pagesRusso 2007 - Improving The Reliability of GSI EstimationsPauly FernándezNo ratings yet
- Quality Evaluation of Cardiac Decision Support Systems Using ISO 25010 StandardDocument8 pagesQuality Evaluation of Cardiac Decision Support Systems Using ISO 25010 StandardorionUPCNo ratings yet
- WalkthroughDocument4 pagesWalkthroughkangstasNo ratings yet
- Designating Special CharacteristicsDocument14 pagesDesignating Special CharacteristicsIoana AlexandraNo ratings yet
- NGT-1-USB Install ManualDocument12 pagesNGT-1-USB Install ManualminhtqNo ratings yet
- Suorineni 2012MassMinSudburyDocument9 pagesSuorineni 2012MassMinSudburyCindy MoralesNo ratings yet
- Daily Safety Task Instruction - SupervisorDocument25 pagesDaily Safety Task Instruction - SupervisorChristian Makande83% (18)
- Atkins HF Oil and Gas PDFDocument12 pagesAtkins HF Oil and Gas PDFDanny BoysieNo ratings yet
- WC77xx SW Install InstructionsDocument2 pagesWC77xx SW Install Instructionssuporte colorgrafixNo ratings yet
- PNR-000054 - Assessment of Management System and Results - Rev.08Document8 pagesPNR-000054 - Assessment of Management System and Results - Rev.08pertiwielsyaNo ratings yet
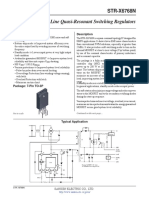
- str-x6768n Ds en PDFDocument9 pagesstr-x6768n Ds en PDFCarlNo ratings yet
- CS8494 Softwareengineering-Unit IiDocument69 pagesCS8494 Softwareengineering-Unit Iijohn8870No ratings yet
- QLD Manual For Assessing Consequence Categories and Hydraulic Performance of StructuresDocument34 pagesQLD Manual For Assessing Consequence Categories and Hydraulic Performance of StructuresShehan UdukumburageNo ratings yet
- Weibull 7 - TrainingDocument98 pagesWeibull 7 - TrainingKhalid MahmoodNo ratings yet
- Bath Tub CurveDocument13 pagesBath Tub CurveMd Arshad Alam100% (1)
- For Email Daily Thermetrics TSTC Product BrochureDocument5 pagesFor Email Daily Thermetrics TSTC Product BrochureIlkuNo ratings yet
- Practitioner Guide 0512 Inspection, Maintenance & Testing of Equipment Installed at PetroleumDocument88 pagesPractitioner Guide 0512 Inspection, Maintenance & Testing of Equipment Installed at PetroleumsusanwebNo ratings yet
- MTTR & MTBF Calculation in SAP PMDocument3 pagesMTTR & MTBF Calculation in SAP PMSaif Ali MominNo ratings yet
- CBM & RCM Applied On Nuclear Power PlantsDocument11 pagesCBM & RCM Applied On Nuclear Power PlantsGeert Henk WijnantsNo ratings yet
- IEEE STD 3006.2 - 2016: Power Systems ReliabilityDocument28 pagesIEEE STD 3006.2 - 2016: Power Systems ReliabilityYogesh MittalNo ratings yet
- Weibull AnalysisDocument2 pagesWeibull AnalysisSebastián D. GómezNo ratings yet
- Learn RCM: Correctly Reliability Centered Maintenance - RCMDocument1 pageLearn RCM: Correctly Reliability Centered Maintenance - RCMRaihan DanishNo ratings yet
- Evaluation of Power Substation Equipment PDFDocument16 pagesEvaluation of Power Substation Equipment PDFkayodeNo ratings yet
- Kuliah 5 - Project RiskDocument27 pagesKuliah 5 - Project RiskJULIAN ARISKY LASENo ratings yet
- Engine Health Monitoring Systems For Industrial Gas TurbinesDocument10 pagesEngine Health Monitoring Systems For Industrial Gas TurbinesAshwin ShindeNo ratings yet