You might also like
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (894)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- AAD Basic SkinDocument57 pagesAAD Basic SkinDevina HarsonoNo ratings yet
- Business Plan of Easy Meal ServiceDocument41 pagesBusiness Plan of Easy Meal ServiceCeddie UnggayNo ratings yet
- Surface Roughness Measurement - MitutoyoDocument2 pagesSurface Roughness Measurement - MitutoyoSelvaraj BalasundramNo ratings yet
- Schneider Power Supply PhaseoDocument26 pagesSchneider Power Supply PhaseoScott EnnisNo ratings yet
- Florence Nightingale: The Lady with the LampDocument18 pagesFlorence Nightingale: The Lady with the LampsrinivasanaNo ratings yet
- Analytical Methods To Measure The Constants of Fats and OilsDocument5 pagesAnalytical Methods To Measure The Constants of Fats and OilsPenicillium Notatum67% (3)
- Tribology - Lubricants and LubricationDocument330 pagesTribology - Lubricants and LubricationJosé Ramírez100% (2)
- Modeling of Soil-Structure Interaction as Finite Element Using SAP2000Document5 pagesModeling of Soil-Structure Interaction as Finite Element Using SAP2000Tariq MahmoodNo ratings yet
- 1 Classification of The AntibioticsDocument5 pages1 Classification of The AntibioticsMulia Sari Mu'minNo ratings yet
- Imaging Algorithm 498950893Document4 pagesImaging Algorithm 498950893Novi IrmalaNo ratings yet
- Skinandantioxidants PDFDocument8 pagesSkinandantioxidants PDFDevina HarsonoNo ratings yet
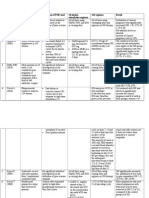
- No Study Study Design and Sample Size Definition of POR Used Ovulation Stimulation Regimen GH Regimen ResultDocument3 pagesNo Study Study Design and Sample Size Definition of POR Used Ovulation Stimulation Regimen GH Regimen ResultDevina HarsonoNo ratings yet
- Evaluating Infertility PDFDocument3 pagesEvaluating Infertility PDFJeff BakerNo ratings yet
- Allergic RhinitisDocument43 pagesAllergic RhinitisDevina HarsonoNo ratings yet
- Reindeer This Heart of MineDocument1 pageReindeer This Heart of MineNermine NasrNo ratings yet
- RCT Journal Propanolol For InfantDocument12 pagesRCT Journal Propanolol For InfantbenyinyisNo ratings yet
- JudulDocument88 pagesJudulPurna Adi PutraNo ratings yet
- TinitusDocument40 pagesTinitusDevina HarsonoNo ratings yet
- Aeiou Tips: Altered Mental StatusDocument13 pagesAeiou Tips: Altered Mental StatusDevina HarsonoNo ratings yet
- Sudden Hearing LossDocument35 pagesSudden Hearing LossDevina HarsonoNo ratings yet
- Adjuvant Growth Hormone For Ovulation Induction WithDocument3 pagesAdjuvant Growth Hormone For Ovulation Induction WithDevina HarsonoNo ratings yet
- Growth HormonDocument4 pagesGrowth HormonDevina HarsonoNo ratings yet
- Effect of Estrogen On Skin Aging and The Potential Role of SERMs PDFDocument16 pagesEffect of Estrogen On Skin Aging and The Potential Role of SERMs PDFDevina HarsonoNo ratings yet
- De 5 264Document7 pagesDe 5 264Devina HarsonoNo ratings yet
- 224 Expder-HormDocument5 pages224 Expder-HormDevina HarsonoNo ratings yet
- Effect of Estrogen On Skin Aging and The Potential Role of SERMs PDFDocument16 pagesEffect of Estrogen On Skin Aging and The Potential Role of SERMs PDFDevina HarsonoNo ratings yet
- De Ning A Poor Responder in IVF 2004Document3 pagesDe Ning A Poor Responder in IVF 2004Devina HarsonoNo ratings yet
- StrokeDocument1 pageStrokeDevina HarsonoNo ratings yet
- Effect of Estrogen On Skin Aging and The Potential Role of SERMs PDFDocument16 pagesEffect of Estrogen On Skin Aging and The Potential Role of SERMs PDFDevina HarsonoNo ratings yet
- Fertility Treatment When The Prognosis Is Very Poor or Futile: A Committee OpinionDocument4 pagesFertility Treatment When The Prognosis Is Very Poor or Futile: A Committee OpinionDevina HarsonoNo ratings yet
- Evaluating Infertility PDFDocument3 pagesEvaluating Infertility PDFJeff BakerNo ratings yet
- Abdominal PainDocument4 pagesAbdominal PainDevina HarsonoNo ratings yet
- Tension Pneumothorax: Diagnosis and TreatmentDocument14 pagesTension Pneumothorax: Diagnosis and TreatmentDevina HarsonoNo ratings yet
- SOCA 2008 - Semester 6Document1 pageSOCA 2008 - Semester 6Devina HarsonoNo ratings yet
- USG Dan CT KontrasDocument8 pagesUSG Dan CT KontrasDevina HarsonoNo ratings yet
- CT Adrenal Morphology in MalignancyDocument6 pagesCT Adrenal Morphology in MalignancyDevina HarsonoNo ratings yet
- CSO Skull SeriesDocument2 pagesCSO Skull SeriesWilchanNo ratings yet
- Traffic Sign Detection and Recognition Using Image ProcessingDocument7 pagesTraffic Sign Detection and Recognition Using Image ProcessingIJRASETPublicationsNo ratings yet
- IB Chemistry HL Test 2nd FEBDocument13 pagesIB Chemistry HL Test 2nd FEBprasad100% (1)
- LP Pressure TestingDocument34 pagesLP Pressure TestinglisaNo ratings yet
- A Kitchen in The Corner of The HouseDocument2 pagesA Kitchen in The Corner of The HousedanielrubarajNo ratings yet
- Projects in the Autonomous Region in Muslim MindanaoDocument4 pagesProjects in the Autonomous Region in Muslim MindanaoMark montebonNo ratings yet
- Mast Bending Stress Calculation: Antenna 1Document6 pagesMast Bending Stress Calculation: Antenna 1Vinay KumarNo ratings yet
- GBDocument10 pagesGBQuoctytranNo ratings yet
- Moisture ManagementDocument5 pagesMoisture ManagementSombis2011No ratings yet
- Indo American Journal of Pharmaceutical Research (India)Document4 pagesIndo American Journal of Pharmaceutical Research (India)Pharmacy2011journalsNo ratings yet
- Koh Pich Construction Company Cambodia-China Polytechnic University Daily Activities ReportDocument7 pagesKoh Pich Construction Company Cambodia-China Polytechnic University Daily Activities ReportNhoek RenNo ratings yet
- Boston Acoustic PDFDocument12 pagesBoston Acoustic PDFAdam StarkNo ratings yet
- Equations 2Document8 pagesEquations 2Patrick ValdezNo ratings yet
- 03-Mechanical Seal &seal System Basics-REV01Document39 pages03-Mechanical Seal &seal System Basics-REV01Fayez Al-ahmadiNo ratings yet
- ABB Price Book 714Document1 pageABB Price Book 714EliasNo ratings yet
- Dr. Carlos S. Lanting College: College of Maritime EducationDocument14 pagesDr. Carlos S. Lanting College: College of Maritime EducationJeynard Moler J. TanNo ratings yet
- The Ultimate Life GuideDocument12 pagesThe Ultimate Life GuideNLPCoachingNo ratings yet
- 2021 Vallourec Universal Registration DocumentDocument368 pages2021 Vallourec Universal Registration DocumentRolando Jara YoungNo ratings yet
- Ross 308 AP Broiler PO2019-EN PDFDocument16 pagesRoss 308 AP Broiler PO2019-EN PDFJORGE GALVISNo ratings yet
- El DoradoDocument12 pagesEl Doradoandrewwilliampalileo@yahoocomNo ratings yet
- US Army TV Course - Documentation Cinematography SS0536Document49 pagesUS Army TV Course - Documentation Cinematography SS0536innerethosNo ratings yet
- 4TWX4036 Service FactsDocument4 pages4TWX4036 Service FactsAlejandro OrdoñezNo ratings yet
- Final Project Proposal Digital Stopwatch-1Document6 pagesFinal Project Proposal Digital Stopwatch-1Shahid AbbasNo ratings yet