You might also like
- Social Thinking PresentationDocument87 pagesSocial Thinking PresentationLaura Bocsa100% (1)
- RAD: Reactive Attachment Disorder ResourcesDocument8 pagesRAD: Reactive Attachment Disorder ResourcesveronicaNo ratings yet
- Application of Attachment Theory To The Study of Sexual AbuseDocument11 pagesApplication of Attachment Theory To The Study of Sexual AbuseBea100% (3)
- Botanical Medicine PDFDocument80 pagesBotanical Medicine PDFDaniel100% (1)
- Vestibular Reha PDFDocument657 pagesVestibular Reha PDFRetnoNo ratings yet
- Physiotherapy Course PDFDocument156 pagesPhysiotherapy Course PDFMamta100% (1)
- Soap ChartingDocument31 pagesSoap ChartingterefagcanganNo ratings yet
- Blue Ocean Startegy: Prepared by Mugambikai Anbalagan Mpp172017 Aezrun Natasha Kharil Mpp171140Document26 pagesBlue Ocean Startegy: Prepared by Mugambikai Anbalagan Mpp172017 Aezrun Natasha Kharil Mpp171140Nor E'lee AhmedNo ratings yet
- The American Psychiatric Association Practice Guideline For The Treatment of Patients With Eating Disorders - TextDocument112 pagesThe American Psychiatric Association Practice Guideline For The Treatment of Patients With Eating Disorders - Textbraispm100% (1)
- Online Job Application for Staff Nurse Position in UAEDocument3 pagesOnline Job Application for Staff Nurse Position in UAEremzyliciousNo ratings yet
- Antiphospholipid SyndromeDocument6 pagesAntiphospholipid SyndromeOm Lakhani100% (1)
- Lymphatic System and San JiaoDocument6 pagesLymphatic System and San JiaoΒιβιλάκη Γεωργία100% (1)
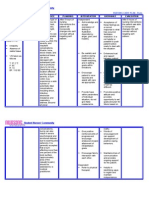
- 1 Burn NCPDocument2 pages1 Burn NCPkingjoy100% (1)
- Motivation, Success, and Problems of Entrepreneurs in NigeriaDocument7 pagesMotivation, Success, and Problems of Entrepreneurs in NigeriaOlufemi AladejebiNo ratings yet
- Sse Frankfurt Finance ClusterDocument36 pagesSse Frankfurt Finance ClusterSanskruti Kakadiya100% (1)
- Hank Kolb CaseDocument2 pagesHank Kolb Casejohnmia2067% (3)
- Perioperative CareDocument48 pagesPerioperative CareBryan FederizoNo ratings yet
- Sample Nursing Interview Questions & TipsDocument2 pagesSample Nursing Interview Questions & TipssamdakaNo ratings yet
- An Extension of Trust and TAM Model With TPB in The Initial Adoption of On-Line TaxDocument25 pagesAn Extension of Trust and TAM Model With TPB in The Initial Adoption of On-Line TaxcherilouderNo ratings yet
- Arabic TerminologiesDocument5 pagesArabic TerminologiesPearly Angelique Boco-MalateNo ratings yet
- The Movement Continuum Theory of Physical Therapy-2Document2 pagesThe Movement Continuum Theory of Physical Therapy-2Ingela Sjölin100% (2)
- 7.reduce Queue in Bank ANANDDocument2 pages7.reduce Queue in Bank ANANDoptimusNo ratings yet
- Natural Resource Based ViewDocument29 pagesNatural Resource Based Viewchau_969663535100% (1)
- Quiz 1 and 2 Operations and Processes Section 09312 Dated June 17 2021Document8 pagesQuiz 1 and 2 Operations and Processes Section 09312 Dated June 17 2021Hardeep SinghNo ratings yet
- TAM ModelDocument40 pagesTAM ModelAbhay VelayudhanNo ratings yet
- The Effect of Blog Trustworthiness, Product Attitude, and Blog Involvement On Purchase Intention PDFDocument13 pagesThe Effect of Blog Trustworthiness, Product Attitude, and Blog Involvement On Purchase Intention PDFJonathan GanNo ratings yet
- TAM Literature Survey Models User Acceptance SystemsDocument4 pagesTAM Literature Survey Models User Acceptance SystemsgamuchiraiNo ratings yet
- Digitalization of Insurance Industry of The Republic of UzbekistanDocument5 pagesDigitalization of Insurance Industry of The Republic of UzbekistanAcademic JournalNo ratings yet
- Chapter+16 IKEA Case+Study+SolutionDocument8 pagesChapter+16 IKEA Case+Study+SolutionJehan ZebNo ratings yet
- The Relationship Between Customer Satisfaction and Service Quality: A Study of Three Service Sectors in UmeåDocument16 pagesThe Relationship Between Customer Satisfaction and Service Quality: A Study of Three Service Sectors in UmeåMohsinRazaNo ratings yet
- M Rizqi Fabianto Case 3Document4 pagesM Rizqi Fabianto Case 3Deta DetadeNo ratings yet
- A Study On Consumer Perceptions Towards Digital Finance and Its Impact On Financial Inclusion - Indian ScenarioDocument12 pagesA Study On Consumer Perceptions Towards Digital Finance and Its Impact On Financial Inclusion - Indian ScenarioIAEME PublicationNo ratings yet
- Information systems provide competitive advantageDocument6 pagesInformation systems provide competitive advantageAfiq Naim100% (2)
- Global Goals For Local ImpactDocument9 pagesGlobal Goals For Local ImpactOpen_InstituteNo ratings yet
- Executive Information SystemsDocument6 pagesExecutive Information SystemsUsman Saleem0% (1)
- RyanairDocument7 pagesRyanairJoão CaladoNo ratings yet
- Consumer Acceptance of Online BankingDocument9 pagesConsumer Acceptance of Online BankingnewspiritNo ratings yet
- Journal of Exclusive Management Science - January 2017 - Vol 6 Issue 01 - ISSN 2277-5684Document6 pagesJournal of Exclusive Management Science - January 2017 - Vol 6 Issue 01 - ISSN 2277-5684archerselevatorsNo ratings yet
- FACTORS AFFECTING E-SAMSAT ACCEPTANCE (Study at The Denpasar SAMSAT Joint Office)Document9 pagesFACTORS AFFECTING E-SAMSAT ACCEPTANCE (Study at The Denpasar SAMSAT Joint Office)AJHSSR JournalNo ratings yet
- Assignment # 2 - Literature Review of Behavioral IntentionDocument14 pagesAssignment # 2 - Literature Review of Behavioral Intentionapi-3719928100% (1)
- The McDonald's StoryDocument13 pagesThe McDonald's Storyshaanchauhan2000No ratings yet
- A Critical Review of Technology Acceptance Literature - Long Li PHDDocument20 pagesA Critical Review of Technology Acceptance Literature - Long Li PHDnovriadi_dharmasrayaNo ratings yet
- Incremental Analysis Week 10 Practice ProblemsDocument2 pagesIncremental Analysis Week 10 Practice ProblemsLulu LuthfiyahNo ratings yet
- Right place at right time with global supply chain monitoringDocument3 pagesRight place at right time with global supply chain monitoringNina_C_ALNo ratings yet
- Android Smartphone Adoption and Intention To Pay For Mobile InternetDocument20 pagesAndroid Smartphone Adoption and Intention To Pay For Mobile InternetradislamyNo ratings yet
- The Impact of Social Presence in The Web Interface On Customer's Purchase Intention Toward Online Stores: The Case of VietnamDocument15 pagesThe Impact of Social Presence in The Web Interface On Customer's Purchase Intention Toward Online Stores: The Case of VietnamMohsinRazaNo ratings yet
- #10. IS Similarity - Post MADocument15 pages#10. IS Similarity - Post MAdewimachfudNo ratings yet
- Case Assignments For The Final Exam of The Business Strategy Course of MBA Progra1Document1 pageCase Assignments For The Final Exam of The Business Strategy Course of MBA Progra1AnikaEmaNo ratings yet
- A Study of Consumer Behavioral Intention To Use E-BooksDocument12 pagesA Study of Consumer Behavioral Intention To Use E-Booksjoe_vaillant0% (1)
- Determinants of Using Go-Pay and Its Impact On Net BenefitsDocument10 pagesDeterminants of Using Go-Pay and Its Impact On Net BenefitsInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Consumer Acceptance and Use of IT-UTAUT2Document22 pagesConsumer Acceptance and Use of IT-UTAUT2Jamirul SyafiqNo ratings yet
- Math Model in Banking SystemDocument13 pagesMath Model in Banking SystemElmir HalilčevićNo ratings yet
- Factors Influencing Acceptance of E-Learning Systems in Higher Ed and Lifelong LearningDocument14 pagesFactors Influencing Acceptance of E-Learning Systems in Higher Ed and Lifelong LearningMohammed ABDO ALBAOMNo ratings yet
- Dogan 2017 A Strategic Approach To InnovationDocument11 pagesDogan 2017 A Strategic Approach To Innovationemigdio_alfaro9892No ratings yet
- Analyzing Cash Flow Projects and Capital Budgeting DecisionsDocument3 pagesAnalyzing Cash Flow Projects and Capital Budgeting DecisionsAlthea LandichoNo ratings yet
- Impact of Online Banking Services: A Study: Associate Professor, Department of Commerce, Alagappa University, KaraikudiDocument10 pagesImpact of Online Banking Services: A Study: Associate Professor, Department of Commerce, Alagappa University, KaraikudiALL OVER EMPIRENo ratings yet
- BSMT - 18025 - Entrepreneurship Assignment#2 (Go-Jek)Document3 pagesBSMT - 18025 - Entrepreneurship Assignment#2 (Go-Jek)Saad SajjadNo ratings yet
- Corporate Foresight in Multinational Business StrategiesDocument15 pagesCorporate Foresight in Multinational Business StrategiesAladdin PrinceNo ratings yet
- Term PaperDocument16 pagesTerm PaperAnu MoudgilNo ratings yet
- Customer ExpirienceDocument28 pagesCustomer ExpirienceYARON11No ratings yet
- HP Supplying DeskJet Printers in EuropeDocument3 pagesHP Supplying DeskJet Printers in EuropeAditya Anshuman DashNo ratings yet
- Effect of Information Communication Technology On Human Resource Productivity of Iranian National Oil CompanyDocument6 pagesEffect of Information Communication Technology On Human Resource Productivity of Iranian National Oil Companyieom2012No ratings yet
- Employee EngagementDocument12 pagesEmployee Engagementaa1122No ratings yet
- Temsa Global's product strategy shift and organizational changesDocument5 pagesTemsa Global's product strategy shift and organizational changesfirinaluvina100% (1)
- 2013 - SULI - SULI - Annual Report - 2013 PDFDocument46 pages2013 - SULI - SULI - Annual Report - 2013 PDFulfadwimustika0% (1)
- Research ProposalDocument16 pagesResearch ProposalPaulos MekuriaNo ratings yet
- Organisational Change Management A Critical ReviewDocument13 pagesOrganisational Change Management A Critical Reviewhimanshu100% (1)
- Case 13 Jordan Telecom GroupDocument19 pagesCase 13 Jordan Telecom GroupKad Saad100% (2)
- Online Food DeliveryDocument3 pagesOnline Food DeliveryAkash soniNo ratings yet
- The Attitude of Finish Accountant Towards Paperless AccountingDocument3 pagesThe Attitude of Finish Accountant Towards Paperless AccountingHelena ThomasNo ratings yet
- Impact of Smartphone News Apps On Print Media - A Twin TAM FrameworkDocument9 pagesImpact of Smartphone News Apps On Print Media - A Twin TAM FrameworkIOSRjournalNo ratings yet
- Evaluation of The Impact External Factors Could Have On Tesco PLC For Future ProspectsDocument7 pagesEvaluation of The Impact External Factors Could Have On Tesco PLC For Future ProspectsJody Mc LaughlinNo ratings yet
- Operational Research in Food DeliveryDocument3 pagesOperational Research in Food DeliveryNurIrlyani0% (1)
- The Strategic Development of Procter and Gamble Into A GlobalDocument5 pagesThe Strategic Development of Procter and Gamble Into A Globalkhurram36No ratings yet
- The impact of social factors on car purchase characteristics selectionDocument13 pagesThe impact of social factors on car purchase characteristics selectionmtdinhthuan4483No ratings yet
- Turkey's First and Largest Online Food Provider CompanyDocument13 pagesTurkey's First and Largest Online Food Provider CompanywavelliNo ratings yet
- Case AnalysisDocument11 pagesCase AnalysisHammad Noor67% (3)
- HO 4 Process AnalysisDocument3 pagesHO 4 Process Analysisjohnmia20No ratings yet
- Job Design and Work Measurement TechniquesDocument8 pagesJob Design and Work Measurement Techniquesjohnmia20100% (1)
- Ops Strat FrameworkDocument4 pagesOps Strat Frameworkjohnmia20No ratings yet
- HO 3 Project ManagementDocument8 pagesHO 3 Project Managementjohnmia20No ratings yet
- Internet Case For Supplement 7Document3 pagesInternet Case For Supplement 7johnmia20No ratings yet
- Process ManagmentDocument1 pageProcess Managmentjohnmia20No ratings yet
- HO 1 IntroductionDocument4 pagesHO 1 Introductionjohnmia20No ratings yet
- Operations & Supply ManagementDocument10 pagesOperations & Supply Managementjohnmia20No ratings yet
- Solution To 11Document2 pagesSolution To 11johnmia20No ratings yet
- Operations & Supply ManagementDocument10 pagesOperations & Supply Managementjohnmia20No ratings yet
- Operations Management 12.15 AssignmentDocument1 pageOperations Management 12.15 Assignmentjohnmia20No ratings yet
- Yellow tablet demand and forecasting methods under 40 charsDocument2 pagesYellow tablet demand and forecasting methods under 40 charsjohnmia20No ratings yet
- OM QuizDocument10 pagesOM Quizjohnmia20No ratings yet
- Operations Management 12.15 AssignmentDocument1 pageOperations Management 12.15 Assignmentjohnmia20No ratings yet
- Operations Management AssignmentDocument3 pagesOperations Management Assignmentjohnmia20No ratings yet
- Operations Management AssignmentDocument3 pagesOperations Management Assignmentjohnmia20No ratings yet
- Template For SynthesesDocument2 pagesTemplate For Synthesesjohnmia20No ratings yet
- 6.PIO TTG Seven Step Handling QueryDocument29 pages6.PIO TTG Seven Step Handling QueryNurinaAdaniSukiakusumahNo ratings yet
- Screenshot 2022-12-14 at 4.16.40 PMDocument1 pageScreenshot 2022-12-14 at 4.16.40 PMPrisha SoniNo ratings yet
- ISAKOS Classification System Provides Comprehensive Assessment of Rotator Cuff TearsDocument4 pagesISAKOS Classification System Provides Comprehensive Assessment of Rotator Cuff TearsAntonio PNo ratings yet
- PKPD For BeginnersDocument8 pagesPKPD For Beginnerstanty_ukNo ratings yet
- Sucker Punch Inspired Workout PDFDocument19 pagesSucker Punch Inspired Workout PDFShuvajoyyyNo ratings yet
- Uterine Fibroids: Causes, Symptoms and Treatment OptionsDocument25 pagesUterine Fibroids: Causes, Symptoms and Treatment OptionssyifasfNo ratings yet
- Practical Research 2: "Correlation of Anxiety To Students' Achievement"Document4 pagesPractical Research 2: "Correlation of Anxiety To Students' Achievement"Marie LargoNo ratings yet
- Peritoneal DialysisDocument5 pagesPeritoneal DialysisLisette TupasNo ratings yet
- PsychiaDocument9 pagesPsychiaNoel RafaelNo ratings yet
- Current Issues in Spinal AnesthesiaDocument19 pagesCurrent Issues in Spinal AnesthesiaNadhifah RahmawatiNo ratings yet
- Single Visit EndodonticsDocument6 pagesSingle Visit EndodonticsSerene Kenny100% (1)
- Post Op Lumbar FusionDocument3 pagesPost Op Lumbar FusionBaiq LenyNo ratings yet
- ChemoDocument32 pagesChemoJehannah Dayanara HayudiniNo ratings yet
- Paracetamol Use Dec 2008Document30 pagesParacetamol Use Dec 2008Nararto PrijogoNo ratings yet