You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Naskah Oldriana Prawiro HapsariDocument10 pagesNaskah Oldriana Prawiro HapsariOldriana Prawiro HapsariNo ratings yet
- 2009 Veiros Et AlDocument7 pages2009 Veiros Et AlOldriana Prawiro HapsariNo ratings yet
- Precede-Proceed ModelDocument16 pagesPrecede-Proceed ModelOldriana Prawiro Hapsari100% (1)
- Precede/ProceedDocument10 pagesPrecede/ProceedOldriana Prawiro HapsariNo ratings yet
- Thesis Prop Trial Print BWDocument18 pagesThesis Prop Trial Print BWOldriana Prawiro HapsariNo ratings yet
- Gordon's 11 Functional Health PatternsDocument1 pageGordon's 11 Functional Health PatternsTracy100% (37)
- The Precede/Proceed Model: 1. OriginatorsDocument7 pagesThe Precede/Proceed Model: 1. OriginatorsdrhafizsameeNo ratings yet
- Instruments RefDocument1 pageInstruments RefOldriana Prawiro HapsariNo ratings yet
- Analysis Of Hygiene and Sanitation Practice Within Hospital Foodservice EmployeesDocument18 pagesAnalysis Of Hygiene and Sanitation Practice Within Hospital Foodservice EmployeesOldriana Prawiro HapsariNo ratings yet
- 9 Qualitative Data Analysis Revision 2009Document46 pages9 Qualitative Data Analysis Revision 2009camilagoncaloNo ratings yet
- Writing A Conceptual FrameworkDocument28 pagesWriting A Conceptual FrameworkNurr Hayaatii YahyaNo ratings yet
- Vital Signs Reference Chart 1.2 - 1 PDFDocument1 pageVital Signs Reference Chart 1.2 - 1 PDFSerious Leo100% (1)
- Theories of Perception Part 1Document29 pagesTheories of Perception Part 1Oldriana Prawiro HapsariNo ratings yet
- Application of The WHO Keys of Safer Food To Improve Food Handling Practices of Food Vendors in A Poor Resource Community in GhanaDocument10 pagesApplication of The WHO Keys of Safer Food To Improve Food Handling Practices of Food Vendors in A Poor Resource Community in GhanaOldriana Prawiro HapsariNo ratings yet
- 16 ICUInsulinOrdersDocument2 pages16 ICUInsulinOrdersJahangir AlamNo ratings yet
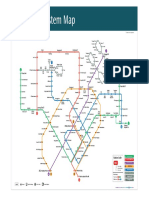
- MRT lines status updateDocument1 pageMRT lines status updateOldriana Prawiro HapsariNo ratings yet
- Anderson S Theory of FaultingDocument25 pagesAnderson S Theory of FaultingAnonymous yZtOPr4FDq100% (2)
- L Green Theory PDFDocument36 pagesL Green Theory PDFOldriana Prawiro HapsariNo ratings yet
- New Usg NovDocument14 pagesNew Usg NovOldriana Prawiro HapsariNo ratings yet
- Kerning and Brudzinski-MeningitaDocument2 pagesKerning and Brudzinski-MeningitaDobre CristinaNo ratings yet
- Yogijicreationspvt Copy 110326050847 Phpapp02Document50 pagesYogijicreationspvt Copy 110326050847 Phpapp02Aditya MajumderNo ratings yet
- EdemaDocument39 pagesEdemaMariyah Qibtiyyah Al JufriNo ratings yet
- ASA Physical Status Classification System PDFDocument2 pagesASA Physical Status Classification System PDFOldriana Prawiro HapsariNo ratings yet
- Foundation Volume 3, Chapter 39, Bacterial ConjunctivitisDocument25 pagesFoundation Volume 3, Chapter 39, Bacterial ConjunctivitisOldriana Prawiro HapsariNo ratings yet
- Rad CraniosynostosisDocument10 pagesRad CraniosynostosisOldriana Prawiro HapsariNo ratings yet
- VOU 17dec2013 DeDeyneC Postgrad Med J 2012 Harris 588-94-1Document9 pagesVOU 17dec2013 DeDeyneC Postgrad Med J 2012 Harris 588-94-1Oldriana Prawiro HapsariNo ratings yet
- Ulkus Kornea Review of Ophthalmology® - Winning The Battle Against Corneal UlcersDocument5 pagesUlkus Kornea Review of Ophthalmology® - Winning The Battle Against Corneal UlcersOldriana Prawiro HapsariNo ratings yet
- DocumentDocument11 pagesDocumentWilly Dwi FebrianNo ratings yet
- OligohydramnioDocument17 pagesOligohydramnioOldriana Prawiro HapsariNo ratings yet
- Archives of Surgery (Chicago Ill 1960) 2010 EvansDocument6 pagesArchives of Surgery (Chicago Ill 1960) 2010 EvansOldriana Prawiro HapsariNo ratings yet
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (894)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Septic Shock Nursing Assessment and ManagementDocument6 pagesSeptic Shock Nursing Assessment and ManagementJenn GallowayNo ratings yet
- Pil - 02Document14 pagesPil - 02Geetika Khandelwal100% (1)
- General Surgery Who PDFDocument83 pagesGeneral Surgery Who PDFMeta Rahma An NazzilaNo ratings yet
- Natural Anti Viral Self Defense StevenWmFowkesDocument251 pagesNatural Anti Viral Self Defense StevenWmFowkesChristopher Phillips100% (1)
- Microbiology The Human ExperienceDocument5 pagesMicrobiology The Human ExperiencezemmiphobiaNo ratings yet
- Antibiotic Guideline Final October 2019Document22 pagesAntibiotic Guideline Final October 2019Cory BurnNo ratings yet
- Virus CultivationDocument33 pagesVirus Cultivationved.g007No ratings yet
- Chain of InfectionDocument3 pagesChain of InfectionShaina SantosNo ratings yet
- ReplotDocument395 pagesReplotMasigdalaNo ratings yet
- iNQUIRIES - Research PaperDocument17 pagesiNQUIRIES - Research PaperTeddyNo ratings yet
- المختص في الحشرات -Synopsis of Medical EntomologyاDocument63 pagesالمختص في الحشرات -Synopsis of Medical EntomologyاDrMohamedBenrashedNo ratings yet
- Communicable Disease Nursing ENHANCER Day 2Document1 pageCommunicable Disease Nursing ENHANCER Day 2Mcbry TiongNo ratings yet
- Extended Product Information Esha 2000supregsupDocument3 pagesExtended Product Information Esha 2000supregsupGustavoNo ratings yet
- 551-Article Text-1710-1-10-20210609Document17 pages551-Article Text-1710-1-10-20210609Grace ManzanoNo ratings yet
- SP Hic Manual PDFDocument76 pagesSP Hic Manual PDFANTO MATHINo ratings yet
- How To Take Care of DogDocument12 pagesHow To Take Care of DogVinod K PillaiNo ratings yet
- Prevalence and Risk Factors of Puerperal Sepsisbamong Reproductive Aged Women at Jinja Regional Referral Hospital From January 2019 To June 2020Document14 pagesPrevalence and Risk Factors of Puerperal Sepsisbamong Reproductive Aged Women at Jinja Regional Referral Hospital From January 2019 To June 2020KIU PUBLICATION AND EXTENSIONNo ratings yet
- BEGUMDocument12 pagesBEGUMRODHIANSYAH DJAYASINGANo ratings yet
- III3 FinalManuscriptDocument54 pagesIII3 FinalManuscriptYESORYES0% (1)
- Hiv AidsDocument18 pagesHiv Aidskerema BadasaNo ratings yet
- Antimicrobial Resistance in Health & DiseaseDocument130 pagesAntimicrobial Resistance in Health & Diseaseadithya polavarapuNo ratings yet
- Your COVID-19 test result negativeDocument2 pagesYour COVID-19 test result negativeSeiyi KohayagawaNo ratings yet
- HIV/AIDS Awareness: World AIDS Day (Dec 1stDocument31 pagesHIV/AIDS Awareness: World AIDS Day (Dec 1stRatneshNo ratings yet
- Rickettsia IFA IgG Detection TestDocument4 pagesRickettsia IFA IgG Detection TestIhdinal MuktiNo ratings yet
- Aggressive Periodontitis GoodDocument99 pagesAggressive Periodontitis GoodDr.Manisha DeolNo ratings yet
- Parasite CleanseDocument17 pagesParasite CleanseHisExcellencyNo ratings yet
- SMEs in Health ResearchDocument192 pagesSMEs in Health ResearchdmaproiectNo ratings yet
- Recent Advances in OtolaryngologyDocument305 pagesRecent Advances in OtolaryngologyDr. T. Balasubramanian80% (5)
- BC-6800 Brochure (V3) PDFDocument16 pagesBC-6800 Brochure (V3) PDFSasa AbassNo ratings yet
- Course Outline in Medical MicrobiologyDocument5 pagesCourse Outline in Medical MicrobiologyRami Tounsi100% (1)