You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- Part 1 Sample Questions MRCPDocument33 pagesPart 1 Sample Questions MRCPCharan Pal Singh100% (1)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Neurobiology of Mental IllnessDocument1,024 pagesNeurobiology of Mental IllnessMario Barragan Cortez100% (1)
- Special Considerations in Pediatric Sepsis ManagementDocument3 pagesSpecial Considerations in Pediatric Sepsis ManagementWalter LojaNo ratings yet
- Signs Liver Failure NAC Treatment Paracetamol PoisoningDocument1 pageSigns Liver Failure NAC Treatment Paracetamol PoisoningCalvinNo ratings yet
- Innova PM Ipte - 3Document1 pageInnova PM Ipte - 3CalvinNo ratings yet
- Maat 05 I 3 P 256Document2 pagesMaat 05 I 3 P 256CalvinNo ratings yet
- May 2009Document4 pagesMay 2009CalvinNo ratings yet
- CEM6578 CEC Letter Re Pararacetamol Guidance 03-09-12 (FINAL)Document1 pageCEM6578 CEC Letter Re Pararacetamol Guidance 03-09-12 (FINAL)CalvinNo ratings yet
- Confidentiality Disclosing Info Serious Commun Diseases 2009.PDF 27493404Document3 pagesConfidentiality Disclosing Info Serious Commun Diseases 2009.PDF 27493404CalvinNo ratings yet
- MRCP 201 20may 202014Document101 pagesMRCP 201 20may 202014CalvinNo ratings yet
- Special Considerations in Pediatric Sepsis ManagementDocument3 pagesSpecial Considerations in Pediatric Sepsis ManagementWalter LojaNo ratings yet
- CEM6579 CEC Letter Re Pararacetamol Guidance 03-09-12 (FINAL ANNEX 1 and 2)Document3 pagesCEM6579 CEC Letter Re Pararacetamol Guidance 03-09-12 (FINAL ANNEX 1 and 2)CalvinNo ratings yet
- Last Minute Pic MRCP2 - Q&ADocument16 pagesLast Minute Pic MRCP2 - Q&ACalvinNo ratings yet
- From: Chapter 25. Male Genital System: Skandalakis' Surgical Anatomy, 2004Document1 pageFrom: Chapter 25. Male Genital System: Skandalakis' Surgical Anatomy, 2004CalvinNo ratings yet
- What Is Memory Loss and What Are The Causes?Document14 pagesWhat Is Memory Loss and What Are The Causes?CalvinNo ratings yet
- Blank 1Document4 pagesBlank 1CalvinNo ratings yet
- CEM6579 CEC Letter Re Pararacetamol Guidance 03-09-12 (FINAL ANNEX 1 and 2)Document3 pagesCEM6579 CEC Letter Re Pararacetamol Guidance 03-09-12 (FINAL ANNEX 1 and 2)CalvinNo ratings yet
- CEM6692 LRI ED Paracet Docu 62 For CEMDocument2 pagesCEM6692 LRI ED Paracet Docu 62 For CEMCalvinNo ratings yet
- Benign Prostatic Hyperplasia: Tan Jack SyenDocument7 pagesBenign Prostatic Hyperplasia: Tan Jack SyenCalvinNo ratings yet
- From: Chapter 29. Colon, Rectum, and Anus: Schwartz's Principles of Surgery, 9e, 2010Document1 pageFrom: Chapter 29. Colon, Rectum, and Anus: Schwartz's Principles of Surgery, 9e, 2010CalvinNo ratings yet
- Benign Prostatic Hyperplasia Library NotesDocument31 pagesBenign Prostatic Hyperplasia Library NotesCalvinNo ratings yet
- Benign Prostatic Hyperplasia PDFDocument496 pagesBenign Prostatic Hyperplasia PDFnurul_nufafinaNo ratings yet
- CEM6578 CEC Letter Re Pararacetamol Guidance 03-09-12 (FINAL)Document1 pageCEM6578 CEC Letter Re Pararacetamol Guidance 03-09-12 (FINAL)CalvinNo ratings yet
- Medscape Upper GI BleedDocument6 pagesMedscape Upper GI BleedCalvinNo ratings yet
- Investigations of HydfsadpertensionDocument9 pagesInvestigations of HydfsadpertensionCalvinNo ratings yet
- Vertigo Gail Ishiyama 1 13 10Document40 pagesVertigo Gail Ishiyama 1 13 10Myname Rama LienNo ratings yet
- Vertigo03 10Document3 pagesVertigo03 10CalvinNo ratings yet
- Ent 2Document45 pagesEnt 2Calvin100% (1)
- 10 PopescuDocument3 pages10 PopescuCalvinNo ratings yet
- MRCP April 2013Document6 pagesMRCP April 2013CalvinNo ratings yet
- Freud'S Analysis of Horace Frink, M.D.: A Previously Unexplained Therapeutic DisasterDocument16 pagesFreud'S Analysis of Horace Frink, M.D.: A Previously Unexplained Therapeutic DisasterIVAN ANDREE VICTORIA VARGASNo ratings yet
- CPG Unerupted Maxillary IncisorDocument19 pagesCPG Unerupted Maxillary IncisorAnonymous 1nLozzNo ratings yet
- Careers in Medicine CV Sample #4Document3 pagesCareers in Medicine CV Sample #4huyenthanh1807No ratings yet
- Berra 2020Document12 pagesBerra 2020Indri AswariNo ratings yet
- Mauban District Hospital: Epublic of The Philippines Province of Quezon Mauban, QuezonDocument2 pagesMauban District Hospital: Epublic of The Philippines Province of Quezon Mauban, QuezonAlmira MenggeNo ratings yet
- Laurie Curtis and Melody RieferDocument5 pagesLaurie Curtis and Melody RieferdwellintheheartNo ratings yet
- 10 Surgical Considerations in Older Adults - Ethics and Palliative CareDocument13 pages10 Surgical Considerations in Older Adults - Ethics and Palliative CareMyrtle Yvonne RagubNo ratings yet
- FP Form 1Document2 pagesFP Form 1hhhirangNo ratings yet
- Dopamine Drug StudyDocument6 pagesDopamine Drug StudyGeorge RussellNo ratings yet
- HealthinDubai 3Document325 pagesHealthinDubai 3GaladariNo ratings yet
- Gastrointestinal MotilityDocument20 pagesGastrointestinal Motilitymuh nuerNo ratings yet
- Guideline: Critical Care: Document Number: Functional Sub-Group: SummaryDocument11 pagesGuideline: Critical Care: Document Number: Functional Sub-Group: SummaryAndrew Lyngdoh100% (1)
- Radical NephrectomyDocument3 pagesRadical NephrectomyBiggs JuntillaNo ratings yet
- Aesthetic Medicine Training CourseDocument8 pagesAesthetic Medicine Training Coursedrdahabra3No ratings yet
- Cases in Nephrology by Muhammad Rafiqul AlamDocument9 pagesCases in Nephrology by Muhammad Rafiqul AlamSELLULARNo ratings yet
- A Sociofugal Space for Privacy in ConsultationDocument7 pagesA Sociofugal Space for Privacy in ConsultationDennis Villaruz-AliasNo ratings yet
- Hormone Replacement Therapy (HRT) Evidence-Based Guidelines: DR Mahdy El-Mazzahy Damietta General HospitalDocument38 pagesHormone Replacement Therapy (HRT) Evidence-Based Guidelines: DR Mahdy El-Mazzahy Damietta General Hospitalhossam626No ratings yet
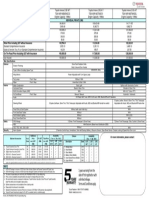
- MyShield Gives Extra Hospital Care As ChargedDocument32 pagesMyShield Gives Extra Hospital Care As ChargedJason TanNo ratings yet
- Drugs To Watch With WARFARINDocument3 pagesDrugs To Watch With WARFARINRajendra RaiNo ratings yet
- Case Assigntment - OsteoporosisDocument7 pagesCase Assigntment - OsteoporosisYasser HoldarNo ratings yet
- 21 Test BankDocument17 pages21 Test BankNaNo ratings yet
- 2021 HIDTA Hawaii Drug Death and Overdose ReportDocument14 pages2021 HIDTA Hawaii Drug Death and Overdose ReportTiffany De MastersNo ratings yet
- CHILD PSYCHIATRY EXAMINES BEHAVIORAL ISSUESDocument14 pagesCHILD PSYCHIATRY EXAMINES BEHAVIORAL ISSUESabrihamNo ratings yet
- Dialysis BrochureDocument13 pagesDialysis BrochureRaffy FlorentinoNo ratings yet
- LSHTM ProspectusDocument32 pagesLSHTM ProspectusNayeon KimNo ratings yet
- Pathophysiology Invasive Ductal Carcinoma Breast Cancer StagesDocument3 pagesPathophysiology Invasive Ductal Carcinoma Breast Cancer StagesAngelique Ramos Pascua100% (1)
- Pentecostal Perspectives: Faith Healing of Cancer and HIV/AIDSDocument3 pagesPentecostal Perspectives: Faith Healing of Cancer and HIV/AIDStruevine_ministryNo ratings yet
- ACE Group Fitness Instructor Certification GuideDocument36 pagesACE Group Fitness Instructor Certification GuideLouis TrầnNo ratings yet
- Test Bank For Managing and Coordinating Nursing Care Fifth EditionDocument7 pagesTest Bank For Managing and Coordinating Nursing Care Fifth Editionkelliejenkinsxzqnyeajkt100% (23)