You might also like
- Thyroglossal Duct Cysts, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandThyroglossal Duct Cysts, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Perichondritis PinnaDocument2 pagesPerichondritis PinnaAnish RajNo ratings yet
- Laryngeal Trauma: Dr. Ida Sjailandrawati Harahap, SP.T.H.T.K.LDocument19 pagesLaryngeal Trauma: Dr. Ida Sjailandrawati Harahap, SP.T.H.T.K.LNoni100% (1)
- Maxillary Sinus Approaches and Disease ManagementDocument23 pagesMaxillary Sinus Approaches and Disease ManagementAhmed KhattabNo ratings yet
- Diagnosis & Management of Midface FracturesDocument66 pagesDiagnosis & Management of Midface FracturesSobia NaseemNo ratings yet
- Suarez - Ent EmergenciesDocument36 pagesSuarez - Ent EmergenciesCarina SuarezNo ratings yet
- Deviated Nasal Septum: Ahmednagar Homoeopathic Medical College & Hospital AhmednagarDocument13 pagesDeviated Nasal Septum: Ahmednagar Homoeopathic Medical College & Hospital AhmednagarSuhas IngaleNo ratings yet
- Surgical Treatment of Postintubation Tracheal StenosisDocument40 pagesSurgical Treatment of Postintubation Tracheal StenosisJessieca LiusenNo ratings yet
- Disease of The Oral CavityDocument86 pagesDisease of The Oral CavityAnonymous wqnuimNo ratings yet
- AtelektasisDocument15 pagesAtelektasisMuhammad Ade RahmanNo ratings yet
- Chronic TonsillitisDocument47 pagesChronic Tonsillitissuci0% (1)
- Maxillary Sinus CarcinomaDocument4 pagesMaxillary Sinus CarcinomaSuresh MettaNo ratings yet
- Lip Cancer-Ablative and Reconstructive Surgery: ChapDocument52 pagesLip Cancer-Ablative and Reconstructive Surgery: ChapYang Lin Chen100% (1)
- Ear Infection Assessment and ManagementDocument8 pagesEar Infection Assessment and ManagementArt Christian Ramos100% (1)
- Cranial Nerve AssessmentDocument17 pagesCranial Nerve AssessmentMahendran Jayaraman100% (1)
- Epidemiology of Oral Cancer PDFDocument6 pagesEpidemiology of Oral Cancer PDFمحمد عبدالهادي إسماعيلNo ratings yet
- Cleft Lip & PalateDocument11 pagesCleft Lip & Palaterittika dasNo ratings yet
- Chronic Otitis Media, Cholesteatoma, and Mastoiditis in AdultsDocument14 pagesChronic Otitis Media, Cholesteatoma, and Mastoiditis in AdultschristineNo ratings yet
- Cancer LaryncDocument35 pagesCancer LaryncSaya MenangNo ratings yet
- Cochlear Implant Surgery Treatment & Management - Medical Therapy, Surgical Therapy, Preoperative DetailsDocument9 pagesCochlear Implant Surgery Treatment & Management - Medical Therapy, Surgical Therapy, Preoperative DetailsFityah UfiNo ratings yet
- Chylous Fistula of The NeckDocument44 pagesChylous Fistula of The Neckgk_anandaNo ratings yet
- External Ear DiseaseDocument60 pagesExternal Ear Diseasenitas23100% (1)
- Ototoxicity LatestDocument37 pagesOtotoxicity LatestSucdi CabdiNo ratings yet
- OtosclerosisDocument44 pagesOtosclerosisSonal Sharma100% (1)
- Keratosis ObturansDocument2 pagesKeratosis ObturansAnish RajNo ratings yet
- Pharyngeal Tumours2Document46 pagesPharyngeal Tumours2miramirajalalNo ratings yet
- Causes, Signs, Treatment of Acute Otitis MediaDocument19 pagesCauses, Signs, Treatment of Acute Otitis MediaRajesh Sharma100% (1)
- Space InfectionsDocument60 pagesSpace InfectionsDan 04No ratings yet
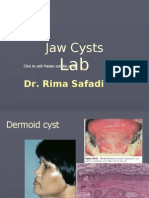
- Lab 4 Jaw Cysts (Slide)Document80 pagesLab 4 Jaw Cysts (Slide)JustDen09No ratings yet
- Upper Airway ObstructionDocument31 pagesUpper Airway ObstructiontrimardiyanaisyanNo ratings yet
- Everything You Need to Know About HerniasDocument47 pagesEverything You Need to Know About HerniasmalathiNo ratings yet
- Benign Tumors of LarynxDocument48 pagesBenign Tumors of LarynxVilZan MominNo ratings yet
- 1) BiopsyDocument30 pages1) BiopsySosa GeorgeNo ratings yet
- Child Ear Infection CausesDocument9 pagesChild Ear Infection CausesMona Santi NainggolanNo ratings yet
- Nasopharyngeal CarcinomaDocument44 pagesNasopharyngeal CarcinomapopoyingNo ratings yet
- Stridor in Children: By: Maj Vishal Gaurav Moderator: DR A SethiDocument33 pagesStridor in Children: By: Maj Vishal Gaurav Moderator: DR A SethiVishal GauravNo ratings yet
- Midface FracturesDocument31 pagesMidface FracturesJoyabrata SarkarNo ratings yet
- Vitamin A and XerophthalmiaDocument29 pagesVitamin A and XerophthalmiaJayashree IyerNo ratings yet
- Maxillofacial - Infection - Dari KikiDrDocument20 pagesMaxillofacial - Infection - Dari KikiDrmashitadyahNo ratings yet
- Management of Lefort FracturesDocument93 pagesManagement of Lefort FracturesKassim OboghenaNo ratings yet
- Otitis MediaDocument6 pagesOtitis MediaririNo ratings yet
- Otitis Media With EffusionDocument3 pagesOtitis Media With EffusionAnish RajNo ratings yet
- Understanding Otosclerosis: Causes, Symptoms and TreatmentDocument38 pagesUnderstanding Otosclerosis: Causes, Symptoms and TreatmentSushmita Kaldan100% (1)
- Chronic SinusitisDocument19 pagesChronic SinusitisMunawwar AwaNo ratings yet
- Infective Endocarditis Symptoms and CausesDocument54 pagesInfective Endocarditis Symptoms and CausesTommy Dearfield100% (1)
- Laryngeal Cancer: Anatomy, Risk Factors, Staging and TreatmentDocument41 pagesLaryngeal Cancer: Anatomy, Risk Factors, Staging and TreatmentNidya PutriNo ratings yet
- Anatomy and Physiology of the ConjunctivaDocument43 pagesAnatomy and Physiology of the ConjunctivaVincentius Okta VidiandickaNo ratings yet
- Median Rhomboid GlossitisDocument2 pagesMedian Rhomboid Glossitisdianzalerti9240No ratings yet
- Ectropion vs. EntropionDocument1 pageEctropion vs. EntropionAhmed ShafikNo ratings yet
- Recurrent Respiratory Papillomatosis: FaringDocument49 pagesRecurrent Respiratory Papillomatosis: FaringIchsanJuliansyahNo ratings yet
- Tracheostomy Procedure GuideDocument18 pagesTracheostomy Procedure GuideSudhanshu ShekharNo ratings yet
- Upper Airway ObstructionDocument17 pagesUpper Airway ObstructionRai Hana100% (1)
- Cortical Mastoid SurgeryDocument22 pagesCortical Mastoid Surgerymanu100% (1)
- Sialolithiasis: Vi Ugboko Fmcds FwacsDocument47 pagesSialolithiasis: Vi Ugboko Fmcds FwacsAkeem Alawode50% (2)
- Cleft Lip and Palate CareDocument16 pagesCleft Lip and Palate CareIsmail LubisNo ratings yet
- Anatomy of EarDocument92 pagesAnatomy of EarGaurav KatariaNo ratings yet
- Ranula Cyst, (Salivary Cyst) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandRanula Cyst, (Salivary Cyst) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Inflamed Trachea, (Tracheitis) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandInflamed Trachea, (Tracheitis) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- An Evidence-Based Approach to the Management of Nasopharyngeal Cancer: From Basic Science to Clinical Presentation and TreatmentFrom EverandAn Evidence-Based Approach to the Management of Nasopharyngeal Cancer: From Basic Science to Clinical Presentation and TreatmentBaharudin AbdullahNo ratings yet
- R2Document3 pagesR2Condurache Ilie-AndreiNo ratings yet
- R1Document3 pagesR1Condurache Ilie-AndreiNo ratings yet
- Text RandomDocument2 pagesText RandomradioPHNo ratings yet
- GasghsahDocument4 pagesGasghsahCondurache Ilie-AndreiNo ratings yet
- ReadmeDocument4 pagesReadmeCondurache Ilie-AndreiNo ratings yet
- 3Document1 page3Condurache Ilie-AndreiNo ratings yet
- 2Document2 pages2Condurache Ilie-AndreiNo ratings yet
- PatchnoteDocument1 pagePatchnoteCondurache Ilie-AndreiNo ratings yet
- 1Document2 pages1Condurache Ilie-AndreiNo ratings yet
- 4Document2 pages4Condurache Ilie-AndreiNo ratings yet
- WWDocument1 pageWWanon_295126143No ratings yet
- 6618 Desire Points PDFDocument1 page6618 Desire Points PDFCondurache Ilie-AndreiNo ratings yet
- King's RaidDocument1 pageKing's RaidCondurache Ilie-AndreiNo ratings yet
- GasgasDocument3 pagesGasgasCondurache Ilie-AndreiNo ratings yet
- ChangesDocument242 pagesChangesbqiceNo ratings yet
- Renal Considerations in Angiotensin Converting Enzyme Inhibitor TherapyDocument8 pagesRenal Considerations in Angiotensin Converting Enzyme Inhibitor TherapyCondurache Ilie-AndreiNo ratings yet
- Read Me, Pretty PleaseDocument1 pageRead Me, Pretty PleaseCondurache Ilie-AndreiNo ratings yet
- CodDocument1 pageCodCondurache Ilie-AndreiNo ratings yet
- Walkthrough by A Backdated FutureDocument270 pagesWalkthrough by A Backdated FutureCondurache Ilie-AndreiNo ratings yet
- Ediatrics: Epidemiology and Clinical Characteristics of Community-Acquired Pneumonia in Hospitalized ChildrenDocument9 pagesEdiatrics: Epidemiology and Clinical Characteristics of Community-Acquired Pneumonia in Hospitalized ChildrenCondurache Ilie-AndreiNo ratings yet
- List of students with personal detailsDocument64 pagesList of students with personal detailsCondurache Ilie-AndreiNo ratings yet
- 104Document28 pages104Condurache Ilie-AndreiNo ratings yet
- Epidemiology, Risk Factors and Sequelae of Venous ThromboembolismDocument10 pagesEpidemiology, Risk Factors and Sequelae of Venous ThromboembolismCondurache Ilie-AndreiNo ratings yet
- Walkthrough by GamingratDocument98 pagesWalkthrough by GamingratCondurache Ilie-AndreiNo ratings yet
- Black Mirror S03E01 720p WEBRip DD5 1 x264-ITSatDocument66 pagesBlack Mirror S03E01 720p WEBRip DD5 1 x264-ITSatCondurache Ilie-AndreiNo ratings yet
- Exploring the history and culture of an ancient civilizationDocument12 pagesExploring the history and culture of an ancient civilizationCondurache Ilie-AndreiNo ratings yet
- Wa0005 PDFDocument45 pagesWa0005 PDFCondurache Ilie-AndreiNo ratings yet
- Walkthrough For PSP by DomZ Ninja - GameFAQsDocument93 pagesWalkthrough For PSP by DomZ Ninja - GameFAQsCondurache Ilie-AndreiNo ratings yet
- Read MeDocument1 pageRead Meanon_637749750No ratings yet
- Hiv MCQDocument89 pagesHiv MCQEliza Spark80% (5)
- Air Regulations CPL Level QuestionsDocument56 pagesAir Regulations CPL Level QuestionsRahul100% (3)
- Original Instruction Manual: Hypro Series 9303Document24 pagesOriginal Instruction Manual: Hypro Series 9303vandoNo ratings yet
- Antox Pickling Paste MSDSDocument10 pagesAntox Pickling Paste MSDSKrishna Vacha0% (1)
- Intellectual Property: Impact of Exhaustion of Intellectual Property Right On Pharmaceutical Industry in VietnamDocument26 pagesIntellectual Property: Impact of Exhaustion of Intellectual Property Right On Pharmaceutical Industry in VietnamSơn BadGuyNo ratings yet
- Design and Analysis of Cooling Fins: Deepak Gupta, Wankhade S.RDocument4 pagesDesign and Analysis of Cooling Fins: Deepak Gupta, Wankhade S.RAntonio SilvaNo ratings yet
- PGDHM SyllabusDocument34 pagesPGDHM SyllabusankushlmpNo ratings yet
- DIAGEO2Document12 pagesDIAGEO2Tatiana Zuleta RojasNo ratings yet
- O-Rings & SealsDocument10 pagesO-Rings & SealsPartsGopher.comNo ratings yet
- 01 PROT4xx PowerSystemFaults r4Document84 pages01 PROT4xx PowerSystemFaults r4Raul MistaNo ratings yet
- Commodity FuturesDocument19 pagesCommodity FuturesPrabhu G UmadiNo ratings yet
- Pdev 111 Week 1 20 1st SemesterDocument123 pagesPdev 111 Week 1 20 1st SemesterReyn TabelismaNo ratings yet
- Music Genre AnalysisDocument5 pagesMusic Genre AnalysisPeh Xin YingNo ratings yet
- Monica Stelly Resume 2017Document2 pagesMonica Stelly Resume 2017api-355097199No ratings yet
- Handout2 Fischer CarbeneDocument5 pagesHandout2 Fischer CarbeneMuhammad ShimaNo ratings yet
- 20190904020842HI Kobelco Tier 4 Final SK140SRL BrochureDocument2 pages20190904020842HI Kobelco Tier 4 Final SK140SRL BrochureAkhmad SebehNo ratings yet
- Higuey, Dom Rep Mdpc/Puj: .Eff.23.MayDocument5 pagesHiguey, Dom Rep Mdpc/Puj: .Eff.23.MayVanessa Yumayusa0% (1)
- Periodic Table of Personality ElementsDocument1 pagePeriodic Table of Personality Elementslilian_vera_1No ratings yet
- Physical Science - q3 - Slm3Document15 pagesPhysical Science - q3 - Slm3Boyet Alvarez AtibagosNo ratings yet
- Norris Claire White Paper Liftware PDFDocument14 pagesNorris Claire White Paper Liftware PDFmeysam NaaNo ratings yet
- Reduced Renal Sodium Excretion: Forced Through A Narrow LumenDocument5 pagesReduced Renal Sodium Excretion: Forced Through A Narrow LumenFlowerNo ratings yet
- Ethylene Glycol PDFDocument2 pagesEthylene Glycol PDFAngela0% (1)
- Chapter Test A: Teacher Notes and Answers 17Document5 pagesChapter Test A: Teacher Notes and Answers 17Mmf 123 JanNo ratings yet
- English Based On Latest PatternDocument13 pagesEnglish Based On Latest PatternAtish ToppoNo ratings yet
- Lab Report 1Document3 pagesLab Report 1CarlEspantoNo ratings yet
- Tips For Establish Ball Pen Refill PlantDocument5 pagesTips For Establish Ball Pen Refill PlantSingam Sridhar100% (1)
- CAP - 5 - 54. Billions and Billions of Demons - by Richard C. Lewontin - The New York Review of BooksDocument11 pagesCAP - 5 - 54. Billions and Billions of Demons - by Richard C. Lewontin - The New York Review of BooksRaimundo Filho100% (1)
- Screening Criteria For Application of EOR Processes in Offshore FieldsDocument7 pagesScreening Criteria For Application of EOR Processes in Offshore FieldsSajad FalahNo ratings yet
- (UNISIM (BEHAS) - Introduction To Aerospace) EAS105 - Lab4Document33 pages(UNISIM (BEHAS) - Introduction To Aerospace) EAS105 - Lab4Mohd Ashraf Mohd IsmailNo ratings yet
- Boiler BlowdownDocument2 pagesBoiler BlowdownbaratheonNo ratings yet