You might also like
- Shoulder DystociaDocument11 pagesShoulder DystociaYulvina IjieNo ratings yet
- Royaldystoci Shoulder 2012 (01-09) PDFDocument9 pagesRoyaldystoci Shoulder 2012 (01-09) PDFpaolaNo ratings yet
- Shoulder DystociaDocument9 pagesShoulder DystociaRorschach VargasNo ratings yet
- Referat Distosia Bahu ElfaDocument16 pagesReferat Distosia Bahu ElfaElfa RiniNo ratings yet
- Distosia Ncbi (Ana)Document8 pagesDistosia Ncbi (Ana)Ni Wayan Ana PsNo ratings yet
- Practice Bullet In: Shoulder DystociaDocument11 pagesPractice Bullet In: Shoulder DystociaMely GallardoNo ratings yet
- AIP Chap13 Shoulder DystociaDocument13 pagesAIP Chap13 Shoulder DystociaJeremia KurniawanNo ratings yet
- CervicalinsufficiencyDocument9 pagesCervicalinsufficiencyChinenye LovethNo ratings yet
- Management of Breech PresentationDocument13 pagesManagement of Breech Presentationdr.Hansen.SH100% (1)
- Guided by Hod and Proff. Dr. Ratna Thakur: Presented by Dr. Snehalata DR - Trina DR - SonalDocument28 pagesGuided by Hod and Proff. Dr. Ratna Thakur: Presented by Dr. Snehalata DR - Trina DR - Sonalkalpana gondipalliNo ratings yet
- VacumDocument16 pagesVacumGkpmi Ekklesia JayapuraNo ratings yet
- Guide to Breech Presentation DeliveryDocument13 pagesGuide to Breech Presentation DeliveryRahmawati Dianing PangestuNo ratings yet
- Risk Factors and Predictability of Shoulder DystociaDocument5 pagesRisk Factors and Predictability of Shoulder DystociaDaniel Ramirez QuintanaNo ratings yet
- PHD Buchmann TextDocument223 pagesPHD Buchmann TextRidski D. MiruNo ratings yet
- Shoulder DystociaDocument63 pagesShoulder Dystociaapi-3841435100% (3)
- Fetal Growth Velocity in Diabetics and The Risk For Shoulder Dystocia: A Case-Control StudyDocument6 pagesFetal Growth Velocity in Diabetics and The Risk For Shoulder Dystocia: A Case-Control Studyaulia ilmaNo ratings yet
- Shoulder Dystocia - ACOGDocument33 pagesShoulder Dystocia - ACOGGita PatelNo ratings yet
- StratOG Vaginal BreechDocument17 pagesStratOG Vaginal BreechNalin AbeysingheNo ratings yet
- Green Top Guidelines 11Document24 pagesGreen Top Guidelines 11garfield1No ratings yet
- Umbilical Cord ProlapseDocument4 pagesUmbilical Cord ProlapseYwagar Ywagar100% (1)
- Elective Primary Cesarean Delivery: Sounding BoardDocument6 pagesElective Primary Cesarean Delivery: Sounding BoardNicole Grace VillegasNo ratings yet
- RANZCOG Management of Breech PresentationDocument9 pagesRANZCOG Management of Breech PresentationKe XuNo ratings yet
- Shoulder DystociaDocument2 pagesShoulder DystociaManjiree KarandikarNo ratings yet
- WHO - Um Interventions For Preventing Shoulder DystociaDocument4 pagesWHO - Um Interventions For Preventing Shoulder Dystociavishramki2009No ratings yet
- Shoulder DystociaDocument8 pagesShoulder DystociaPorfirio MaciasNo ratings yet
- Overview#a8: Uterine Rupture in PregnancyDocument13 pagesOverview#a8: Uterine Rupture in PregnancyFadillaLovianaIrwanNo ratings yet
- Breech BirthDocument10 pagesBreech Birthcirlce:twoworldsconnectedNo ratings yet
- Articulo 6Document13 pagesArticulo 6Monica ReyesNo ratings yet
- Indication For CsDocument20 pagesIndication For CsSandiNo ratings yet
- Shoulder Dystocia: Diagnosis and Intervention: This Course Has Been Awarded Two (2.0) Contact HoursDocument26 pagesShoulder Dystocia: Diagnosis and Intervention: This Course Has Been Awarded Two (2.0) Contact HoursraimiNo ratings yet
- AnestesiDocument15 pagesAnestesiayang rasheldaNo ratings yet
- Anaesthesia For LSCS PDFDocument14 pagesAnaesthesia For LSCS PDFaksinuNo ratings yet
- Determinants and Obstetrics Outcome of Umbilical Cord Prolapse at University of Calabar Teaching Hospital, Calabar, NigeriaDocument6 pagesDeterminants and Obstetrics Outcome of Umbilical Cord Prolapse at University of Calabar Teaching Hospital, Calabar, NigeriaIOSRjournalNo ratings yet
- Hemorrgia Obstetrica 2020Document20 pagesHemorrgia Obstetrica 2020Carolina VargasNo ratings yet
- Prolonged PregnancyDocument41 pagesProlonged PregnancyPratiwi Anggun LestariningrumNo ratings yet
- Umbilical Cord Prolapse: Green-Top Guideline No. 50Document13 pagesUmbilical Cord Prolapse: Green-Top Guideline No. 50Nurul Aimi Abdul RahmanNo ratings yet
- Managing Delivery of TwinsDocument7 pagesManaging Delivery of TwinsRegina HershaaNo ratings yet
- Cephalopelvic Disproportion FinalDocument7 pagesCephalopelvic Disproportion FinalJesie Mel Bacena100% (1)
- Risk Factors for Uterine Rupture After CesareanDocument15 pagesRisk Factors for Uterine Rupture After CesareanSakena NurzaNo ratings yet
- Benign Breast Disorders+Document15 pagesBenign Breast Disorders+Fernando Peralta PalmezanoNo ratings yet
- EXTERNAL CEPHALIC VERSION AND REDUCING THE INCIDENCE OF Breech PDFDocument8 pagesEXTERNAL CEPHALIC VERSION AND REDUCING THE INCIDENCE OF Breech PDFrolla_hiraNo ratings yet
- C-Obs 38 Planned Vaginal Birth After C-Section New Jul 10Document7 pagesC-Obs 38 Planned Vaginal Birth After C-Section New Jul 10Aris SugiatnoNo ratings yet
- AIP Chap12 Vaginal Breech PDFDocument14 pagesAIP Chap12 Vaginal Breech PDFviaereaNo ratings yet
- DistosiaDocument12 pagesDistosiaIntan PermataNo ratings yet
- Shoulder DystociaDocument8 pagesShoulder DystociaMajo MelchiadeNo ratings yet
- b2 10 1Document9 pagesb2 10 1Tio Ayahnya AtharNo ratings yet
- Guidelines for Managing Shoulder DystociaDocument6 pagesGuidelines for Managing Shoulder DystociaNguyen HuyNo ratings yet
- Malignancies in Pregnancy Multiple 2016 Best Practice Research ClinicalDocument8 pagesMalignancies in Pregnancy Multiple 2016 Best Practice Research ClinicalorriNo ratings yet
- Scholarly LogDocument4 pagesScholarly Logapi-441649567No ratings yet
- ReadingDocument1 pageReadingFroo KeruNo ratings yet
- TOG Advanced Abdominal Pregnancy 2022Document10 pagesTOG Advanced Abdominal Pregnancy 2022MarNo ratings yet
- RCOG Guidelines - Gestational Trophoblastic DiseaseDocument12 pagesRCOG Guidelines - Gestational Trophoblastic Diseasemob3100% (1)
- Umbilical Cord ProlapseDocument5 pagesUmbilical Cord Prolapseangga hergaNo ratings yet
- BMJ 333 7579 Prac 01159Document4 pagesBMJ 333 7579 Prac 01159Neky KuntjoroNo ratings yet
- Prolonged PregnancyDocument40 pagesProlonged Pregnancyjan caraNo ratings yet
- Shoulder Dystocia and Birth Injury: Prevention and TreatmentFrom EverandShoulder Dystocia and Birth Injury: Prevention and TreatmentNo ratings yet
- Absolute Obstetric Anesthesia Review: The Complete Study Guide for Certification and RecertificationFrom EverandAbsolute Obstetric Anesthesia Review: The Complete Study Guide for Certification and RecertificationNo ratings yet
- Management of Labor and DeliveryFrom EverandManagement of Labor and DeliveryGeorge A. MaconesNo ratings yet
- Controversies in Diagnosis of Preterm LabourDocument3 pagesControversies in Diagnosis of Preterm Labourrolla_hiraNo ratings yet
- Twiss 2014Document6 pagesTwiss 2014rolla_hiraNo ratings yet
- Nut consumption may not lower hypertension riskDocument7 pagesNut consumption may not lower hypertension riskrolla_hiraNo ratings yet
- Acute Mastoiditis in ChildrenDocument8 pagesAcute Mastoiditis in Childrenrolla_hiraNo ratings yet
- Nut consumption may not lower hypertension riskDocument7 pagesNut consumption may not lower hypertension riskrolla_hiraNo ratings yet
- Intrauterine Infection and PrematurityDocument11 pagesIntrauterine Infection and Prematurityrolla_hiraNo ratings yet
- Hindmilk and Weight Gain in Preterm Very Low-Birthweight InfantsDocument5 pagesHindmilk and Weight Gain in Preterm Very Low-Birthweight Infantsrolla_hiraNo ratings yet
- Serum Ferritin in Term and Preterm InfantsDocument4 pagesSerum Ferritin in Term and Preterm Infantsrolla_hiraNo ratings yet
- Prematurity at Birth Trends RacialDocument6 pagesPrematurity at Birth Trends Racialrolla_hiraNo ratings yet
- Use of Oxygen in The Resuscitation of Preterm Infants CurrentDocument5 pagesUse of Oxygen in The Resuscitation of Preterm Infants Currentrolla_hiraNo ratings yet
- Current Understanding of Genetic Factors in Preterm BirthDocument4 pagesCurrent Understanding of Genetic Factors in Preterm Birthrolla_hiraNo ratings yet
- C 4Document41 pagesC 4rolla_hiraNo ratings yet
- Slide Adit Buat Teh EpoyDocument1 pageSlide Adit Buat Teh Epoyrolla_hiraNo ratings yet
- Tayangan Case 23 Maret 2009Document38 pagesTayangan Case 23 Maret 2009rolla_hiraNo ratings yet
- Clinics MyomasDocument221 pagesClinics Myomasfelix campos100% (3)
- Anemia Related Cancer GuidelineDocument19 pagesAnemia Related Cancer Guidelinerolla_hiraNo ratings yet
- No. 29. Chronic Hypertension in PregnancyDocument9 pagesNo. 29. Chronic Hypertension in Pregnancyrolla_hiraNo ratings yet
- Genetics ScreeningDocument30 pagesGenetics Screeningrolla_hiraNo ratings yet
- Anemia Related Cancer GuidelineDocument19 pagesAnemia Related Cancer Guidelinerolla_hiraNo ratings yet
- Uterine CA GuedileneDocument43 pagesUterine CA Guedilenerolla_hiraNo ratings yet
- Preeclampsia JOCC PDFDocument52 pagesPreeclampsia JOCC PDFindahsaviNo ratings yet
- Cervical ScreeningDocument31 pagesCervical Screeningrolla_hiraNo ratings yet
- Diagnosis and Management of Gestational Hypertension and Preeclampsia - SibaiDocument12 pagesDiagnosis and Management of Gestational Hypertension and Preeclampsia - SibaiHabibullah AlNo ratings yet
- Hypertension in PregnancyDocument16 pagesHypertension in Pregnancyrolla_hiraNo ratings yet
- Ovarian Ca Guideline PDFDocument40 pagesOvarian Ca Guideline PDFrolla_hiraNo ratings yet
- Nut consumption may not lower hypertension riskDocument7 pagesNut consumption may not lower hypertension riskrolla_hiraNo ratings yet
- Treatments For COPDDocument13 pagesTreatments For COPDrolla_hiraNo ratings yet
- Sonography of Adenomyosis: Sound Judgment SeriesDocument4 pagesSonography of Adenomyosis: Sound Judgment Seriesrolla_hiraNo ratings yet
- Human reproduction self-assessment questionsDocument2 pagesHuman reproduction self-assessment questionsEdyWidjajaNo ratings yet
- Research KhushiDocument7 pagesResearch KhushiMeet PatelNo ratings yet
- Acog Practice Bulletin Summary: Pregestational Diabetes MellitusDocument3 pagesAcog Practice Bulletin Summary: Pregestational Diabetes MellitusMaría Fernanda Palma AcostaNo ratings yet
- Obstetrics: Antenatal Care IncludesDocument11 pagesObstetrics: Antenatal Care Includesapi-3829364No ratings yet
- Science-10 Q3 Module-2 Week-2Document5 pagesScience-10 Q3 Module-2 Week-2Marl Rina EsperanzaNo ratings yet
- Ob / Gyn Nursing: by Group 1 Elfa Susanti Nurafianti OktamegaDocument11 pagesOb / Gyn Nursing: by Group 1 Elfa Susanti Nurafianti OktamegaRolli SptNo ratings yet
- Obstetrics & Gynecology 2019 Bases Krok 2 Explaned - Students AssistantDocument157 pagesObstetrics & Gynecology 2019 Bases Krok 2 Explaned - Students AssistantAbhinav VermaNo ratings yet
- Gannguan PubertasDocument56 pagesGannguan PubertasAde Yosdi PutraNo ratings yet
- Internal examination and cervical dilation processDocument2 pagesInternal examination and cervical dilation processJnana YumnaNo ratings yet
- Pregnancy W Std's ArticleDocument4 pagesPregnancy W Std's ArticleCharina AubreyNo ratings yet
- Obstetric Haemorrhage: EsmoeDocument43 pagesObstetric Haemorrhage: EsmoeLana LocoNo ratings yet
- Reproductive Endocrinology, by Prof - Dr.Vesna Antovska PHD 2023Document50 pagesReproductive Endocrinology, by Prof - Dr.Vesna Antovska PHD 2023Vesna AntovskaNo ratings yet
- Physiology of The Female Reproductive System: Liu Wei Department of Ob & Gy Ren Ji HospitalDocument24 pagesPhysiology of The Female Reproductive System: Liu Wei Department of Ob & Gy Ren Ji HospitalAmanuel MaruNo ratings yet
- Contraception Questions and Answers For PharmacistsDocument9 pagesContraception Questions and Answers For PharmacistsMohamed OmerNo ratings yet
- LACTATION Physiology and ManagementDocument37 pagesLACTATION Physiology and ManagementRed Williams0% (2)
- Tugas Mata Kuliah Bahasa Inggris: Dosen Pembimbing: A. M. Aziz, M. PDDocument4 pagesTugas Mata Kuliah Bahasa Inggris: Dosen Pembimbing: A. M. Aziz, M. PDMega Safira MahardiniNo ratings yet
- 3讲义ObestetricDocument104 pages3讲义Obestetricchongyu888xiongNo ratings yet
- Acog Committee Opinion: Cesarean Delivery On Maternal RequestDocument5 pagesAcog Committee Opinion: Cesarean Delivery On Maternal RequestfbihansipNo ratings yet
- ENGLISH VERSION - Lactation Teaching ToolsDocument15 pagesENGLISH VERSION - Lactation Teaching ToolsXiomara Salort100% (1)
- ASSESSMENT Reproductive SystemDocument3 pagesASSESSMENT Reproductive SystemJossie Allen PradoNo ratings yet
- The Role of Ultrasound in ObstetricsDocument9 pagesThe Role of Ultrasound in ObstetricsHanun FaizaNo ratings yet
- Cervical CerclageDocument21 pagesCervical Cerclagerolla_hiraNo ratings yet
- APH & PPH: Causes, Diagnosis and ManagementDocument81 pagesAPH & PPH: Causes, Diagnosis and ManagementSheilla ElfiraNo ratings yet
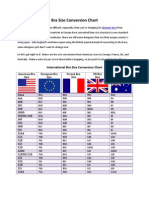
- Bra Size Conversion ChartDocument3 pagesBra Size Conversion ChartTop Drawer Lingerie100% (1)
- Practice Guidelines Acog Bulletin 102Document0 pagesPractice Guidelines Acog Bulletin 102Indah Puspita Sari PaneNo ratings yet
- Ovulation and FertilizationDocument2 pagesOvulation and FertilizationEarl CopeNo ratings yet
- High Risk Labour FinalDocument60 pagesHigh Risk Labour FinalSusan HepziNo ratings yet
- Preparation of Women in LabourDocument21 pagesPreparation of Women in LabourAbinaya RanganathanNo ratings yet
- Chemistry of Oral ContraceptivesDocument13 pagesChemistry of Oral ContraceptivesJuan Carlos UriarteNo ratings yet
- Module 8 Postpartum Stage Mercado Sibal IIIDocument13 pagesModule 8 Postpartum Stage Mercado Sibal IIIFrancisco Sibal IIINo ratings yet