You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (72)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Zakynthos - Greece enDocument32 pagesZakynthos - Greece ensilversurfer3100% (4)
- An Introduction To: Subsea CablesDocument12 pagesAn Introduction To: Subsea CablesJason GuthrieNo ratings yet
- Origin Destination Flight No. Aircraft Days of Departure Arrival Type Operation Time TimeDocument38 pagesOrigin Destination Flight No. Aircraft Days of Departure Arrival Type Operation Time Timekulkarni68No ratings yet
- Astero E0201E-20 991063Document186 pagesAstero E0201E-20 991063Thinh Nguyen100% (1)
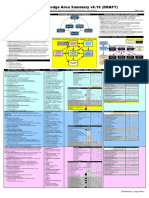
- Babok v3 Knowledge Area Summary v0.15 (DRAFT)Document2 pagesBabok v3 Knowledge Area Summary v0.15 (DRAFT)vkcon100% (1)
- Chapter 12: Media Access Control (MAC)Document66 pagesChapter 12: Media Access Control (MAC)soumyaNo ratings yet
- Indian Association For Management Development Accredited A' Grade by NAACDocument8 pagesIndian Association For Management Development Accredited A' Grade by NAACTejas DesaiNo ratings yet
- Historicizing Rappaport's Pigs For The AncestorsDocument29 pagesHistoricizing Rappaport's Pigs For The AncestorsObservador20No ratings yet
- Medieval Women Artists and Modem HistoriansDocument11 pagesMedieval Women Artists and Modem HistoriansDeniss Dominguez CervantesNo ratings yet
- M.A Chaudary Greenhall OL Physics NotesDocument139 pagesM.A Chaudary Greenhall OL Physics NotesArshad KhanNo ratings yet
- Subject: Biochemistry Topic:Lipid Metabolism 2 Lecturer: Dr. Laygo DATE: NOV. 2010Document11 pagesSubject: Biochemistry Topic:Lipid Metabolism 2 Lecturer: Dr. Laygo DATE: NOV. 2010Std DlshsiNo ratings yet
- Assessment Form 10 (Collection and Analysis of Quantitative and Qualitative Data) 3Document8 pagesAssessment Form 10 (Collection and Analysis of Quantitative and Qualitative Data) 3Raymond RamirezNo ratings yet
- Contract of Lease - Knoxport 2024 (Sept-Feb)Document8 pagesContract of Lease - Knoxport 2024 (Sept-Feb)Lexter Owen ApeladoNo ratings yet
- A320 Flow PatternDocument18 pagesA320 Flow PatternFritz Carlo MagpantayNo ratings yet
- Microzed-A V Microzed-A V3.1 3.1: User'S ManualDocument38 pagesMicrozed-A V Microzed-A V3.1 3.1: User'S ManualWassim Baccari100% (1)
- Engine 1Document8 pagesEngine 1minhgiapleNo ratings yet
- Rich Text Editor For MediaWiki (Berlin, April 2010)Document16 pagesRich Text Editor For MediaWiki (Berlin, April 2010)Inez_KorczyńskiNo ratings yet
- LESSON PLAN Reading (Unit 2: SpoDocument6 pagesLESSON PLAN Reading (Unit 2: SpoSoffea RahimNo ratings yet
- RBI Master Circular on Management of Advances for UCBsDocument57 pagesRBI Master Circular on Management of Advances for UCBsashwini.krs80No ratings yet
- BE 510 Business Economics 1 Problem Set 5 SolutionsDocument5 pagesBE 510 Business Economics 1 Problem Set 5 SolutionsCreative Work21stNo ratings yet
- MC3000 Charger Manual (English V1.12)Document22 pagesMC3000 Charger Manual (English V1.12)x3350No ratings yet
- BSR 512: Topic 2: Norehan Haji Mohd Noor Senior Lecturer Program of Building Surveying, Uitm PerakDocument35 pagesBSR 512: Topic 2: Norehan Haji Mohd Noor Senior Lecturer Program of Building Surveying, Uitm PerakaremyulNo ratings yet
- Letter From Mayor Stoney Requesting Data For Phase OneDocument2 pagesLetter From Mayor Stoney Requesting Data For Phase OneWTVR CBS 6100% (1)
- Universiti Tun Hussein Onn Malaysia Faculty of Mechanical and Manufacturing EngineeringDocument10 pagesUniversiti Tun Hussein Onn Malaysia Faculty of Mechanical and Manufacturing EngineeringAriff AliNo ratings yet
- What Is A Risk Assessment?Document7 pagesWhat Is A Risk Assessment?Mohamad Yusof0% (1)
- READING 8 Free Cashflow (Equity Valuation)Document25 pagesREADING 8 Free Cashflow (Equity Valuation)DandyNo ratings yet
- Quality: PerformsDocument21 pagesQuality: PerformsJérémy BELLISSENTNo ratings yet
- Wireless TechhnologyDocument16 pagesWireless TechhnologyAhmad Raza AnsariNo ratings yet
- Microsoft Outlook - How To Avoid Sending Winmail - Dat FileDocument1 pageMicrosoft Outlook - How To Avoid Sending Winmail - Dat FileGoran DonićNo ratings yet
- DLL NAIL CARE - Basic ConceptsDocument5 pagesDLL NAIL CARE - Basic ConceptsChé Ché JavierNo ratings yet