You might also like
- Pathophysiology of Myocardial Infarction (STEMI)Document2 pagesPathophysiology of Myocardial Infarction (STEMI)michaela100% (3)
- Multiple Organ Dysfunction SyndromeDocument31 pagesMultiple Organ Dysfunction SyndromeIbrahim Akinbola100% (1)
- Pneumothorax (Collapsed Lung)Document34 pagesPneumothorax (Collapsed Lung)james garcia100% (3)
- Chest TraumaDocument9 pagesChest Traumaapi-3838240100% (7)
- Science: Quarter 2 - Module 1Document20 pagesScience: Quarter 2 - Module 1Kate BatacNo ratings yet
- COPD PathoDocument1 pageCOPD PathoLeah May AnchetaNo ratings yet
- Liver Cirrhosis: (Alterations in Metabolic and Endocrine Functions)Document8 pagesLiver Cirrhosis: (Alterations in Metabolic and Endocrine Functions)Jorie RocoNo ratings yet
- Acute Respiratory Distress SyndromeDocument31 pagesAcute Respiratory Distress Syndromegretchen marie100% (1)
- Coronary Artery Disease PathophysiologyDocument3 pagesCoronary Artery Disease PathophysiologyElmer Balgos Alinsog50% (4)
- Cardiogenic ShockDocument21 pagesCardiogenic ShockIslamOteshNo ratings yet
- Nursing TheoriesDocument51 pagesNursing TheoriesJorie RocoNo ratings yet
- Myocardial Infarction Pathophysiology & Schematic DiagramDocument3 pagesMyocardial Infarction Pathophysiology & Schematic DiagramJessica Peñamora100% (1)
- Pathophysiology of Appendicitis and its ComplicationsDocument4 pagesPathophysiology of Appendicitis and its ComplicationsAngelica Cassandra VillenaNo ratings yet
- The Teacher's Role and ResponsibilitiesDocument7 pagesThe Teacher's Role and ResponsibilitiesJorie RocoNo ratings yet
- Adel Elkady Sba PDFDocument290 pagesAdel Elkady Sba PDFAsh Ame100% (2)
- Right-Sided Heart FailureDocument4 pagesRight-Sided Heart FailureKhalid Mahmud ArifinNo ratings yet
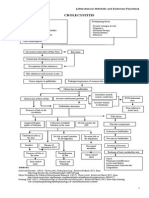
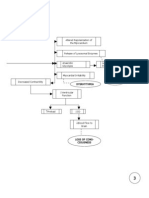
- Cholecystitis: (Alterations in Metabolic and Endocrine Functions)Document4 pagesCholecystitis: (Alterations in Metabolic and Endocrine Functions)Jorie RocoNo ratings yet
- Measures of SkewnessDocument15 pagesMeasures of SkewnessJorie Roco100% (1)
- Myocardial Infarction Pathophysiology ExplainedDocument3 pagesMyocardial Infarction Pathophysiology ExplainedAbi Habiling100% (3)
- Chronic Obstructive Pulmonary Disease (COPD)Document32 pagesChronic Obstructive Pulmonary Disease (COPD)matrixtrinityNo ratings yet
- Symptoms of Low PotassiumDocument3 pagesSymptoms of Low PotassiumCharlene Mae Calanoy100% (1)
- Group-1b Myocardial InfarctionDocument39 pagesGroup-1b Myocardial InfarctionJean ReyesNo ratings yet
- Dilated Cardiomyopathy Case StudyDocument29 pagesDilated Cardiomyopathy Case Studydvalitz100% (2)
- Iv. Pathophysiology 1. Schematic Diagram Book Based Pathophysiology: Precipitating/Modifiable Factors Non Modifiable / Predisposing FactorsDocument2 pagesIv. Pathophysiology 1. Schematic Diagram Book Based Pathophysiology: Precipitating/Modifiable Factors Non Modifiable / Predisposing Factorsikemas67% (6)
- Pathophysiology of CVADocument1 pagePathophysiology of CVAChristine Joy Ilao PasnoNo ratings yet
- ARDS With PathophysiologyDocument79 pagesARDS With Pathophysiologymabec pagaduan95% (19)
- Pathophysiology of StrokeDocument3 pagesPathophysiology of StrokeAqeel Al-Mahdaly0% (1)
- Acute Respiratory FailureDocument2 pagesAcute Respiratory FailurePaolo Luis MontenegroNo ratings yet
- Congestive Heart Failure Schematic DiagramDocument1 pageCongestive Heart Failure Schematic DiagramCyrus De Asis100% (1)
- Pathophysiology of Malignant Pleural Effusion Due to Breast Cancer MetastasisDocument1 pagePathophysiology of Malignant Pleural Effusion Due to Breast Cancer Metastasisfaula rocamora80% (5)
- Acute Respiratory Distress SyndromeDocument17 pagesAcute Respiratory Distress SyndromeSanjeet SahNo ratings yet
- Pulmonary EdemaDocument59 pagesPulmonary EdemamaibejoseNo ratings yet
- Ards Cmap FinalDocument4 pagesArds Cmap FinalPam Araune67% (3)
- Advanced Statistics ReviewDocument21 pagesAdvanced Statistics ReviewJorie RocoNo ratings yet
- StaffingDocument50 pagesStaffingPradeep PandaNo ratings yet
- DCM - Heart Failure Due to Dilated CardiomyopathyDocument13 pagesDCM - Heart Failure Due to Dilated CardiomyopathyPrincysuzine PintoNo ratings yet
- Acute Respiratory Distress Syndrome - PathophysiologyDocument5 pagesAcute Respiratory Distress Syndrome - PathophysiologyJoann67% (3)
- Pancreatitis: (Alterations in Metabolic and Endocrine Functions)Document7 pagesPancreatitis: (Alterations in Metabolic and Endocrine Functions)Jorie Roco0% (1)
- Patho (Lung Cancer)Document1 pagePatho (Lung Cancer)k.n.e.d.No ratings yet
- Pathophysiology ARDSDocument1 pagePathophysiology ARDSRoderick Agbuya100% (1)
- Pathophysiology of Septic Shock Draft 1Document1 pagePathophysiology of Septic Shock Draft 1Ju Lie AnnNo ratings yet
- Pathophysiology of Bronchial AsthmaDocument2 pagesPathophysiology of Bronchial AsthmaFirenze Fil100% (21)
- Acute Respiratory Failure Pa Tho PhysiologyDocument4 pagesAcute Respiratory Failure Pa Tho Physiologyroseanne18100% (4)
- Asthma PathophysiologyDocument4 pagesAsthma PathophysiologyCee SanchezNo ratings yet
- English Assessment Physiotherapy & History Taking Dialogue EnglishDocument4 pagesEnglish Assessment Physiotherapy & History Taking Dialogue EnglishRobby FahrezaNo ratings yet
- Ecart Medications and EquipmentDocument9 pagesEcart Medications and EquipmentJan Philippe BelandoNo ratings yet
- Transpersonal CaringDocument46 pagesTranspersonal CaringJorie Roco100% (1)
- Pulmonary EmbolismDocument8 pagesPulmonary EmbolismspoilttbrattNo ratings yet
- Soft Tissue Biology Around Dental ImplantsDocument76 pagesSoft Tissue Biology Around Dental Implantsaakankshakanwar0% (2)
- Abdominoperineal Resection MilesDocument17 pagesAbdominoperineal Resection MilesHugoNo ratings yet
- Pneumonia PathophysiologyDocument1 pagePneumonia PathophysiologyDee Sarajan100% (3)
- Pathophysiology Acute Respiratory FailureDocument2 pagesPathophysiology Acute Respiratory FailureKimberly Regacho88% (8)
- PneumoniaDocument1 pagePneumoniaAyen FornollesNo ratings yet
- Pathophysiology of AtherosclerosisDocument1 pagePathophysiology of AtherosclerosisAzrul Hakim100% (2)
- Pneumonia Case Study: Toddler Diagnosis and TreatmentDocument5 pagesPneumonia Case Study: Toddler Diagnosis and TreatmentcrisolandNo ratings yet
- Bronchiectasis PathophysiologyDocument1 pageBronchiectasis PathophysiologyRayne Dunstan Pascual VergaraNo ratings yet
- pg1-33 of Pneumothorax Case StudyDocument36 pagespg1-33 of Pneumothorax Case StudyikemasNo ratings yet
- Patho Pleural EffusionDocument2 pagesPatho Pleural EffusionJess Prodigo50% (2)
- CASE STUDY-Heart FailureDocument4 pagesCASE STUDY-Heart FailureSarra Mood ImanNo ratings yet
- Drug Study in PneumoniaDocument17 pagesDrug Study in PneumoniaKara Kathrina FuentesNo ratings yet
- Pleural Effusion Case StudyDocument5 pagesPleural Effusion Case Studyjanice ianNo ratings yet
- PathophysiologyDocument2 pagesPathophysiologyKarla Karina Dela CruzNo ratings yet
- Myocardial Infarction Risk Factors and ComplicationsDocument4 pagesMyocardial Infarction Risk Factors and ComplicationsHearty ArriolaNo ratings yet
- Myocardial InfarctionDocument18 pagesMyocardial InfarctionYanna Habib-MangotaraNo ratings yet
- Nursing Diagnosis: Impaired Gas ExchangeDocument4 pagesNursing Diagnosis: Impaired Gas ExchangeShen Paril0% (1)
- Human Diseases Case Study 18 ADocument4 pagesHuman Diseases Case Study 18 Aairickann100% (1)
- Copd Health TeachingDocument2 pagesCopd Health TeachingMel Sevilla100% (1)
- Lung CancerDocument4 pagesLung CancerKrizia TepootNo ratings yet
- Cardiomyopathy Dilated CardiomyopathyDocument5 pagesCardiomyopathy Dilated Cardiomyopathym3d1k100% (1)
- Acute Respiratory Failure 1Document7 pagesAcute Respiratory Failure 1Trish 0019No ratings yet
- Pathophysiology of Respiratory FailureDocument6 pagesPathophysiology of Respiratory FailurevidagurlNo ratings yet
- Acute Respiratory Distress Syndrome in Near DrowningDocument30 pagesAcute Respiratory Distress Syndrome in Near DrowningJane SharpsNo ratings yet
- Acute Respiratory Distress SyndromeDocument3 pagesAcute Respiratory Distress SyndromedindayantNo ratings yet
- Risk factors for respiratory failureDocument7 pagesRisk factors for respiratory failureMaria FriskaNo ratings yet
- Noncardiogenic Pumonary EdemaDocument15 pagesNoncardiogenic Pumonary EdemaAnonymous OlS0WZwNo ratings yet
- Pediatric Acute Respiratory Distress SyndromeDocument2 pagesPediatric Acute Respiratory Distress SyndromeTry Febriani SiregarNo ratings yet
- BioethicsDocument31 pagesBioethicsJorie RocoNo ratings yet
- Critical Thinking PointersDocument40 pagesCritical Thinking PointersJorie RocoNo ratings yet
- Cover Page Nursing ManualDocument1 pageCover Page Nursing ManualJorie RocoNo ratings yet
- Measures of LocationDocument9 pagesMeasures of LocationJorie RocoNo ratings yet
- Case Study ProposalDocument4 pagesCase Study ProposalJorie RocoNo ratings yet
- Chapter 1Document5 pagesChapter 1Jorie RocoNo ratings yet
- Approval Sheet SampleDocument1 pageApproval Sheet SampleJorie RocoNo ratings yet
- Jean Watson's Theory of Transpersonal CaringDocument24 pagesJean Watson's Theory of Transpersonal CaringJorie RocoNo ratings yet
- Table of ContentsDocument2 pagesTable of ContentsJorie RocoNo ratings yet
- Hypos TestingDocument192 pagesHypos TestingJorie RocoNo ratings yet
- Kinds of Data PresentationDocument18 pagesKinds of Data PresentationJorie RocoNo ratings yet
- Measures of LocationDocument9 pagesMeasures of LocationJorie RocoNo ratings yet
- Kinds of Data PresentationDocument18 pagesKinds of Data PresentationJorie RocoNo ratings yet
- Overview of SpssDocument49 pagesOverview of SpssJorie RocoNo ratings yet
- Summary StatisticsDocument28 pagesSummary StatisticsJorie RocoNo ratings yet
- Survey Hema OncoDocument1 pageSurvey Hema OncoJorie RocoNo ratings yet
- SurveyDocument38 pagesSurveyJorie RocoNo ratings yet
- J1 Lecture 1 A Stimulus To DefineDocument6 pagesJ1 Lecture 1 A Stimulus To DefineJorie RocoNo ratings yet
- Nursing Administration PowepointDocument27 pagesNursing Administration PowepointJorie RocoNo ratings yet
- Saint Paul University Dumaguete Graduate School: Master of Science in NursingDocument5 pagesSaint Paul University Dumaguete Graduate School: Master of Science in NursingJorie RocoNo ratings yet
- Objectives For Hospital ExperienceDocument5 pagesObjectives For Hospital ExperienceJorie RocoNo ratings yet
- Propofol Infusion SyndromeDocument7 pagesPropofol Infusion SyndromewadejackNo ratings yet
- Drug Study Quinine SulfateDocument7 pagesDrug Study Quinine SulfateKathlyn_Matic_6376No ratings yet
- Teaching Project - BPDocument22 pagesTeaching Project - BPapi-283482759No ratings yet
- CEMONCDocument10 pagesCEMONCApril GuiangNo ratings yet
- MODUL 1 FKG UnairDocument61 pagesMODUL 1 FKG UnairLaurensia NovenNo ratings yet
- Advancesinlocal Anesthesiain Dentistry: Orrett E. Ogle,, Ghazal MahjoubiDocument19 pagesAdvancesinlocal Anesthesiain Dentistry: Orrett E. Ogle,, Ghazal Mahjoubicarlos gilbertoNo ratings yet
- FOR35 5crAB06 PDFDocument32 pagesFOR35 5crAB06 PDFFleRexNo ratings yet
- Hubungan Antara Abdominal Perfusion Pressure: (App) Dengan Outcome Post OperasiDocument17 pagesHubungan Antara Abdominal Perfusion Pressure: (App) Dengan Outcome Post OperasidrelvNo ratings yet
- Management of The Urologic Sepsis SyndromeDocument10 pagesManagement of The Urologic Sepsis SyndromeNur Syamsiah MNo ratings yet
- Laporan Diet Pasca BedahDocument13 pagesLaporan Diet Pasca BedahYuliza RosalinaNo ratings yet
- Anxiety and Depression in TeensDocument2 pagesAnxiety and Depression in TeensHenry Alexander Gerena SalazarNo ratings yet
- How China Is Fighting HIV/AIDS Stigma (Wang Longde)Document22 pagesHow China Is Fighting HIV/AIDS Stigma (Wang Longde)National Press FoundationNo ratings yet
- Name_Naw Aung_La Mai Patient Focused ProceduresDocument2 pagesName_Naw Aung_La Mai Patient Focused ProceduresEileenNo ratings yet
- Hyper-Reflexia in Guillain - Barré Syndrome: Systematic ReviewDocument7 pagesHyper-Reflexia in Guillain - Barré Syndrome: Systematic ReviewVladimir BasurtoNo ratings yet
- Daftar PustakaDocument6 pagesDaftar PustakaChintiaNo ratings yet
- Tara's Intro To Critical CareDocument6 pagesTara's Intro To Critical CareTara McNeillNo ratings yet
- Nursing Care Plan: Change in Health Status As Evidence by Excessive Shaking After 1hour, The Patient Will Be Able ToDocument1 pageNursing Care Plan: Change in Health Status As Evidence by Excessive Shaking After 1hour, The Patient Will Be Able ToVoid LessNo ratings yet
- StomatitisDocument74 pagesStomatitisZahoor ZaidiNo ratings yet
- Consent Form Nephrology BHUDocument6 pagesConsent Form Nephrology BHURajeshKumarJainNo ratings yet
- Perinatal Factor Journal PediatricDocument8 pagesPerinatal Factor Journal PediatricHasya KinasihNo ratings yet
- Nutrients: Anemia of Chronic Diseases: Wider Diagnostics-Better Treatment?Document17 pagesNutrients: Anemia of Chronic Diseases: Wider Diagnostics-Better Treatment?Gufront MustofaNo ratings yet
- Live Donor Liver Transplantation: Caq CornerDocument12 pagesLive Donor Liver Transplantation: Caq CornerBarbara ZabraNo ratings yet
- Aubf Module 3 Laboratory Assignment - Macabanding - PrincessDocument5 pagesAubf Module 3 Laboratory Assignment - Macabanding - PrincessNailah MacabandingNo ratings yet