You might also like
- Marijuana Legalization (Copypasta Pastiche)Document4 pagesMarijuana Legalization (Copypasta Pastiche)LeEminenceGriseNo ratings yet
- Medical Marijuana OverviewDocument2 pagesMedical Marijuana OverviewMPP0% (1)
- Position Paper On Marijuana As MedicineDocument4 pagesPosition Paper On Marijuana As Medicinenetmail2307100% (1)
- Medical Marijuana PowerpointDocument71 pagesMedical Marijuana PowerpointPagulayan Natividad Aljan100% (1)
- Why Marijuana Should Not Be LegalizedDocument7 pagesWhy Marijuana Should Not Be LegalizedomondistepNo ratings yet
- Colorado: The Economy After Legalization and RegulationDocument2 pagesColorado: The Economy After Legalization and RegulationMPPNo ratings yet
- Legalization of Medical Marijuana in The PhilippinesDocument114 pagesLegalization of Medical Marijuana in The PhilippinesJed Daet71% (38)
- Argument Essay FinaleDocument4 pagesArgument Essay Finaleapi-458895222No ratings yet
- Why Marijuana Should Be LegalDocument62 pagesWhy Marijuana Should Be LegalRenato Ferraz100% (40)
- Marijuana Research PaperDocument11 pagesMarijuana Research PaperJack DohertyNo ratings yet
- Marijuana Research PaperDocument12 pagesMarijuana Research PaperTianna100% (1)
- An Argumentative Essay On The Use of Marijuana in MedicineDocument6 pagesAn Argumentative Essay On The Use of Marijuana in MedicineSeth Andrew Salih100% (11)
- Final Research Paper - Marijuana LegalizationDocument10 pagesFinal Research Paper - Marijuana LegalizationSaberUmbra92% (13)
- Legalizing Marijuana for Medical and Recreational UseDocument6 pagesLegalizing Marijuana for Medical and Recreational UseAlyssa HilliardNo ratings yet
- Medical MarijuanaDocument5 pagesMedical Marijuanaapi-322399513No ratings yet
- Cannabis Legalization EssayDocument3 pagesCannabis Legalization Essayriley1987No ratings yet
- Argumentative Essay Medical MarijuanaDocument7 pagesArgumentative Essay Medical MarijuanaMaxim Dahan100% (1)
- Case Study: Legalization of MarijuanaDocument22 pagesCase Study: Legalization of MarijuanaIvyBautista100% (2)
- Medical Marijuana Legalization ImpactDocument55 pagesMedical Marijuana Legalization ImpactSusana G. Bencio100% (2)
- Medicinal Cannabis BriefingDocument32 pagesMedicinal Cannabis BriefingMiguelSantaellaSerranoNo ratings yet
- Medical Marijuana Protections in The 50 StatesDocument14 pagesMedical Marijuana Protections in The 50 StatesMPPNo ratings yet
- Summary of Medical Marijuana LawsDocument36 pagesSummary of Medical Marijuana LawsMPP100% (2)
- MarijuanaDocument8 pagesMarijuanajohnkyleNo ratings yet
- Marijuanaandlaw FinalDocument11 pagesMarijuanaandlaw Finalapi-283892872No ratings yet
- (FINAL) Legalization of Medical Marijuana Affirmative SpeechDocument5 pages(FINAL) Legalization of Medical Marijuana Affirmative SpeechKaye SantosNo ratings yet
- Top 10 Pros and Cons - Medical Marijuana - ProConDocument5 pagesTop 10 Pros and Cons - Medical Marijuana - ProConNews-Press100% (1)
- 11th Grade Persuausive Essay ExampleDocument2 pages11th Grade Persuausive Essay ExampleLindsay LigonesNo ratings yet
- What Is Medical Marijuana?Document11 pagesWhat Is Medical Marijuana?ZAARA ADAMSNo ratings yet
- Medical Marijuana Is Not Regulated As Most Medicines AreDocument3 pagesMedical Marijuana Is Not Regulated As Most Medicines AreElmy GarciaNo ratings yet
- Why Medical Marijuana Should Be LegalizedDocument5 pagesWhy Medical Marijuana Should Be LegalizedMarkNo ratings yet
- Guide To Cannabis For Chronic Pain Patients in EuropeDocument28 pagesGuide To Cannabis For Chronic Pain Patients in EuropeMilosNo ratings yet
- Marijuana and Medicine: Assessing The Science BaseDocument4 pagesMarijuana and Medicine: Assessing The Science BaseMPPNo ratings yet
- Revised Should Marijuana Be Legalized in The USDocument24 pagesRevised Should Marijuana Be Legalized in The USBailey DeitchNo ratings yet
- Final Paper WordDocument8 pagesFinal Paper Wordapi-357159376No ratings yet
- Legalization of Medical Marijuana in the USDocument12 pagesLegalization of Medical Marijuana in the USTeresa SmithNo ratings yet
- Should Marijuana Be Legal For Medicinal PurposesDocument2 pagesShould Marijuana Be Legal For Medicinal PurposesMOHD FITRI SAIMINo ratings yet
- Medical Marijuana: Benefits, Risks & State Laws: Understanding Marijuana: A New Look at The Scientific EvidenceDocument7 pagesMedical Marijuana: Benefits, Risks & State Laws: Understanding Marijuana: A New Look at The Scientific EvidenceLynette CantosNo ratings yet
- House OKs Medical Marijuana BillDocument3 pagesHouse OKs Medical Marijuana BillJennifer Garcia EreseNo ratings yet
- DPA - Fact Sheet - Medical - Marijuana - Jan2015 PDFDocument3 pagesDPA - Fact Sheet - Medical - Marijuana - Jan2015 PDFwebmaster@drugpolicy.orgNo ratings yet
- MMJ-BriefingPaper 0210Document4 pagesMMJ-BriefingPaper 0210toddler1100% (1)
- Is Marijuana Good or BadDocument2 pagesIs Marijuana Good or BadDana MocanuNo ratings yet
- Pain BrochureDocument24 pagesPain Brochurelordhavok33No ratings yet
- Keywords: Ailments, Availability and Legality, Aware, Epilepsy, High, KnowledgeableDocument18 pagesKeywords: Ailments, Availability and Legality, Aware, Epilepsy, High, KnowledgeablePatrick DgNo ratings yet
- Rhetorical Analysis Final DraftDocument5 pagesRhetorical Analysis Final Draftapi-643343018No ratings yet
- NY Physicians For Comp Care - Letter About Smoking - 06 05 2014Document3 pagesNY Physicians For Comp Care - Letter About Smoking - 06 05 2014samueloakford100% (1)
- Medical Marijuana as an Alternative to Prescription MedicationsDocument10 pagesMedical Marijuana as an Alternative to Prescription MedicationsMarcellaNo ratings yet
- The Benefits of Medical Marijuana For Cancer PatientsDocument4 pagesThe Benefits of Medical Marijuana For Cancer PatientsSheryl DiazNo ratings yet
- Cannabis DocumentationDocument20 pagesCannabis DocumentationRicardo CampuzanoNo ratings yet
- 5 Diseases Proven To Respond Better To Cannabis Than Prescription DrugsDocument12 pages5 Diseases Proven To Respond Better To Cannabis Than Prescription DrugsJames BondNo ratings yet
- Complementary Therapies in Medicine: Yuval Zolotov, Lia Eshet, Ofir MoragDocument5 pagesComplementary Therapies in Medicine: Yuval Zolotov, Lia Eshet, Ofir MoragRafael MouraNo ratings yet
- Research Paper 1Document6 pagesResearch Paper 1api-406728189No ratings yet
- Legalization Medical Marijuana Annotated Bibliography FINALDocument9 pagesLegalization Medical Marijuana Annotated Bibliography FINALRyan BloomNo ratings yet
- Medical Marijuana Research Paper ConclusionDocument6 pagesMedical Marijuana Research Paper Conclusionh02ver8h100% (1)
- Dr. A. Hazekamp Self-Medication With CannabisDocument39 pagesDr. A. Hazekamp Self-Medication With CannabisEl'Nelu Weed100% (2)
- Causal ArgumentDocument5 pagesCausal Argumentapi-471011232No ratings yet
- Physician Guide To Cannabis-Assisted Opioid Reduction (Distributed by EB)Document2 pagesPhysician Guide To Cannabis-Assisted Opioid Reduction (Distributed by EB)Lisa Rough100% (6)
- Medical Marijuana - GI BrochureDocument13 pagesMedical Marijuana - GI Brochure420100% (8)
- Reiman Et Al 2017 Cannabis As A Substitute For Opioid Based Pain Medication Patient Self ReportDocument7 pagesReiman Et Al 2017 Cannabis As A Substitute For Opioid Based Pain Medication Patient Self ReportfelipepretelmktNo ratings yet
- Medical Marijuana - Arthritis BrochureDocument13 pagesMedical Marijuana - Arthritis Brochure420100% (7)
- Petition Urging Governors To Protect Medical Cannabis AccessDocument70 pagesPetition Urging Governors To Protect Medical Cannabis AccessMPPNo ratings yet
- MPP Policy Paper - Regulating Cannabis Oil VaporizersDocument7 pagesMPP Policy Paper - Regulating Cannabis Oil VaporizersMPPNo ratings yet
- 2020 Vermont Poll ResultsDocument7 pages2020 Vermont Poll ResultsMPPNo ratings yet
- Decriminalization and Expungement in NY: An Overview of A0840 / S06579Document1 pageDecriminalization and Expungement in NY: An Overview of A0840 / S06579MPPNo ratings yet
- Medical Cannabis Provides An Alternative To OpiatesDocument1 pageMedical Cannabis Provides An Alternative To OpiatesMPPNo ratings yet
- GQR Connecticut Poll January 2020Document1 pageGQR Connecticut Poll January 2020MPPNo ratings yet
- Marijuana Policy Progress Report 2019 Legislative UpdateDocument28 pagesMarijuana Policy Progress Report 2019 Legislative UpdateMPP100% (3)
- Medical Cannabis Implementation TimelinesDocument10 pagesMedical Cannabis Implementation TimelinesMPPNo ratings yet
- Potential Revenue From Regulating Marijuana in ConnecticutDocument2 pagesPotential Revenue From Regulating Marijuana in ConnecticutMPPNo ratings yet
- Marijuana Policy Map May 2020Document1 pageMarijuana Policy Map May 2020MPPNo ratings yet
- Simon Poll March 2019Document14 pagesSimon Poll March 2019MPPNo ratings yet
- 2018 SIU Paul Simon Public Policy Institute Legalization PollDocument4 pages2018 SIU Paul Simon Public Policy Institute Legalization PollMPPNo ratings yet
- Medical Marijuana MapDocument1 pageMedical Marijuana MapMPPNo ratings yet
- Severe Pain and Medical CannabisDocument1 pageSevere Pain and Medical CannabisMPPNo ratings yet
- Prescribing Versus Recommending Medical CannabisDocument2 pagesPrescribing Versus Recommending Medical CannabisMPPNo ratings yet
- Maryland Progress ReportDocument2 pagesMaryland Progress ReportMPPNo ratings yet
- 2017 SIU Paul Simon Public Policy Institute Legalization PollDocument7 pages2017 SIU Paul Simon Public Policy Institute Legalization PollMPPNo ratings yet
- U.S. Attorneys' Comments Post Cole Memo RecissionDocument8 pagesU.S. Attorneys' Comments Post Cole Memo RecissionMPPNo ratings yet
- Breakdown of Taxes in Adult-Use StatesDocument2 pagesBreakdown of Taxes in Adult-Use StatesMPPNo ratings yet
- What Does Former AG Sessions' Marijuana Enforcement Memo Mean in Practice?Document2 pagesWhat Does Former AG Sessions' Marijuana Enforcement Memo Mean in Practice?MPPNo ratings yet
- Progress Report New York Medical Marijuana ProgramDocument2 pagesProgress Report New York Medical Marijuana ProgramMPPNo ratings yet
- Sessions Asks Congress To Undo Medical Marijuana ProtectionsDocument3 pagesSessions Asks Congress To Undo Medical Marijuana ProtectionsMPPNo ratings yet
- Expungement: Removing The Life-Long Stigma Caused by Marijuana ProhibitionDocument1 pageExpungement: Removing The Life-Long Stigma Caused by Marijuana ProhibitionMPPNo ratings yet
- New Jersey Progress ReportDocument2 pagesNew Jersey Progress ReportMPPNo ratings yet
- D.C.'s Medical Marijuana ProgramDocument2 pagesD.C.'s Medical Marijuana ProgramMPPNo ratings yet
- Medical Marijuana by The NumbersDocument2 pagesMedical Marijuana by The NumbersMPPNo ratings yet
- Breakdown of Fees in Adult-Use StatesDocument6 pagesBreakdown of Fees in Adult-Use StatesMPPNo ratings yet
- Safe, Legal Access To Marijuana Can Help Fight The Opioid EpidemicDocument1 pageSafe, Legal Access To Marijuana Can Help Fight The Opioid EpidemicMPPNo ratings yet
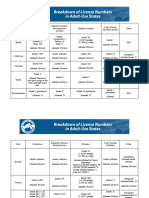
- Breakdown of License Numbers in Adult-Use StatesDocument2 pagesBreakdown of License Numbers in Adult-Use StatesMPPNo ratings yet
- Revenue From Adult Use StatesDocument5 pagesRevenue From Adult Use StatesMPPNo ratings yet
- Of Antimicrobial Resistance: The Who Aware (Access, Watch, Reserve) Antibiotic Book and PreventionDocument7 pagesOf Antimicrobial Resistance: The Who Aware (Access, Watch, Reserve) Antibiotic Book and PreventionBBD BBDNo ratings yet
- Sun Zi's Strategies Help Pfizer SucceedDocument15 pagesSun Zi's Strategies Help Pfizer SucceedKomalaa BalanNo ratings yet
- PHA3801 Short Answer QuestionsDocument5 pagesPHA3801 Short Answer QuestionsFarhana Azmira AsmadiNo ratings yet
- 19 FebDocument2 pages19 FebNlm NaulakNo ratings yet
- A Review On Effervescent TabletDocument6 pagesA Review On Effervescent TabletInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Drug Study - AzithromycinDocument3 pagesDrug Study - AzithromycinLorel Faith ToradaNo ratings yet
- Evaluation of Poisoning and Drug Overdose Among Cases Presented To Poison Control Centre, Ain Shams University Hospital During The Year 2015Document13 pagesEvaluation of Poisoning and Drug Overdose Among Cases Presented To Poison Control Centre, Ain Shams University Hospital During The Year 2015Hany TawfikNo ratings yet
- Dr. Warsinggih, SP.B-KBD (SLIDE ERAS in Digestive Surgery)Document34 pagesDr. Warsinggih, SP.B-KBD (SLIDE ERAS in Digestive Surgery)dewiswahyuNo ratings yet
- Lista Barna 2013Document43 pagesLista Barna 2013Denisa KalaciNo ratings yet
- KMPLN Cara Menghitung RumusDocument46 pagesKMPLN Cara Menghitung RumusLia SetiawatiNo ratings yet
- Salmeterol+ FluticasonaDocument1 pageSalmeterol+ FluticasonaJulian Santiago Ladino AlemanNo ratings yet
- Emergency Drug Box Approved ListDocument1 pageEmergency Drug Box Approved ListGee_anne_Saldi_9627No ratings yet
- Pharmacokinetics and pharmacodynamics of anaesthetic drugs in paediatricsDocument7 pagesPharmacokinetics and pharmacodynamics of anaesthetic drugs in paediatricsR KNo ratings yet
- Pediatric Practice Math ProblemsDocument3 pagesPediatric Practice Math ProblemsKaren HutchinsonNo ratings yet
- Types of Drug Preparation (Credit To The Rightful Owner)Document1 pageTypes of Drug Preparation (Credit To The Rightful Owner)Keren Grace EspirituNo ratings yet
- Pharmacokinetics PrinciplesDocument11 pagesPharmacokinetics PrinciplesEryll Paolo AleaNo ratings yet
- PD3 - Dose-Response Relationship - Akm-050116 PDFDocument27 pagesPD3 - Dose-Response Relationship - Akm-050116 PDFSindhu Babu100% (1)
- WHO Pharm 2-2023Document19 pagesWHO Pharm 2-2023Paola Cristini Gama SilvaNo ratings yet
- SynthroidDocument3 pagesSynthroidKatie McPeekNo ratings yet
- Medicinal Chemistry (MCQs Exam)Document10 pagesMedicinal Chemistry (MCQs Exam)AbCc100% (6)
- 3819 - Ibr - November - 2020 - Written - Expression - Exam FRENKI QIRJAKODocument6 pages3819 - Ibr - November - 2020 - Written - Expression - Exam FRENKI QIRJAKOkevin hoxhaNo ratings yet
- IV Med AdminDocument4 pagesIV Med AdminMa. Ferimi Gleam BajadoNo ratings yet
- Dosage CalculationsDocument8 pagesDosage CalculationsReinna Angel CampoNo ratings yet
- Pain Managment in Nursing (Fundamentals)Document21 pagesPain Managment in Nursing (Fundamentals)crosadotNo ratings yet
- Rle Lectures Medications: Arturo G. Garcia JR RN, MSN, U.S RNDocument33 pagesRle Lectures Medications: Arturo G. Garcia JR RN, MSN, U.S RNMaria Paula Amor GeronimoNo ratings yet
- Clinical Pharmacy and TherapeuticsDocument1 pageClinical Pharmacy and TherapeuticsAnkita UpadhyayNo ratings yet
- Drugs Affecting The Respiratory SystemDocument32 pagesDrugs Affecting The Respiratory SystemKita kitaNo ratings yet
- Preparation and Evaluation of Microsphere of Antidiabetic Drug by Emulsion Solvent Evaporation MethodDocument21 pagesPreparation and Evaluation of Microsphere of Antidiabetic Drug by Emulsion Solvent Evaporation MethodSujit DasNo ratings yet
- Pharma Topic 3 NotesDocument3 pagesPharma Topic 3 NotesAshley Franceska CansanayNo ratings yet
- Mapeh 6: Quarter 4 - Module 1Document10 pagesMapeh 6: Quarter 4 - Module 1ALEX CORPORALNo ratings yet