You might also like
- Physician Assistant PANCE & PANRE: a QuickStudy Laminated Reference GuideFrom EverandPhysician Assistant PANCE & PANRE: a QuickStudy Laminated Reference GuideNo ratings yet
- Adult Soap Note GuideDocument5 pagesAdult Soap Note Guidelizdp21No ratings yet
- A Practical Guide To Clinical MedicineDocument11 pagesA Practical Guide To Clinical MedicineMichael NyaongoNo ratings yet
- History3 LungooooooDocument10 pagesHistory3 LungooooooGiorgio CivitareseNo ratings yet
- First Aid ObGynDocument252 pagesFirst Aid ObGynineedsomebooksNo ratings yet
- NEUROPrelims - History Taking in NeurologyDocument4 pagesNEUROPrelims - History Taking in NeurologyRenatoCosmeGalvanJuniorNo ratings yet
- First Aid For The Obstetrics Gynecology ClerkshipDocument252 pagesFirst Aid For The Obstetrics Gynecology ClerkshipsilasjubaNo ratings yet
- Clinical History TakingDocument36 pagesClinical History Takingapi-1964133775% (4)
- 10 The Rest of The HistoryDocument3 pages10 The Rest of The Historybeba macasinagNo ratings yet
- MRCGP OsceDocument4 pagesMRCGP OsceJaved YakoobNo ratings yet
- First Aid For The Obstetrics & Gynecology ClerkshipDocument253 pagesFirst Aid For The Obstetrics & Gynecology Clerkshipadereje7100% (1)
- HP Worksheet RevisedDocument15 pagesHP Worksheet Revisedapi-273787321No ratings yet
- Medical History Guidelines & Components 2021Document5 pagesMedical History Guidelines & Components 2021TLNo ratings yet
- 2beginning The History Taking-1Document30 pages2beginning The History Taking-1Wizz Háķìm ĻêşòwNo ratings yet
- CPC 3Document47 pagesCPC 3Kenneth NuñezNo ratings yet
- Adult NAC RevisedDocument26 pagesAdult NAC RevisedOsan BogdanNo ratings yet
- Proforma Ophthalmic HistoryDocument3 pagesProforma Ophthalmic Historymahir patelNo ratings yet
- Pharmacy CounsellingDocument8 pagesPharmacy CounsellingChrissieNo ratings yet
- Client Health HistoryDocument22 pagesClient Health HistoryAudrygodwynNo ratings yet
- TDM Exam Study Resources PDFDocument5 pagesTDM Exam Study Resources PDFDrosler MedqsNo ratings yet
- MRCGP OsceDocument17 pagesMRCGP OsceJaved Yakoob100% (1)
- Screening For Good Health: The Australian Guide To Health Screening And ImmunisationFrom EverandScreening For Good Health: The Australian Guide To Health Screening And ImmunisationNo ratings yet
- History TakingDocument51 pagesHistory TakingJAMES TONNY OKINYINo ratings yet
- History TakingDocument51 pagesHistory TakingJAMES TONNY OKINYINo ratings yet
- Pat FundamentalsDocument14 pagesPat Fundamentalsapi-281676750No ratings yet
- SOAP Note AdviceDocument5 pagesSOAP Note AdviceNico AvellanaNo ratings yet
- Clinical Exam. & History TakingDocument23 pagesClinical Exam. & History TakingManiish Trivedi100% (2)
- MH Case StudyDocument17 pagesMH Case StudyS. JacobsNo ratings yet
- 5-1 HX & Exam Handbook Final PDFDocument23 pages5-1 HX & Exam Handbook Final PDFPépé TechopathamNo ratings yet
- Nursing Health History FormatDocument7 pagesNursing Health History FormatJasmine PonceNo ratings yet
- Nursing Health History FormatDocument7 pagesNursing Health History Formatgeraldine suarezNo ratings yet
- History of Present IllnessDocument10 pagesHistory of Present Illnesshirsi200518No ratings yet
- Gordon's 11 Functional Health PatternDocument3 pagesGordon's 11 Functional Health Patternbladimer_ria100% (3)
- Nursing History - A. Syanthiqah TirtaDocument3 pagesNursing History - A. Syanthiqah TirtaSanti TirtaNo ratings yet
- University of South Florida College of Nursing: Fundamental Patient Assessment ToolDocument13 pagesUniversity of South Florida College of Nursing: Fundamental Patient Assessment Toolapi-315444338No ratings yet
- Winnyfred Patience Ayugi Bsc. MidwiferyDocument30 pagesWinnyfred Patience Ayugi Bsc. MidwiferyAYO NELSONNo ratings yet
- PHB Lec 1 Phlebotomy and The Health Care Setting Part 1Document42 pagesPHB Lec 1 Phlebotomy and The Health Care Setting Part 1Jean KenNo ratings yet
- Tally and O'Connor's Clinical Examination (8 Edition, Volume 1) Notes & Summaries by Yasin KadriDocument9 pagesTally and O'Connor's Clinical Examination (8 Edition, Volume 1) Notes & Summaries by Yasin KadriYasin KadriNo ratings yet
- Pat Revised 2013 1Document19 pagesPat Revised 2013 1api-300362033No ratings yet
- Speaking Sub-Test Overview PDFDocument10 pagesSpeaking Sub-Test Overview PDFProsanjit MajumderNo ratings yet
- Foundations of Clinical Medicine-1 Summer 2014 Semester: History TakingDocument63 pagesFoundations of Clinical Medicine-1 Summer 2014 Semester: History Takingparanoea911100% (1)
- How To Fi ND Doctor Right: Elping PeopleDocument8 pagesHow To Fi ND Doctor Right: Elping PeopleAB ShawNo ratings yet
- Functional HealthassessmentDocument74 pagesFunctional HealthassessmentZanie CruzNo ratings yet
- AHG Health & Medical FormsDocument12 pagesAHG Health & Medical FormsAnonymous 2buCBbFNo ratings yet
- The Ultimate Guide to Physician Associate OSCEs: Written by a Physician Associate for Physician AssociatesFrom EverandThe Ultimate Guide to Physician Associate OSCEs: Written by a Physician Associate for Physician AssociatesNo ratings yet
- Health HistoryDocument19 pagesHealth HistoryAngelene Caliva100% (1)
- TDM Candidate Information Sheet July2020Document6 pagesTDM Candidate Information Sheet July2020Miguel Alberto Perez SanchezNo ratings yet
- 2019-02-22T161010.053Document17 pages2019-02-22T161010.053felamendoNo ratings yet
- HP Worksheet RevisedDocument14 pagesHP Worksheet Revisedapi-261460315100% (1)
- Clinical ClerkingDocument17 pagesClinical ClerkingMuhammad ShakeelNo ratings yet
- Barriers To Communication: Communication Barrier - Anything That Gets in The Way of Clear CommunicationDocument29 pagesBarriers To Communication: Communication Barrier - Anything That Gets in The Way of Clear CommunicationRana Waji Ul HassanNo ratings yet
- First Aid For The Obstetrics & Gynecology ClerkshipDocument253 pagesFirst Aid For The Obstetrics & Gynecology ClerkshipSimona Prodanoiu100% (17)
- Soap RoutineDocument3 pagesSoap RoutineRoberto Ramos100% (1)
- Primary Care Intake PaperworkDocument7 pagesPrimary Care Intake Paperworkasalizwa ludlalaNo ratings yet
- HOPI in History TakingDocument5 pagesHOPI in History TakingKumar KP100% (1)
- Clinical Skills Review: Scenarios Based on Standardized PatientsFrom EverandClinical Skills Review: Scenarios Based on Standardized PatientsRating: 4 out of 5 stars4/5 (10)
- Oop Say You Know MeDocument1 pageOop Say You Know MeawuahbohNo ratings yet
- Article For JournalDocument6 pagesArticle For JournalawuahbohNo ratings yet
- NCLEX Random FactsDocument34 pagesNCLEX Random FactsLegnaMary100% (8)
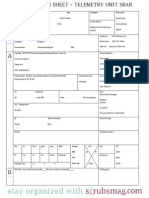
- Nurse Brain Sheet Telemetry Unit SBARDocument1 pageNurse Brain Sheet Telemetry Unit SBARvsosa624No ratings yet
- The BSN Job Search: Interview Preparation: Telling Your StoryDocument25 pagesThe BSN Job Search: Interview Preparation: Telling Your StoryawuahbohNo ratings yet
- King Rush MoreDocument1 pageKing Rush MoreawuahbohNo ratings yet
- HandOff SampleToolsDocument9 pagesHandOff SampleToolsOllie EvansNo ratings yet
- Pharm NclexDocument9 pagesPharm NclexawuahbohNo ratings yet
- PolypharmacyDocument24 pagesPolypharmacySurina Zaman HuriNo ratings yet
- EBP Article 1Document11 pagesEBP Article 1awuahbohNo ratings yet
- Probability of A or B and A and B-1Document2 pagesProbability of A or B and A and B-1awuahbohNo ratings yet
- Massachusetts Department of Public HealthDocument24 pagesMassachusetts Department of Public HealthawuahbohNo ratings yet
- Article For CET CHFDocument5 pagesArticle For CET CHFawuahbohNo ratings yet
- EBP Article 3Document6 pagesEBP Article 3awuahbohNo ratings yet
- STDA VaricealDocument8 pagesSTDA VaricealDeisy de JesusNo ratings yet
- Random FactsDocument338 pagesRandom Factscyram81100% (1)
- Tips On Answering NclexDocument4 pagesTips On Answering NclexawuahbohNo ratings yet
- Critical Thinking StrategiesDocument3 pagesCritical Thinking StrategiesawuahbohNo ratings yet
- Article For CET CHFDocument5 pagesArticle For CET CHFawuahbohNo ratings yet
- Drugs NclexDocument30 pagesDrugs Nclexawuahboh100% (1)
- Therapeutic CommunicationDocument1 pageTherapeutic CommunicationawuahbohNo ratings yet
- Patient Report FormDocument1 pagePatient Report FormawuahbohNo ratings yet
- ENT Throat and EsophagusDocument41 pagesENT Throat and EsophagusMUHAMMAD HASAN NAGRANo ratings yet
- Does Prospective Payment Increase Hospital (In) Efficiency? Evidence From The Swiss Hospital SectorDocument24 pagesDoes Prospective Payment Increase Hospital (In) Efficiency? Evidence From The Swiss Hospital SectorawuahbohNo ratings yet
- Article For Journal 4-18-14Document8 pagesArticle For Journal 4-18-14awuahbohNo ratings yet
- Article For JournalDocument6 pagesArticle For JournalawuahbohNo ratings yet
- Med Surg BurnsDocument8 pagesMed Surg BurnsawuahbohNo ratings yet
- Debate 3 Youth Incarceration in Adult PrisonsDocument6 pagesDebate 3 Youth Incarceration in Adult PrisonsawuahbohNo ratings yet
- Article For Jouranal 2 (498P)Document5 pagesArticle For Jouranal 2 (498P)awuahbohNo ratings yet
- Prognostic Factors and Management of Patients With Choanal AtresiaDocument7 pagesPrognostic Factors and Management of Patients With Choanal Atresiafarah maulida martaNo ratings yet
- CCDocument5 pagesCCnazmulNo ratings yet
- Operator'S Manual Diesel Engine: 2L41C - 2M41 - 2M41ZDocument110 pagesOperator'S Manual Diesel Engine: 2L41C - 2M41 - 2M41ZMauricio OlayaNo ratings yet
- The Reason: B. FlowsDocument4 pagesThe Reason: B. FlowsAryanti UrsullahNo ratings yet
- Reaction Paper FinalDocument5 pagesReaction Paper FinalJelo RoxasNo ratings yet
- Newsletter 1-2021 Nordic-Baltic RegionDocument30 pagesNewsletter 1-2021 Nordic-Baltic Regionapi-206643591100% (1)
- Functional Programming in Swift by Eidhof Chris, Kugler Florian, Swierstra Wouter.Document212 pagesFunctional Programming in Swift by Eidhof Chris, Kugler Florian, Swierstra Wouter.angloesamNo ratings yet
- The Time Machine Was First Published in 1984 As A Story Under The Name The Time Traveller in The National ObserverDocument1 pageThe Time Machine Was First Published in 1984 As A Story Under The Name The Time Traveller in The National ObservermarceNo ratings yet
- Extract The .Msi FilesDocument2 pagesExtract The .Msi FilesvladimirNo ratings yet
- CRISTIAN COLCERIU - PERSONALITATI CLUJENE Prof - Dr.ing - POMPILIU MANEADocument21 pagesCRISTIAN COLCERIU - PERSONALITATI CLUJENE Prof - Dr.ing - POMPILIU MANEAcristian colceriu100% (2)
- Lab Manual Switchgear and Protection SapDocument46 pagesLab Manual Switchgear and Protection SapYash MaheshwariNo ratings yet
- 9881 enDocument345 pages9881 enSaid BenNo ratings yet
- Refutation EssayDocument6 pagesRefutation Essayapi-314826327No ratings yet
- Daily Lesson Log Quarter 1 Week 1Document5 pagesDaily Lesson Log Quarter 1 Week 1John Patrick Famadulan100% (1)
- Manual de Operacion y MantenimientoDocument236 pagesManual de Operacion y MantenimientoalexNo ratings yet
- Principles of Supply Chain Management A Balanced Approach 4th Edition Wisner Solutions ManualDocument36 pagesPrinciples of Supply Chain Management A Balanced Approach 4th Edition Wisner Solutions Manualoutlying.pedantry.85yc100% (28)
- Duo Interpretation Class PresentationDocument31 pagesDuo Interpretation Class PresentationPlanetSparkNo ratings yet
- Erosional VelocityDocument15 pagesErosional VelocityGary JonesNo ratings yet
- Consent Form: Republic of The Philippines Province of - Municipality ofDocument1 pageConsent Form: Republic of The Philippines Province of - Municipality ofLucette Legaspi EstrellaNo ratings yet
- Fire Prevention Plan Template - FINAL 5-30-08Document5 pagesFire Prevention Plan Template - FINAL 5-30-08Peter GeorgeNo ratings yet
- Vieworks DR Panel BrochureDocument8 pagesVieworks DR Panel Brochuretito goodNo ratings yet
- Natural Cataclysms and Global ProblemsDocument622 pagesNatural Cataclysms and Global ProblemsphphdNo ratings yet
- Past Simple Vs Past ContinuousDocument3 pagesPast Simple Vs Past ContinuousNatalia SalinasNo ratings yet
- Low Speed Aerators PDFDocument13 pagesLow Speed Aerators PDFDgk RajuNo ratings yet
- Transparency and Digitalization in The Public Administration of RomaniaDocument8 pagesTransparency and Digitalization in The Public Administration of RomaniaMădălina MarincaşNo ratings yet
- Microfinance Ass 1Document15 pagesMicrofinance Ass 1Willard MusengeyiNo ratings yet
- Ancient Sumer Flip BookDocument9 pagesAncient Sumer Flip Bookapi-198624210No ratings yet
- Roles and Responsibilities of An InstructorDocument4 pagesRoles and Responsibilities of An InstructorMohanlal SainiNo ratings yet
- 21 Tara Mantra-Wps OfficeDocument25 pages21 Tara Mantra-Wps OfficeAlteo FallaNo ratings yet
- Flow of FoodDocument2 pagesFlow of FoodGenevaNo ratings yet