You might also like
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- V. Pathophysiology Modifiable: Non - ModifiableDocument2 pagesV. Pathophysiology Modifiable: Non - ModifiableMary Grace BanezNo ratings yet
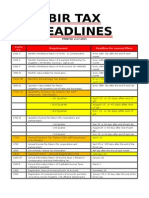
- Bir Tax Deadlines 2015Document2 pagesBir Tax Deadlines 2015Mary Grace BanezNo ratings yet
- 2014 Tax Calendar (For Web)Document29 pages2014 Tax Calendar (For Web)Mary Grace BanezNo ratings yet
- Mech VentDocument8 pagesMech VentMary Grace BanezNo ratings yet
- Nonimmigrant Visa Application ProceduresDocument12 pagesNonimmigrant Visa Application ProceduresMary Grace BanezNo ratings yet
- The Nine Abdominal RegionsDocument2 pagesThe Nine Abdominal RegionsMary Grace BanezNo ratings yet
- VS SheetDocument1 pageVS SheetMary Grace BanezNo ratings yet
- SOCIO 102 Course SyllabusDocument2 pagesSOCIO 102 Course SyllabusMary Grace BanezNo ratings yet
- Christopher KaplonskiDocument3 pagesChristopher KaplonskiMary Grace BanezNo ratings yet
- Mutagenic Agents TableDocument1 pageMutagenic Agents TableMary Grace BanezNo ratings yet
- FDARDocument1 pageFDARMary Grace BanezNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (894)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Shipping dispute over vessel possession resolved in courtDocument4 pagesShipping dispute over vessel possession resolved in courtMarian's PreloveNo ratings yet
- Judgement in OS 9 OF 2021Document8 pagesJudgement in OS 9 OF 2021r4ravitejNo ratings yet
- Domingo Neypes Vs Court of AppealsDocument1 pageDomingo Neypes Vs Court of AppealsAurora Pelagio VallejosNo ratings yet
- Nagaland Jhumland Act 1970Document15 pagesNagaland Jhumland Act 1970Latest Laws TeamNo ratings yet
- Fedman Development Corporation, Vs AgcaoiliDocument1 pageFedman Development Corporation, Vs AgcaoiliJay-ar TeodoroNo ratings yet
- Heirs of Francisco I Narvasa SR Et Al Vs Emiliana Imbornal Et AlDocument10 pagesHeirs of Francisco I Narvasa SR Et Al Vs Emiliana Imbornal Et AlJuan TañamorNo ratings yet
- United States v. Colonial Motor Inn, Inc., and Maurice Shear, 440 F.2d 1227, 1st Cir. (1971)Document3 pagesUnited States v. Colonial Motor Inn, Inc., and Maurice Shear, 440 F.2d 1227, 1st Cir. (1971)Scribd Government DocsNo ratings yet
- Benguet Corporation Tailings Dam Tax Assessment CaseDocument8 pagesBenguet Corporation Tailings Dam Tax Assessment CaseEmma Ruby Aguilar-ApradoNo ratings yet
- NIH Patent Services AwardsDocument4 pagesNIH Patent Services AwardsDaniel BallardNo ratings yet
- Andhra Pradesh Civil Courts Amendment Act 1989Document12 pagesAndhra Pradesh Civil Courts Amendment Act 1989Latest Laws TeamNo ratings yet
- Kes MahkamahDocument16 pagesKes Mahkamahfirdaus azinunNo ratings yet
- Already Elected Philippine Citizenship For Protestee by Declaring Him As Such."Document5 pagesAlready Elected Philippine Citizenship For Protestee by Declaring Him As Such."Raymond ChengNo ratings yet
- Datatreasury Corporation v. Wells Fargo & Company Et Al - Document No. 581Document6 pagesDatatreasury Corporation v. Wells Fargo & Company Et Al - Document No. 581Justia.comNo ratings yet
- Mumbai Tribunal Rules Reimbursement of ExpensesDocument5 pagesMumbai Tribunal Rules Reimbursement of ExpensestongkiNo ratings yet
- Property Class IntroductionDocument108 pagesProperty Class Introductionachrys13No ratings yet
- Tutorial 2Document3 pagesTutorial 2猪mongNo ratings yet
- Devesh Tripathi Mnlu CVDocument3 pagesDevesh Tripathi Mnlu CVArpit GoyalNo ratings yet
- People v. Dumlao DigestDocument1 pagePeople v. Dumlao DigestbillietotNo ratings yet
- RAM JETHMALANI Vs PDFDocument2 pagesRAM JETHMALANI Vs PDFRvi MahayNo ratings yet
- Special Power of Attorney DfaDocument4 pagesSpecial Power of Attorney DfaAlijoh Aries M. Aquidado0% (1)
- G-P-, AXXX XXX 001 (BIA Sept. 25, 2017)Document9 pagesG-P-, AXXX XXX 001 (BIA Sept. 25, 2017)Immigrant & Refugee Appellate Center, LLCNo ratings yet
- Luzon Stevedoring Corporation Vs CADocument1 pageLuzon Stevedoring Corporation Vs CAPan CorreoNo ratings yet
- Doctrine of Isolated TransactionDocument2 pagesDoctrine of Isolated Transactionangelo_uy2No ratings yet
- Procedure For Project Charter - 25 Aug 2011Document15 pagesProcedure For Project Charter - 25 Aug 2011Atif Mumtaz KhanNo ratings yet
- DynCorps' Answer To Original ComplaintDocument12 pagesDynCorps' Answer To Original ComplaintDallasObserverNo ratings yet
- COMAT Training Services Job ApplicationDocument5 pagesCOMAT Training Services Job ApplicationRiti Noor AknanNo ratings yet
- Dick Bentley Productions Ltd. and Another V Harold Smith (Motors) Ltd.Document7 pagesDick Bentley Productions Ltd. and Another V Harold Smith (Motors) Ltd.Squall LeonhartNo ratings yet
- Sahib Foods LTD & Anor V Paskin Kyriakides Sands (2003) EWCA Civ 1832Document3 pagesSahib Foods LTD & Anor V Paskin Kyriakides Sands (2003) EWCA Civ 1832lylei2010No ratings yet
- INTELLECTUAL PROPERTY 2017 TSN Part 1 Introduction To TrademarkDocument51 pagesINTELLECTUAL PROPERTY 2017 TSN Part 1 Introduction To TrademarkKarlena G. LuzNo ratings yet
- Boston Globe 2707Document36 pagesBoston Globe 2707Grafo Bogdanov Novi SadNo ratings yet