You might also like
- 115 Sample Chapter PDFDocument111 pages115 Sample Chapter PDFAmey GudigarNo ratings yet
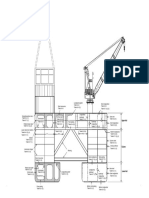
- Semi-Submersible (Nomenclature)Document1 pageSemi-Submersible (Nomenclature)Free_Beating_HeartNo ratings yet
- Vessel Stability GuidelinesDocument32 pagesVessel Stability Guidelinesahong100No ratings yet
- Traffic Circle vs Roundabout: Key DifferencesDocument1 pageTraffic Circle vs Roundabout: Key DifferencesFree_Beating_HeartNo ratings yet
- Ship Stability NotesDocument13 pagesShip Stability NotesDnv Bailey100% (1)
- Treatment ProcessesDocument36 pagesTreatment ProcessesFree_Beating_HeartNo ratings yet
- 115 Sample Chapter PDFDocument111 pages115 Sample Chapter PDFAmey GudigarNo ratings yet
- Fact File 2008 PDFDocument99 pagesFact File 2008 PDFsantiagovbNo ratings yet
- Masonry - RoymechDocument6 pagesMasonry - RoymechFree_Beating_HeartNo ratings yet
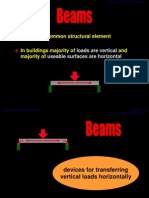
- Extremely Common Structural Element: Loads Are Vertical Useable Surfaces Are HorizontalDocument39 pagesExtremely Common Structural Element: Loads Are Vertical Useable Surfaces Are Horizontaldox4useNo ratings yet
- Balanced Section Explanation - Bill Mosley 6th Ed.Document3 pagesBalanced Section Explanation - Bill Mosley 6th Ed.Free_Beating_HeartNo ratings yet
- How To Lay A New Water Supply PipeDocument4 pagesHow To Lay A New Water Supply PipeNasir KamalNo ratings yet
- Unite 600x600x150 PUB 71-1406ADocument1 pageUnite 600x600x150 PUB 71-1406AFree_Beating_HeartNo ratings yet
- Technical Data Sheet For HIT-HY-200 Injectable Mortar For Anchor and Rebar Technical Information ASSET DOC 2331175Document85 pagesTechnical Data Sheet For HIT-HY-200 Injectable Mortar For Anchor and Rebar Technical Information ASSET DOC 2331175ing urbanNo ratings yet
- Hdb-E - Manufacturers LituratureDocument28 pagesHdb-E - Manufacturers LituratureFree_Beating_HeartNo ratings yet
- Beam DeflectionDocument5 pagesBeam DeflectionChinna ValleNo ratings yet
- Arcadis Corporate Brochure 2015Document50 pagesArcadis Corporate Brochure 2015Free_Beating_HeartNo ratings yet
- Installing Shower PumpDocument4 pagesInstalling Shower PumpFree_Beating_HeartNo ratings yet
- Scale User ManualDocument15 pagesScale User ManualFree_Beating_HeartNo ratings yet
- Bulb FlatDocument12 pagesBulb FlatMahdiNo ratings yet
- Scale User ManualDocument15 pagesScale User ManualFree_Beating_HeartNo ratings yet
- LR Civil Engineering Guidelines For SurveyorsDocument63 pagesLR Civil Engineering Guidelines For SurveyorsFree_Beating_HeartNo ratings yet
- Introduction To OceanographyDocument6 pagesIntroduction To OceanographyFree_Beating_HeartNo ratings yet
- Concrete Centre Basements For HousingDocument24 pagesConcrete Centre Basements For HousingFree_Beating_Heart100% (1)
- SteelDocument38 pagesSteelvidrascuNo ratings yet
- Northsea Oil Gas Map 2013Document1 pageNorthsea Oil Gas Map 2013Free_Beating_HeartNo ratings yet
- Hadith Jibreel (Angel Gabriel)Document2 pagesHadith Jibreel (Angel Gabriel)Free_Beating_Heart100% (1)
- The Spiritual Cure - Surah Al FatihaDocument203 pagesThe Spiritual Cure - Surah Al Fatihaلا اله الا الله محمد رسول الله 1No ratings yet
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (894)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Open Hole Logging Services: Logging Tool Mnemonic Logging Tool Name Log Type Formation Property Measured CommentDocument5 pagesOpen Hole Logging Services: Logging Tool Mnemonic Logging Tool Name Log Type Formation Property Measured CommentRio de MarioNo ratings yet
- Guidelines For Produced Water InjectionDocument28 pagesGuidelines For Produced Water InjectionleopumpkingNo ratings yet
- Backreaming SPE 116555 MSDocument17 pagesBackreaming SPE 116555 MSCharles Desmazures100% (1)
- Introductory To Well HeadDocument20 pagesIntroductory To Well HeadAhmad Reza Atef100% (1)
- Waterflooding overviewDocument68 pagesWaterflooding overviewAdisti A100% (1)
- Drilling Torque & DragDocument66 pagesDrilling Torque & DragShamit Rathi100% (1)
- Bourgoyne AdamDocument130 pagesBourgoyne AdamOSDocs2012No ratings yet
- SPE102378 Jetting Structural Casing in DeepwaterDocument15 pagesSPE102378 Jetting Structural Casing in DeepwaterKarime VegaNo ratings yet
- Ch08 Multizone CompletionDocument33 pagesCh08 Multizone CompletionPrithiraj KalitaNo ratings yet
- Non-Consolidating Plugging Material For Wellbore and AnnulusDocument18 pagesNon-Consolidating Plugging Material For Wellbore and AnnulusSLACKENGINEERNo ratings yet
- New Retrievable Wire Line Cementing ToolDocument8 pagesNew Retrievable Wire Line Cementing ToolPutri MarantikaNo ratings yet
- Elevator Design GuidelinesDocument39 pagesElevator Design GuidelinesErnesto Andres Guevara MalaveNo ratings yet
- Drilling Operation OverviewDocument21 pagesDrilling Operation OverviewWai HtutNo ratings yet
- TCFR Product Sheet A4 2016Document2 pagesTCFR Product Sheet A4 2016unduhNo ratings yet
- UGSSolutionsDocument6 pagesUGSSolutionscuervohijoguachoNo ratings yet
- 08-HLB Packers PDFDocument66 pages08-HLB Packers PDFQaiser HafeezNo ratings yet
- 2 Completions & FluidsDocument52 pages2 Completions & Fluidsعبد العزيز مروىNo ratings yet
- H09626 IsolizerCentralizerDocument2 pagesH09626 IsolizerCentralizerAQUILES CARRERANo ratings yet
- Squeeze Cementing JobDocument64 pagesSqueeze Cementing Jobkhushbu Hasan100% (1)
- PRESSURE TEST AFTER WOC (Wait On Cement) OIL WELL CASING DESIGNDocument10 pagesPRESSURE TEST AFTER WOC (Wait On Cement) OIL WELL CASING DESIGNCharlie TinelliNo ratings yet
- Management Skill: RIG Manager Training DiagramDocument1 pageManagement Skill: RIG Manager Training DiagramLong Do100% (1)
- 06 Openhole IsolationDocument24 pages06 Openhole IsolationMuhammad ShahrukhNo ratings yet
- Steel Pipe & Tube Products CatalogDocument14 pagesSteel Pipe & Tube Products CatalogJawad ChamsouNo ratings yet
- 7 Liner Running & CementingDocument84 pages7 Liner Running & Cementingafasdg100% (1)
- Piezometer Instruction ManualDocument32 pagesPiezometer Instruction ManualHernánNo ratings yet
- ASTM D2573 - 08, Field Vane Shear Test in Cohesive Soil PDFDocument8 pagesASTM D2573 - 08, Field Vane Shear Test in Cohesive Soil PDFLuis ValdiviaNo ratings yet
- Subsea Well Plug and Abandon Intervention Using A Coiled Tubing Conveyed Inflatable Packer A Case Study KopyaDocument7 pagesSubsea Well Plug and Abandon Intervention Using A Coiled Tubing Conveyed Inflatable Packer A Case Study KopyaErdal AYDINNo ratings yet
- Packer Calculations SecureDocument230 pagesPacker Calculations SecureEmre Cengiz100% (3)
- Cementing Example ProblemDocument10 pagesCementing Example ProblemChilledambienceNo ratings yet
- Plunger LiftDocument4 pagesPlunger LiftChristian AvilaNo ratings yet