You might also like
- Congestive Heart Failure ReportDocument6 pagesCongestive Heart Failure ReportSunshine_Bacla_4275100% (1)
- HYPERTENSIONDocument5 pagesHYPERTENSIONRajesh RamanNo ratings yet
- 10-11 Treatment of HypertensionDocument11 pages10-11 Treatment of HypertensionHanif GandohNo ratings yet
- Congestive Heart Failure: CardiacDocument36 pagesCongestive Heart Failure: CardiacHUZAIFA YAMAANNo ratings yet
- Antihypertensive Pharmacologic Agents: Nr33 K Burger, Msed, MSN, RN, CneDocument28 pagesAntihypertensive Pharmacologic Agents: Nr33 K Burger, Msed, MSN, RN, CneLopez JoeNo ratings yet
- Pedal EdemaDocument45 pagesPedal Edemafirdaushassan2112No ratings yet
- Anti Arrhythmic DrugsDocument91 pagesAnti Arrhythmic DrugsAlex beharuNo ratings yet
- Pharmacology Cardiovascular DrugsDocument120 pagesPharmacology Cardiovascular DrugsDareRaymond100% (1)
- Cardiotronic MedicationsDocument13 pagesCardiotronic MedicationsTee WoodNo ratings yet
- Treating Heart Failure: Current Guidelines for Pharmacological ManagementDocument11 pagesTreating Heart Failure: Current Guidelines for Pharmacological ManagementKareem SaeedNo ratings yet
- Pharmacotherapy of Congestive Heart Failure (CHF)Document163 pagesPharmacotherapy of Congestive Heart Failure (CHF)Aditya rathoreNo ratings yet
- Cad CommerDocument2 pagesCad CommerWhatDoYouSeriesNo ratings yet
- Cardiovascular Agent: Prof. Clement Belvis RN, RM, MPHDocument86 pagesCardiovascular Agent: Prof. Clement Belvis RN, RM, MPHEimhie Lee CasiNo ratings yet
- Drug Presentation On Anti-Hypertensive: All India Institute of Medical and Science New Delhi 2021-2022Document12 pagesDrug Presentation On Anti-Hypertensive: All India Institute of Medical and Science New Delhi 2021-2022Priya SinghNo ratings yet
- Drugs For Congestive Heart FailureDocument46 pagesDrugs For Congestive Heart Failuresultan khabeeb100% (1)
- Cardio Lab MedsDocument11 pagesCardio Lab MedsDianne Erika MeguinesNo ratings yet
- Management of Heart Failure: OutlineDocument27 pagesManagement of Heart Failure: OutlineBoetik AlifiaNo ratings yet
- CHF Drugs Guide: Key Medications for Treating Congestive Heart FailureDocument21 pagesCHF Drugs Guide: Key Medications for Treating Congestive Heart Failuremohsen mirdamadiNo ratings yet
- Antihypertensive & Antianginal DrugsDocument5 pagesAntihypertensive & Antianginal Drugsdomememe1No ratings yet
- Drugs for Hypertension 2023 (1)Document19 pagesDrugs for Hypertension 2023 (1)aguilarjanicaNo ratings yet
- Pharmacology Chapter 42 zp-1-3Document42 pagesPharmacology Chapter 42 zp-1-3sho bartNo ratings yet
- 1 Antihypertensive DrugsDocument14 pages1 Antihypertensive DrugsReda SoNo ratings yet
- Cardiac Drugs PowerpointDocument17 pagesCardiac Drugs PowerpointsiratelNo ratings yet
- Congestive Cardiac Failure (1)Document27 pagesCongestive Cardiac Failure (1)Krupasagar Pn PalegarNo ratings yet
- ACE Inhibitors: Medications To Control Blood PressureDocument3 pagesACE Inhibitors: Medications To Control Blood PressurekNo ratings yet
- Pharmacology: Unit VIIIDocument92 pagesPharmacology: Unit VIIIChristian Laraya AlayonNo ratings yet
- Hypertension: 1-Hypertension Is Defined As (BP)Document37 pagesHypertension: 1-Hypertension Is Defined As (BP)hussein alnasryNo ratings yet
- Drug StudyDocument28 pagesDrug StudyJheryck SabadaoNo ratings yet
- CARDIAC-MEDICATION-LECTUREDocument23 pagesCARDIAC-MEDICATION-LECTUREilikeedsheeranNo ratings yet
- Cardiac Drugs PowerpointDocument17 pagesCardiac Drugs PowerpointNoci M. FrenkNo ratings yet
- Merged 1 PDFDocument305 pagesMerged 1 PDFAhmed KurdiNo ratings yet
- Update: Review and Update On Inotropes and VasopressorsDocument9 pagesUpdate: Review and Update On Inotropes and VasopressorsMaryam JamilahNo ratings yet
- Antihypertensive DrugsDocument52 pagesAntihypertensive Drugsapi-224264169No ratings yet
- Drugs Used in HF IIDocument40 pagesDrugs Used in HF IIJamal LudinNo ratings yet
- CHF Simulation PreparationDocument5 pagesCHF Simulation Preparation5Dragoon5No ratings yet
- Heart Failure New SlidesDocument41 pagesHeart Failure New SlidesjawadNo ratings yet
- 11A Drugs Acting On The Cardiovascular SystemDocument85 pages11A Drugs Acting On The Cardiovascular SystemJaps De la CruzNo ratings yet
- 5 HypertensionDocument8 pages5 Hypertensioniraqeana100100No ratings yet
- Hypertension (HTN or HT), Also Known As High Blood Pressure (HBP), Is ADocument4 pagesHypertension (HTN or HT), Also Known As High Blood Pressure (HBP), Is AReynaKatNo ratings yet
- Cardiovascular Drugs and Blood Pressure RegulationDocument4 pagesCardiovascular Drugs and Blood Pressure RegulationReynaKatNo ratings yet
- Acute Heart FailureDocument18 pagesAcute Heart FailureGeorge GeorgeNo ratings yet
- Anti-Arrhythmic Agents For Pharmacy PDFDocument41 pagesAnti-Arrhythmic Agents For Pharmacy PDFKelvinTMaikanaNo ratings yet
- Cardiac Drugs HypertensionDocument5 pagesCardiac Drugs HypertensionEciOwnsMeNo ratings yet
- HypertensionDocument10 pagesHypertensionaa zzNo ratings yet
- Clinical Pharmacy 2023-2024 Lectures - 2Document104 pagesClinical Pharmacy 2023-2024 Lectures - 2ameerjawad150No ratings yet
- Lecture 1 antihypertensionSDSDocument7 pagesLecture 1 antihypertensionSDSSara AbbasNo ratings yet
- Cardiovascular Agents: Florianne E. Adlawan, R.NDocument31 pagesCardiovascular Agents: Florianne E. Adlawan, R.NadlawanflorianneNo ratings yet
- Lec 2 Heart Failure, Angina and Arryth2Document19 pagesLec 2 Heart Failure, Angina and Arryth2Adel AlomarNo ratings yet
- Cardiotonic DrugsDocument67 pagesCardiotonic DrugsLady Mae Ramos100% (1)
- Antianginal Drugs: Roger Joseph Ii R. Jecino, M.DDocument31 pagesAntianginal Drugs: Roger Joseph Ii R. Jecino, M.DFranz Earl Niño AlbesaNo ratings yet
- Heart Failure Drug Treatment GuideDocument45 pagesHeart Failure Drug Treatment GuideJoshua ObrienNo ratings yet
- Cardiovascular SystemDocument4 pagesCardiovascular SystemRegineCuasSulibNo ratings yet
- Cardiac Medications: Mildred YarboroughDocument51 pagesCardiac Medications: Mildred YarboroughQueennitaNo ratings yet
- Heart FailureDocument30 pagesHeart FailureYopih YohanesNo ratings yet
- DBP: Diastolic Blood Pressure SBP: Systolic Blood PressureDocument7 pagesDBP: Diastolic Blood Pressure SBP: Systolic Blood PressureM. JoyceNo ratings yet
- Cardiovascular Endocrinology and Metabolism: Theory and Practice of Cardiometabolic MedicineFrom EverandCardiovascular Endocrinology and Metabolism: Theory and Practice of Cardiometabolic MedicineAndrew J. KrentzNo ratings yet
- Hepatorenal Syndrome, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandHepatorenal Syndrome, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Eating Disorder Admission GuideDocument14 pagesEating Disorder Admission GuideJeremy Yang100% (1)
- Beethoven Pathetique Sonata AnalysisDocument3 pagesBeethoven Pathetique Sonata AnalysisJeremy YangNo ratings yet
- OSCE Shoulder ExaminationDocument6 pagesOSCE Shoulder ExaminationJeremy YangNo ratings yet
- Atrial Fibrillation Management PDFDocument3 pagesAtrial Fibrillation Management PDFJeremy YangNo ratings yet
- OSCE Station 1 Diabetic LL ExamDocument5 pagesOSCE Station 1 Diabetic LL ExamJeremy YangNo ratings yet
- Atrial Fibrillation Management PDFDocument3 pagesAtrial Fibrillation Management PDFJeremy YangNo ratings yet
- Scale Practice TableDocument1 pageScale Practice TableJeremy YangNo ratings yet
- Iacta 2011 Janak Mehta Award Winning PresentationDocument56 pagesIacta 2011 Janak Mehta Award Winning PresentationDr.Sandeep Kumar KarNo ratings yet
- Almostadoctor - co.Uk-Summary of ECG AbnormalitiesDocument8 pagesAlmostadoctor - co.Uk-Summary of ECG AbnormalitiesAnu SharmaNo ratings yet
- Simultaneous Atrial and Ventricular Pacing During Narrow Complex Tachycardia - The Janus Response. Which One Is True?Document5 pagesSimultaneous Atrial and Ventricular Pacing During Narrow Complex Tachycardia - The Janus Response. Which One Is True?Sahil HasanNo ratings yet
- ECG in Emergency Room, HowDocument43 pagesECG in Emergency Room, HowFabian Fabiansyah100% (1)
- ALTERATION/ ABNORMAL FINDINGS IN PULSEDocument7 pagesALTERATION/ ABNORMAL FINDINGS IN PULSEShalabh JoharyNo ratings yet
- ECG Rhythm InterpretationDocument21 pagesECG Rhythm Interpretationvanstar7100% (1)
- Rhythm Description Schematic Diagram Egc Characteristics Sample TraceDocument6 pagesRhythm Description Schematic Diagram Egc Characteristics Sample TraceJhenne Kyle Ko Dee100% (1)
- ArrhythmiasDocument29 pagesArrhythmiasVijay GadagiNo ratings yet
- Paroxysmal Supraventricular Tachycardia: Pathophysiology, Diagnosis, and ManagementDocument8 pagesParoxysmal Supraventricular Tachycardia: Pathophysiology, Diagnosis, and ManagementLaurensia Sherly SusiloNo ratings yet
- Ecg For AnkiDocument3 pagesEcg For AnkijNo ratings yet
- Emp SyncopeDocument20 pagesEmp SyncopeWilmer JimenezNo ratings yet
- Nurs 603 Assignment 1 Objective Tests Design and Considerations Final For SubmissionDocument13 pagesNurs 603 Assignment 1 Objective Tests Design and Considerations Final For Submissionapi-323169345No ratings yet
- Basic EKG RefresherDocument210 pagesBasic EKG RefresherAaron D. Phoenix100% (6)
- Ventricular Arrhythmias EP Overview MedtronicDocument44 pagesVentricular Arrhythmias EP Overview Medtronicinu_upNo ratings yet
- Important Causes of Sudden Cardiac DeathDocument2 pagesImportant Causes of Sudden Cardiac DeathTausif AbbasNo ratings yet
- KKH Baby Bear Book 2010 2nd EditionDocument305 pagesKKH Baby Bear Book 2010 2nd EditionErnest Ho100% (4)
- Drug StudyDocument9 pagesDrug StudyChristine PunsalanNo ratings yet
- A. Bayés de Luna (Auth.) Textbook of Clinical EDocument520 pagesA. Bayés de Luna (Auth.) Textbook of Clinical ETAUFAN RACHIMNo ratings yet
- Intepretasi EKG (DR Eka)Document93 pagesIntepretasi EKG (DR Eka)Danil Anugrah JayaNo ratings yet
- Chapter 12Document28 pagesChapter 12Muhammad AmirNo ratings yet
- From: Rapid Interpretation of EKG'sDocument14 pagesFrom: Rapid Interpretation of EKG'sLucija Kljaić100% (1)
- Clinical Indication Def.Document11 pagesClinical Indication Def.Anish H DaveNo ratings yet
- Medicine in The Pagan Arab StatesDocument134 pagesMedicine in The Pagan Arab StatesQurratu QolbiNo ratings yet
- ACLS Tachycardia Algorithm For Managing Stable TachycardiaDocument4 pagesACLS Tachycardia Algorithm For Managing Stable TachycardiaizkalotlNo ratings yet
- Heart Block PPT by SibaDocument36 pagesHeart Block PPT by Sibaritumitu_ritumitu100% (1)
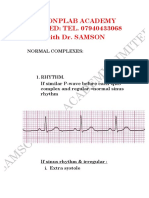
- ECG With DR Samson-1.Document10 pagesECG With DR Samson-1.Ebuwa AmadasunNo ratings yet
- AbbreviationDocument35 pagesAbbreviationroxy0709No ratings yet
- WPW SyndromeDocument6 pagesWPW SyndromeAlvin Wijaya RustamNo ratings yet
- A Simplified ECG GuideDocument4 pagesA Simplified ECG Guidejalan_z96% (25)
- Supraventricular Tachycardia - Life in The Fast Lane ECG LibraryDocument29 pagesSupraventricular Tachycardia - Life in The Fast Lane ECG LibraryYehuda Agus SantosoNo ratings yet