You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Clinical CaseDocument10 pagesClinical CaseRoberto RamosNo ratings yet
- Case 3Document8 pagesCase 3Roberto RamosNo ratings yet
- Rhie Full OcrDocument120 pagesRhie Full OcrRoberto RamosNo ratings yet
- Long Case Presentation FINAL-5Document7 pagesLong Case Presentation FINAL-5Roberto RamosNo ratings yet
- Case 4Document8 pagesCase 4Roberto RamosNo ratings yet
- Long Case Presentation FINAL-33Document7 pagesLong Case Presentation FINAL-33Roberto RamosNo ratings yet
- History: Chief Complaint: History of Present Illness: Patient Is A 59 Year Old G6 P1051 Woman Who Is An Inmate That WasDocument9 pagesHistory: Chief Complaint: History of Present Illness: Patient Is A 59 Year Old G6 P1051 Woman Who Is An Inmate That WasRoberto RamosNo ratings yet
- Case 2 AlmostDocument8 pagesCase 2 AlmostRoberto RamosNo ratings yet
- Universidad de Puerto Rico Mail - (No Subject)Document77 pagesUniversidad de Puerto Rico Mail - (No Subject)Roberto RamosNo ratings yet
- Soap RoutineDocument3 pagesSoap RoutineRoberto Ramos100% (1)
- Long Case Presentation FINAL-5Document7 pagesLong Case Presentation FINAL-5Roberto RamosNo ratings yet
- McCowan SGA RiskFactors BJOG 2010Document9 pagesMcCowan SGA RiskFactors BJOG 2010Roberto RamosNo ratings yet
- Repaso ShelfDocument135 pagesRepaso ShelfRoberto RamosNo ratings yet
- Paciente 3Document80 pagesPaciente 3Roberto RamosNo ratings yet
- Untitled Spreadsheet 2Document4 pagesUntitled Spreadsheet 2Roberto RamosNo ratings yet
- "Repaso" Shelf OB - GYN 2 2Document9 pages"Repaso" Shelf OB - GYN 2 2Roberto RamosNo ratings yet
- Final - Answers of Ekg QuizDocument46 pagesFinal - Answers of Ekg QuizRoberto RamosNo ratings yet
- Radio ObGynDocument1 pageRadio ObGynRoberto RamosNo ratings yet
- Progress Note Osce - HIV (1) - 2Document1 pageProgress Note Osce - HIV (1) - 2Roberto RamosNo ratings yet
- Universidad Puerto Rico Manual 1415Document161 pagesUniversidad Puerto Rico Manual 1415Roberto RamosNo ratings yet
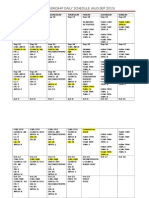
- OB-GYN Clerkship Daily ScheduleDocument3 pagesOB-GYN Clerkship Daily ScheduleRoberto RamosNo ratings yet
- Health Maintenance Cases For Discussion-5Document4 pagesHealth Maintenance Cases For Discussion-5Roberto RamosNo ratings yet
- There Is Been An Overlooked But Important TopicDocument2 pagesThere Is Been An Overlooked But Important TopicRoberto RamosNo ratings yet
- DR - Umpierrere2012 2013 4Document70 pagesDR - Umpierrere2012 2013 4Roberto RamosNo ratings yet
- There Is Been An Overlooked But Important TopicDocument2 pagesThere Is Been An Overlooked But Important TopicRoberto RamosNo ratings yet
- HTTPDocument1 pageHTTPRoberto RamosNo ratings yet
- HTTPDocument1 pageHTTPRoberto RamosNo ratings yet
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (894)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- DETAILED LESSON PLAN IN Health 9Document6 pagesDETAILED LESSON PLAN IN Health 9shiramae91% (11)
- Cervical Spine CYRIAXDocument16 pagesCervical Spine CYRIAXCarlos TavaresNo ratings yet
- What is Interventional Radiology in 38 CharactersDocument8 pagesWhat is Interventional Radiology in 38 CharactersNIMKY EMBER B. CLAMOHOYNo ratings yet
- Measles MorbiliDocument16 pagesMeasles MorbiliRegyna SusantiNo ratings yet
- Testicular CancerDocument48 pagesTesticular Cancerluckyswiss7776848No ratings yet
- Spiritual Needs of Dying PatientsDocument7 pagesSpiritual Needs of Dying PatientsLia Catalina Escobar SaldanaNo ratings yet
- Jurnal Placenta PreviaDocument9 pagesJurnal Placenta Previasheva25No ratings yet
- Causes and Pathophysiology of Cushing's Syndrome - UpToDateDocument15 pagesCauses and Pathophysiology of Cushing's Syndrome - UpToDateRoberto López MataNo ratings yet
- Non Healing UlcersDocument36 pagesNon Healing UlcersIniya RajendranNo ratings yet
- Health Financing Summit 2010 ReportDocument36 pagesHealth Financing Summit 2010 Reportpatburchall6278No ratings yet
- IlumaDocument2 pagesIlumaMaja Maja BułkaNo ratings yet
- Diagnosis and Examination in OrthopaedicsDocument34 pagesDiagnosis and Examination in OrthopaedicsinezNo ratings yet
- GORDON’S HEALTH PATTERN SUBMITTEDDocument6 pagesGORDON’S HEALTH PATTERN SUBMITTEDEnrique LuNo ratings yet
- MaprotilineDocument10 pagesMaprotilineAnonymous U4E6I1R100% (1)
- Patient Information SheetDocument1 pagePatient Information Sheetapi-354525636No ratings yet
- Pendekatan Klinis Penurunan PendengaranDocument29 pagesPendekatan Klinis Penurunan PendengaranHeather PorterNo ratings yet
- Acute Bronchitis and Chronic Bronchitis GuideDocument2 pagesAcute Bronchitis and Chronic Bronchitis GuideNica BaldicanasNo ratings yet
- Universal ECG Sample ReportsDocument6 pagesUniversal ECG Sample ReportsHemant Soni100% (1)
- ATROVENTDocument25 pagesATROVENTNúñez AlejandroNo ratings yet
- GLOVINGDocument4 pagesGLOVINGAngelene CalivaNo ratings yet
- 001-0 Complaint - 140723Document40 pages001-0 Complaint - 140723Anonymous GF8PPILW5No ratings yet
- Arogya Premier Policy WordingDocument30 pagesArogya Premier Policy WordingSyed AbudhakirNo ratings yet
- Career Fact Sheet-Selena1Document2 pagesCareer Fact Sheet-Selena1api-240236335No ratings yet
- Coarctation of The Aorta 1Document3 pagesCoarctation of The Aorta 1Zig OngNo ratings yet
- CGHS Empaneled HospitalsDocument61 pagesCGHS Empaneled HospitalsAshutosh SaxenaNo ratings yet
- Crisis Trauma: WWW - Eastzonemedico.co M WWW - Eastzonemedico.inDocument14 pagesCrisis Trauma: WWW - Eastzonemedico.co M WWW - Eastzonemedico.inswipetoplay32No ratings yet
- Study GuideDocument6 pagesStudy GuideFidelis MusicGroupNo ratings yet
- ConcussionDocument6 pagesConcussionradziah_mohdNo ratings yet
- Essay ListeriosisDocument7 pagesEssay ListeriosisNor Ashikin IsmailNo ratings yet
- Assessment Nursing Diagnosis Analysis Goals and Objectives Nursing Interventions Rationale Evaluation EffectivenessDocument3 pagesAssessment Nursing Diagnosis Analysis Goals and Objectives Nursing Interventions Rationale Evaluation EffectivenessYnah Sayoc75% (4)