You might also like
- PAKISTAN CUSTOMS TARIFF 2014-15Document348 pagesPAKISTAN CUSTOMS TARIFF 2014-15AliChana1No ratings yet
- 2167190Document20 pages2167190Umar FarooqNo ratings yet
- Force 30 Valleylab ManualDocument16 pagesForce 30 Valleylab ManualUmar FarooqNo ratings yet
- A Systematic Review of Graft Augmentation Urethroplasty Techniques For The Treatment of Anterior Urethral StricturesDocument18 pagesA Systematic Review of Graft Augmentation Urethroplasty Techniques For The Treatment of Anterior Urethral StricturesUmar FarooqNo ratings yet
- Higher Algebra - Hall & KnightDocument593 pagesHigher Algebra - Hall & KnightRam Gollamudi100% (2)
- AmputationsDocument30 pagesAmputationsUmar FarooqNo ratings yet
- Apr 02 14Document59 pagesApr 02 14Umar FarooqNo ratings yet
- Higher Algebra - Hall & KnightDocument593 pagesHigher Algebra - Hall & KnightRam Gollamudi100% (2)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5782)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (72)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Intramuscular CKLDocument2 pagesIntramuscular CKLapi-310181843No ratings yet
- Bio OssDocument4 pagesBio OssVizi AdrianNo ratings yet
- SinusitisDocument12 pagesSinusitis05-NH-HU-KEVIN JULIO HUAYLLANE SOLISNo ratings yet
- DescargaDocument173 pagesDescargaAlexander León PuelloNo ratings yet
- Solvalitt Aluminium - MSDSDocument11 pagesSolvalitt Aluminium - MSDSLITOGENT 893No ratings yet
- 2010 STEPS Report BangladeshDocument176 pages2010 STEPS Report Bangladeshfatehatun noorNo ratings yet
- ACWA MBR presents Submerged Membrane Bioreactors using the Kubota MembraneDocument48 pagesACWA MBR presents Submerged Membrane Bioreactors using the Kubota Membranecharles samsonNo ratings yet
- Prostho IV-Slides 2 - Assessment of The Edentulous PatientDocument60 pagesProstho IV-Slides 2 - Assessment of The Edentulous Patientبراءة أحمد السلاماتNo ratings yet
- Clean The Pressure Sore by Irrigating The WoundDocument3 pagesClean The Pressure Sore by Irrigating The WounddeardestinyNo ratings yet
- NarrativeDocument10 pagesNarrativesaikrish36No ratings yet
- Stugeron® TabletsDocument3 pagesStugeron® TabletsmahgadNo ratings yet
- Social and Emotional Well Being Framework 2004-2009Document79 pagesSocial and Emotional Well Being Framework 2004-2009MikeJacksonNo ratings yet
- Acellular MatricesDocument16 pagesAcellular MatricesElo MediavillaNo ratings yet
- Ganga Action PlanDocument18 pagesGanga Action PlanAjithEdathootNo ratings yet
- Chad ScoreDocument5 pagesChad ScoreakochaNo ratings yet
- Burn WoundDocument68 pagesBurn WoundjrefkyNo ratings yet
- Acetabular Labral Tears and Hip Scope Rehab Webinar HandoutDocument20 pagesAcetabular Labral Tears and Hip Scope Rehab Webinar Handoutgemichan26No ratings yet
- Sodium Valproate Uses, DosageDocument2 pagesSodium Valproate Uses, DosageKhairul KhairulNo ratings yet
- 3 2.Msds Shell GTL Sarawax Sx50v1915072016gbDocument18 pages3 2.Msds Shell GTL Sarawax Sx50v1915072016gbArturo BLANCAS MARTINEZNo ratings yet
- Amen ADD QuestionnaireDocument3 pagesAmen ADD QuestionnaireReeshabhdev GauttamNo ratings yet
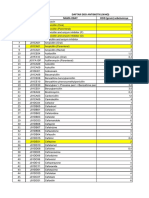
- DAFTAR ATC DDD ANTIBIOTIK WHO 2018 AbcDocument12 pagesDAFTAR ATC DDD ANTIBIOTIK WHO 2018 AbcMahezha DhewaNo ratings yet
- Listening and Reading Comprehension TestDocument12 pagesListening and Reading Comprehension TestPrimaIstianaNo ratings yet
- Brochure Rev04Document2 pagesBrochure Rev04nickj702No ratings yet
- PsychoanalysisDocument30 pagesPsychoanalysisjaydokNo ratings yet
- Drugs For Epilepsy: Subgroup 6Document31 pagesDrugs For Epilepsy: Subgroup 6Kwadwo Sarpong JnrNo ratings yet
- Case Presentation Ji Castante, Leah SDocument17 pagesCase Presentation Ji Castante, Leah SLeah CastanteNo ratings yet
- Effectiveness of Micronutrients and Physiotherapy in The Management of Oral Submucous Fibrosis PDFDocument5 pagesEffectiveness of Micronutrients and Physiotherapy in The Management of Oral Submucous Fibrosis PDFNia LieantoNo ratings yet
- ANSI/ASHRAE/ASHE Standard 170-2008 Tables for Filter Efficiencies and Design ParametersDocument4 pagesANSI/ASHRAE/ASHE Standard 170-2008 Tables for Filter Efficiencies and Design ParametersPradeep SukumaranNo ratings yet
- Cholestasis: Dr. Darmadi SPPD, FinasimDocument20 pagesCholestasis: Dr. Darmadi SPPD, FinasimTiens MonisaNo ratings yet
- Reflective QuestionsDocument2 pagesReflective Questionsayne joulceNo ratings yet