You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Disease of Adrenal Gland: Dr. Fatimah Eliana, SPPD, KemdDocument57 pagesDisease of Adrenal Gland: Dr. Fatimah Eliana, SPPD, KemdDeby Tri Widia LestariNo ratings yet
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- KadDocument25 pagesKadraisaNo ratings yet
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- GPQ 20 Jun08 PDFDocument4 pagesGPQ 20 Jun08 PDFDeby Tri Widia LestariNo ratings yet
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (894)
- Kuliah Obat Esensial Dan FormulariumDocument12 pagesKuliah Obat Esensial Dan FormulariumNita RahmatunnisaNo ratings yet
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Osteoporosis F DHDocument39 pagesOsteoporosis F DH95kodok85No ratings yet
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Japan Earthquake HighlightedDocument3 pagesJapan Earthquake HighlightedDeby Tri Widia LestariNo ratings yet
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Telmisartan AmlodipineDocument10 pagesTelmisartan AmlodipineDeby Tri Widia LestariNo ratings yet
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- HonkDocument11 pagesHonkYozhanNo ratings yet
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Cardiogenic Shock Hemodynamic ParametersDocument31 pagesCardiogenic Shock Hemodynamic ParameterscantikarevieraNo ratings yet
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- P Knowlesi PDFDocument3 pagesP Knowlesi PDFNurbieber Saiianklylavrilavigne BieberNo ratings yet
- Sexual Violence Sept 2014 152Document6 pagesSexual Violence Sept 2014 152Deby Tri Widia LestariNo ratings yet
- 0704 06Document4 pages0704 06Deby Tri Widia LestariNo ratings yet
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
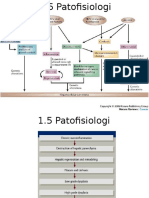
- 1.5 Patofisiologi Karsinoma HepatoselulerDocument2 pages1.5 Patofisiologi Karsinoma HepatoselulerDeby Tri Widia LestariNo ratings yet
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- Konsumsi Makanan Dan Kejadian Anemia Pada Siswi Salah Satu SMP Di Kota MakassarDocument4 pagesKonsumsi Makanan Dan Kejadian Anemia Pada Siswi Salah Satu SMP Di Kota MakassarTegoeh RizkiNo ratings yet
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Migraine Prevalence, Alexithymia, and Post-Traumatic StressDocument9 pagesMigraine Prevalence, Alexithymia, and Post-Traumatic StressDeby Tri Widia LestariNo ratings yet
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- NAP For Web - Headache Diagnosis TestingDocument38 pagesNAP For Web - Headache Diagnosis TestingDeby Tri Widia LestariNo ratings yet
- Headache QuestionnaireDocument10 pagesHeadache QuestionnairePerisha VeeraNo ratings yet
- IndianJMedSci6611-3703196 101711Document12 pagesIndianJMedSci6611-3703196 10171195kodok85No ratings yet
- Stress Dan AnxietasDocument4 pagesStress Dan AnxietasIhsan Rasyid YuldiNo ratings yet
- VaksinasiDocument9 pagesVaksinasiDeby Tri Widia LestariNo ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- 15Document5 pages15Deby Tri Widia LestariNo ratings yet
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- Epidemiological Investigation of A Temporal Increase in Atonic Postpartum Haemorrhage A Population-Based Retrospective Cohort StudyDocument10 pagesEpidemiological Investigation of A Temporal Increase in Atonic Postpartum Haemorrhage A Population-Based Retrospective Cohort StudyDeby Tri Widia LestariNo ratings yet
- Life Stress Test Score GuideDocument2 pagesLife Stress Test Score Guide95kodok85No ratings yet
- Prevalence of Anemia Risk Factors in Pregnant Women in Kerman, IranDocument4 pagesPrevalence of Anemia Risk Factors in Pregnant Women in Kerman, IranDeby Tri Widia LestariNo ratings yet
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Postpartum Haemorrhage in Midwifery Care in The Netherlands Validation of Quality Indicators For Midwifery GuidelinesDocument6 pagesPostpartum Haemorrhage in Midwifery Care in The Netherlands Validation of Quality Indicators For Midwifery GuidelinesDeby Tri Widia LestariNo ratings yet
- Prevalence of stress among medical studentsDocument7 pagesPrevalence of stress among medical studentsDeby Tri Widia LestariNo ratings yet
- Konsumsi Makanan Dan Kejadian Anemia Pada Siswi Salah Satu SMP Di Kota MakassarDocument4 pagesKonsumsi Makanan Dan Kejadian Anemia Pada Siswi Salah Satu SMP Di Kota MakassarTegoeh RizkiNo ratings yet
- Exsanguinated Uterus After Massive Atonic Postpartum HaemorrhageDocument4 pagesExsanguinated Uterus After Massive Atonic Postpartum HaemorrhageDeby Tri Widia LestariNo ratings yet
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Maternal Near Miss in Rural Hospital SudanDocument4 pagesMaternal Near Miss in Rural Hospital SudanVikas LonikarNo ratings yet
- PIH Renal Doppler Pregnancy - CutDocument4 pagesPIH Renal Doppler Pregnancy - CutAnonymous 9QxPDpNo ratings yet
- Hypertension in Pregnancy - The New ACOG Guidelines - John Barton, MDDocument69 pagesHypertension in Pregnancy - The New ACOG Guidelines - John Barton, MDJuwita Maggie Ogytha TandoNo ratings yet
- Pacheco-Romero, José Introduction To The Preeclampsia Revista Peruana de Ginecología y Obstetricia, Vol. 63, Núm. 2, 2017, Pp. 199-206 Sociedad Peruana de Obstetricia y Ginecología San Isidro, PerúDocument9 pagesPacheco-Romero, José Introduction To The Preeclampsia Revista Peruana de Ginecología y Obstetricia, Vol. 63, Núm. 2, 2017, Pp. 199-206 Sociedad Peruana de Obstetricia y Ginecología San Isidro, PerúAlessandraCarneroNeyraNo ratings yet
- Drug Study PreeclampsiaDocument14 pagesDrug Study PreeclampsiaBiway RegalaNo ratings yet
- Management of PreeclampsiaDocument11 pagesManagement of PreeclampsiaDanNo ratings yet
- Preeclampsia PDFDocument24 pagesPreeclampsia PDFAnghelino Jesus Meza CentenoNo ratings yet
- (PIH) CASE PRESENTATION (Group11)Document41 pages(PIH) CASE PRESENTATION (Group11)Kaye Drexcel SequilloNo ratings yet
- Chapter 40: Drugs Used in Obstetrics Test Bank: Multiple ChoiceDocument10 pagesChapter 40: Drugs Used in Obstetrics Test Bank: Multiple ChoiceNurse UtopiaNo ratings yet
- Maternal Safety Bundle For: Severe Hypertension in PregnancyDocument34 pagesMaternal Safety Bundle For: Severe Hypertension in PregnancyCarlos MayaNo ratings yet
- Book Garba SamskaraDocument3 pagesBook Garba SamskaraYogaguru NehaNo ratings yet
- Kompilasi - ICD MM Dan PM - Reference GuideDocument93 pagesKompilasi - ICD MM Dan PM - Reference GuidehijraNo ratings yet
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Pregnancy Hypertension CaseDocument7 pagesPregnancy Hypertension CaseRalph Emerson RatonNo ratings yet
- Nur 2310 Maternal Exam Questions and AnswersDocument80 pagesNur 2310 Maternal Exam Questions and AnswersNelson MandelaNo ratings yet
- Maternity Case 1: Olivia Jones (Core) : Guided Reflection QuestionsDocument3 pagesMaternity Case 1: Olivia Jones (Core) : Guided Reflection QuestionsDai Nguyen100% (1)
- Icd 10 Revisi 2010Document45 pagesIcd 10 Revisi 2010Lena ArdhiyantiNo ratings yet
- Hypertension in Pregnancy CorrectedDocument24 pagesHypertension in Pregnancy CorrectedPipipNo ratings yet
- IVFDocument46 pagesIVFKrissie LimNo ratings yet
- PreeclampsiaDocument13 pagesPreeclampsiaAnamikaNo ratings yet
- Welcome To NCM 104: Davao Doctors College, IncDocument212 pagesWelcome To NCM 104: Davao Doctors College, IncwindloverNo ratings yet
- Promotion of Nutrition Among Pregnant and Lactating MothersDocument12 pagesPromotion of Nutrition Among Pregnant and Lactating MothersGil GanibanNo ratings yet
- 0-Intial Pages Nandita ThesisDocument25 pages0-Intial Pages Nandita ThesisArunKumarNo ratings yet
- Is Zuspan Regimen Adequate For Preventing EclampsiDocument3 pagesIs Zuspan Regimen Adequate For Preventing EclampsiTimpswalo EmatsuloNo ratings yet
- Ritodrine and Other BetaDocument3 pagesRitodrine and Other BetaFaith Levi Alecha AlferezNo ratings yet
- Edit - HIL - Daily IGD 25.09.19Document30 pagesEdit - HIL - Daily IGD 25.09.19Inez WijayaNo ratings yet
- Competing Risks Model in Screening For Preeclampsia by Maternal Factors and Biomarkers at 11-13 Weeks GestationDocument12 pagesCompeting Risks Model in Screening For Preeclampsia by Maternal Factors and Biomarkers at 11-13 Weeks GestationmochkurniawanNo ratings yet
- Program EmasDocument8 pagesProgram EmasSavitri FazriNo ratings yet
- Pre-Eclampsia and EclampsiaDocument21 pagesPre-Eclampsia and EclampsiaTamratKelelegn100% (1)
- Recent Trends in PIHDocument21 pagesRecent Trends in PIHShashank VsNo ratings yet
- Management of Obstetric Emergencies Y5Document80 pagesManagement of Obstetric Emergencies Y5Charles Wilson83% (6)
- Hypertensive Disorders in PregnancyDocument6 pagesHypertensive Disorders in PregnancyLuiciaNo ratings yet
- Summary of The Body Keeps the Score: Brain, Mind, and Body in the Healing of Trauma by Bessel van der Kolk MDFrom EverandSummary of The Body Keeps the Score: Brain, Mind, and Body in the Healing of Trauma by Bessel van der Kolk MDRating: 4.5 out of 5 stars4.5/5 (167)
- Summary: The Myth of Normal: Trauma, Illness, and Healing in a Toxic Culture By Gabor Maté MD & Daniel Maté: Key Takeaways, Summary & AnalysisFrom EverandSummary: The Myth of Normal: Trauma, Illness, and Healing in a Toxic Culture By Gabor Maté MD & Daniel Maté: Key Takeaways, Summary & AnalysisRating: 4 out of 5 stars4/5 (9)
- The Upward Spiral: Using Neuroscience to Reverse the Course of Depression, One Small Change at a TimeFrom EverandThe Upward Spiral: Using Neuroscience to Reverse the Course of Depression, One Small Change at a TimeRating: 4.5 out of 5 stars4.5/5 (140)
- BORDERLINE PERSONALITY DISORDER: Help Yourself and Help Others. Articulate Guide to BPD. Tools and Techniques to Control Emotions, Anger, and Mood Swings. Save All Your Relationships and Yourself. NEW VERSIONFrom EverandBORDERLINE PERSONALITY DISORDER: Help Yourself and Help Others. Articulate Guide to BPD. Tools and Techniques to Control Emotions, Anger, and Mood Swings. Save All Your Relationships and Yourself. NEW VERSIONRating: 4.5 out of 5 stars4.5/5 (24)
- Rewire Your Anxious Brain: How to Use the Neuroscience of Fear to End Anxiety, Panic, and WorryFrom EverandRewire Your Anxious Brain: How to Use the Neuroscience of Fear to End Anxiety, Panic, and WorryRating: 4.5 out of 5 stars4.5/5 (157)
- The Happiness Trap: How to Stop Struggling and Start LivingFrom EverandThe Happiness Trap: How to Stop Struggling and Start LivingRating: 4 out of 5 stars4/5 (1)