You might also like
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (894)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- Kaldor's Reply to Criticism of his Theory on Productivity and GrowthDocument8 pagesKaldor's Reply to Criticism of his Theory on Productivity and GrowthPal SaruzNo ratings yet
- Data Mining SASDocument484 pagesData Mining SASpartying_shot100% (4)
- GARP 2023 FRM PART I-Book 2 - Quantitative AnalysisDocument296 pagesGARP 2023 FRM PART I-Book 2 - Quantitative Analysisivan arista100% (1)
- Compiled Notes: Mscfe 610 EconometricsDocument44 pagesCompiled Notes: Mscfe 610 EconometricsRahul DevtareNo ratings yet
- ML Project ReportDocument35 pagesML Project Reportveerabhadra100% (1)
- Customer Loyalty Marketing Research - A Comparative Approach Between Hospitality and Business JournalsDocument12 pagesCustomer Loyalty Marketing Research - A Comparative Approach Between Hospitality and Business JournalsM Syah RezaNo ratings yet
- Demographics of Overconfidence PDFDocument8 pagesDemographics of Overconfidence PDFNadeemNo ratings yet
- Trail Making Test: Normative Data For The Latin American Spanish Speaking Adult PopulationDocument23 pagesTrail Making Test: Normative Data For The Latin American Spanish Speaking Adult PopulationMarysabel Mendoza ApazaNo ratings yet
- IMC Unit2 v11Document20 pagesIMC Unit2 v11Munyaradzi Pasinawako0% (1)
- Binary Logistic Regression Analysis of IDocument16 pagesBinary Logistic Regression Analysis of IRay BoettgerNo ratings yet
- Principles of Biostatistics: Simple Linear RegressionDocument53 pagesPrinciples of Biostatistics: Simple Linear Regressionghosh71No ratings yet
- Btech Ai&Ds Ay2021-22 SyllabusDocument203 pagesBtech Ai&Ds Ay2021-22 Syllabusshubham VithalkarNo ratings yet
- CH E Problem 3Document3 pagesCH E Problem 3Brayan AguilarNo ratings yet
- Systematically Trading FX Mean Reversion in The Long Run 1680234492Document32 pagesSystematically Trading FX Mean Reversion in The Long Run 1680234492Jaehyun KimNo ratings yet
- Tribhuvan University Course Details for BIM 3rd SemesterDocument12 pagesTribhuvan University Course Details for BIM 3rd SemesterWave Wo100% (1)
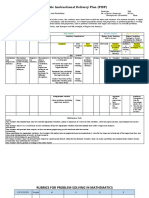
- Flexible Instructional Delivery Plan (FIDP) : What To Teach?Document3 pagesFlexible Instructional Delivery Plan (FIDP) : What To Teach?Arniel LlagasNo ratings yet
- STAT 2601 Test 3 Formula Sheet (Official)Document1 pageSTAT 2601 Test 3 Formula Sheet (Official)subui613No ratings yet
- Demand Forecasting Report Polyester Filament YarnDocument9 pagesDemand Forecasting Report Polyester Filament YarnPawan KumarNo ratings yet
- Importance Indices in Ethnobotany: Bruce Hoffman and Timothy GallaherDocument18 pagesImportance Indices in Ethnobotany: Bruce Hoffman and Timothy GallaherSucursal Piedras NegrasNo ratings yet
- The Influence of Accounting Software in Achieving The Internationalaccounting Standard Boards Qualitative Characteristics of Financial InformationDocument13 pagesThe Influence of Accounting Software in Achieving The Internationalaccounting Standard Boards Qualitative Characteristics of Financial InformationIJAR JOURNALNo ratings yet
- Regression Analysis with Cross-Sectional Data ExplainedDocument0 pagesRegression Analysis with Cross-Sectional Data ExplainedGabriel SimNo ratings yet
- Regional Studies in Marine Science: R.L. Boufeniza, M.M. Alsahli, N.I. Bachari, F. Houma BachariDocument10 pagesRegional Studies in Marine Science: R.L. Boufeniza, M.M. Alsahli, N.I. Bachari, F. Houma BachariHugo Pecho ChipaNo ratings yet
- Peterson 2009 RFS - Mitchell A - Double ClusterDocument46 pagesPeterson 2009 RFS - Mitchell A - Double ClusterEleanor RigbyNo ratings yet
- Journal of Building Engineering: SciencedirectDocument11 pagesJournal of Building Engineering: SciencedirectGülce Tunçbilek KarakayaNo ratings yet
- Thread ConsumptionDocument17 pagesThread ConsumptionMuhammad Hamza 18-NTU-0106No ratings yet
- Comm 2502 Practice Final S 2015Document8 pagesComm 2502 Practice Final S 2015Matt CohenNo ratings yet
- Marketing Research Project On StarbucksDocument49 pagesMarketing Research Project On StarbucksSalman Bin HabibNo ratings yet
- 6 - Measuring Price Promotion Effects - CasoDocument3 pages6 - Measuring Price Promotion Effects - CasoMarcela Fernandez100% (2)
- Pes University, Bangalore-85: Management StudiesDocument8 pagesPes University, Bangalore-85: Management StudiesshreeniNo ratings yet
- EE8702 - Power System Operation and Control (Ripped From Amazon Kindle Ebooks by Sai Seena)Document196 pagesEE8702 - Power System Operation and Control (Ripped From Amazon Kindle Ebooks by Sai Seena)19EEE009 Deepika SNo ratings yet