You might also like
- SWOT AnalysisDocument6 pagesSWOT Analysishananshahid96No ratings yet
- Solidwork Flow Simulation TutorialDocument298 pagesSolidwork Flow Simulation TutorialMilad Ah100% (8)
- HealthcareDocument57 pagesHealthcaredevadaskrishnanNo ratings yet
- Checklist For Mold RemediationDocument2 pagesChecklist For Mold Remediation631052No ratings yet
- Skype Sex - Date of Birth - Nationality: Curriculum VitaeDocument4 pagesSkype Sex - Date of Birth - Nationality: Curriculum VitaeSasa DjurasNo ratings yet
- p2 - Guerrero Ch13Document40 pagesp2 - Guerrero Ch13JerichoPedragosa88% (17)
- Nurse Deployment Program by DOHDocument23 pagesNurse Deployment Program by DOHGee Ridad74% (27)
- Case Study, g6Document62 pagesCase Study, g6julie pearl peliyoNo ratings yet
- Talon Star Trek Mod v0.2Document4 pagesTalon Star Trek Mod v0.2EdmundBlackadderIVNo ratings yet
- National Health PolicyDocument35 pagesNational Health PolicyLekshmi Manu100% (2)
- Special Proceedings Case DigestDocument14 pagesSpecial Proceedings Case DigestDyan Corpuz-Suresca100% (1)
- Health Care ReformDocument8 pagesHealth Care ReformAnjliNo ratings yet
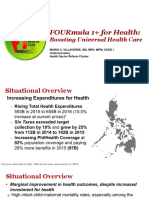
- 4 FOURmula 1 For Health Boosting Universal Health Care by DR Beverly HoDocument12 pages4 FOURmula 1 For Health Boosting Universal Health Care by DR Beverly HoJanella DandanNo ratings yet
- 2019 ASME Section V ChangesDocument61 pages2019 ASME Section V Changesmanisami7036100% (4)
- Introduction To HospitalDocument10 pagesIntroduction To HospitalAakansha DhadaseNo ratings yet
- AYUSHMAN BHARAT - Lec 7th SemDocument61 pagesAYUSHMAN BHARAT - Lec 7th SempriyankaNo ratings yet
- NHSRC - Operational Guidelines On Maternal and Newborn HealthDocument46 pagesNHSRC - Operational Guidelines On Maternal and Newborn HealthNational Child Health Resource Centre (NCHRC)No ratings yet
- National Rural Health Mission: Dr. Rajeshwar Rao ADocument37 pagesNational Rural Health Mission: Dr. Rajeshwar Rao Akuruvagadda sagarNo ratings yet
- National Health Policy-2017Document52 pagesNational Health Policy-2017Kailash NagarNo ratings yet
- Effects of War On EconomyDocument7 pagesEffects of War On Economyapi-3721555100% (1)
- Machine Tools Cutting FluidsDocument133 pagesMachine Tools Cutting FluidsDamodara MadhukarNo ratings yet
- Wargames Illustrated #115Document64 pagesWargames Illustrated #115Анатолий Золотухин100% (1)
- National Rural Health MissionDocument17 pagesNational Rural Health MissionShubham DwivediNo ratings yet
- Towards Universal Health Coverage HWCO 14 12 20 For WebDocument166 pagesTowards Universal Health Coverage HWCO 14 12 20 For WebhypersoftclientNo ratings yet
- DPMU Module PDFDocument315 pagesDPMU Module PDFkeyspNo ratings yet
- Evolution of Healthcare in Saudi ArabiaDocument41 pagesEvolution of Healthcare in Saudi ArabiaAmjadNo ratings yet
- Safety and Quality of Health Care System in IndiaDocument18 pagesSafety and Quality of Health Care System in IndiaKNOWLEDGE FeedNo ratings yet
- HRD in Health SectorDocument18 pagesHRD in Health SectorA Kaur MarwahNo ratings yet
- Understanding PHC Reviews and The Nigeria Planning and Implementation Framework - DR Eboreime EjemaiDocument34 pagesUnderstanding PHC Reviews and The Nigeria Planning and Implementation Framework - DR Eboreime EjemaiEjemai EboreimeNo ratings yet
- Group2 D IE HealthcareDocument33 pagesGroup2 D IE HealthcareSpandana AchantaNo ratings yet
- Challenges & Achievements of NRHMDocument3 pagesChallenges & Achievements of NRHMRenu R NairNo ratings yet
- Healthcare Management: BBA 503 Bba-V Semester Department of Management StudiesDocument17 pagesHealthcare Management: BBA 503 Bba-V Semester Department of Management Studiesvatsalya gaubaNo ratings yet
- 3 Health Care SystemDocument26 pages3 Health Care SystemAli HamzaNo ratings yet
- PRESENTATION: Asia Pacific's Health Trends-Obesity, NCDs and ADB's Operational Plan For Health 2015-2020Document40 pagesPRESENTATION: Asia Pacific's Health Trends-Obesity, NCDs and ADB's Operational Plan For Health 2015-2020ADB Health Sector GroupNo ratings yet
- NHSSP-Abridged-version NS 16.11.21.dir .22.11.21Document9 pagesNHSSP-Abridged-version NS 16.11.21.dir .22.11.21Sabina KontehNo ratings yet
- 3 Health Care SystemDocument27 pages3 Health Care SystemMuaaz Tahir Muaaz TahirNo ratings yet
- Core Resilientsustainablesystemsforhealth Infonote enDocument35 pagesCore Resilientsustainablesystemsforhealth Infonote enSponge BobNo ratings yet
- National Health Policy, Sustainable DevelopmentDocument115 pagesNational Health Policy, Sustainable DevelopmentMatei Sailo SailoNo ratings yet
- Human Resources For Public Health in India - Issues and ChallengesDocument13 pagesHuman Resources For Public Health in India - Issues and ChallengesHarikeshYadavNo ratings yet
- STANDARD F1+ PRESENTATION WITH NOTES FinalDocument15 pagesSTANDARD F1+ PRESENTATION WITH NOTES FinalMargaret Ani100% (2)
- DGHS IPHS CommunityHealthCentresDocument120 pagesDGHS IPHS CommunityHealthCentresSargam MahendruNo ratings yet
- Ingabire2015 PDFDocument6 pagesIngabire2015 PDFnofitaNo ratings yet
- Viewpoint: Healthcare Agenda For The Indian GovernmentDocument3 pagesViewpoint: Healthcare Agenda For The Indian GovernmentKahmishKhanNo ratings yet
- IHCDocument30 pagesIHCAbhijit PathakNo ratings yet
- Operational Guidelines For HWCDocument83 pagesOperational Guidelines For HWCharleenNo ratings yet
- Introduction of Health Care Services Under Ayushman Bharat Pradhan Mantri Jan Arogya Yojana AB (PM-JAY) - A Literature ReviewDocument6 pagesIntroduction of Health Care Services Under Ayushman Bharat Pradhan Mantri Jan Arogya Yojana AB (PM-JAY) - A Literature ReviewInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- NACHC 2022 Workforce Survey Full Report 1Document8 pagesNACHC 2022 Workforce Survey Full Report 1Bai Monisa GampongNo ratings yet
- 20-12 Lyst6901Document2 pages20-12 Lyst6901Samaira KhanNo ratings yet
- nhp2017 170426171207 PDFDocument52 pagesnhp2017 170426171207 PDFSaumitra SahaiNo ratings yet
- Government Hospital Project ReportDocument23 pagesGovernment Hospital Project ReportAditi JainNo ratings yet
- Operational Guidelines For Quality Assurance in Public Health Facilities 2013Document113 pagesOperational Guidelines For Quality Assurance in Public Health Facilities 2013baladhiliban100% (1)
- NIAHS Report PDFDocument218 pagesNIAHS Report PDFSwati Gorade100% (1)
- Organisational Behaviour: Sanjeet Singh & Yashmin SheikhDocument22 pagesOrganisational Behaviour: Sanjeet Singh & Yashmin SheikhSanjeet SinghNo ratings yet
- Pascal Zurn PASRC Policy Seminar 13 April 2022 SlidesDocument28 pagesPascal Zurn PASRC Policy Seminar 13 April 2022 Slidessaima FPONo ratings yet
- Rural HealthcareDocument13 pagesRural HealthcareIndia Heals-2020No ratings yet
- Family Planning 2020 Commitment: Govt. of IndiaDocument3 pagesFamily Planning 2020 Commitment: Govt. of Indiasandeepv08No ratings yet
- Policy Brief: Improving Health Workforce Planning and ManagementDocument10 pagesPolicy Brief: Improving Health Workforce Planning and ManagementMHIKIE MANZANARESNo ratings yet
- Health Care System in Pakistan .Document11 pagesHealth Care System in Pakistan .Shimmering MoonNo ratings yet
- Critical Review of Health Policy-2018 Updated (171206012)Document13 pagesCritical Review of Health Policy-2018 Updated (171206012)sdNo ratings yet
- 440.paper 2 Class 10 Health by @ImTgLokiDocument29 pages440.paper 2 Class 10 Health by @ImTgLokiprepcapfNo ratings yet
- National Health MissionDocument28 pagesNational Health Missionprabha krishnanNo ratings yet
- National Health Policy in India Goals, Objectives & RecommendationsDocument38 pagesNational Health Policy in India Goals, Objectives & RecommendationsRadhakrishnan TherivilaNo ratings yet
- Caronan NDP POLO HKGDocument23 pagesCaronan NDP POLO HKGKatrine Danielle GuardiansNo ratings yet
- The National Health Policy and MalnutritionDocument11 pagesThe National Health Policy and Malnutritiondishydashy88No ratings yet
- National Health Policy 2002 Goals and ObjectivesDocument72 pagesNational Health Policy 2002 Goals and Objectivesayushi rainaNo ratings yet
- National Health PolicyDocument34 pagesNational Health PolicydranshulitrivediNo ratings yet
- Amendola: HondurasDocument12 pagesAmendola: HondurasNewborn2013No ratings yet
- Issue Brief 5 CHWsDocument2 pagesIssue Brief 5 CHWsNay Lin HtikeNo ratings yet
- Lecture-1-Hcds-Prelim (20230921124305)Document26 pagesLecture-1-Hcds-Prelim (20230921124305)TEACHERNo ratings yet
- Health System Strengthening IndiaDocument4 pagesHealth System Strengthening Indiaumesh chhotalaNo ratings yet
- 1180 Project ReportDocument60 pages1180 Project Reportkarthikeyan01No ratings yet
- Khyber Pakhtunkhwa Health Sector Review: Hospital CareFrom EverandKhyber Pakhtunkhwa Health Sector Review: Hospital CareNo ratings yet
- Session 6A - Case Study On Myanmar - MIVillarroel PDFDocument16 pagesSession 6A - Case Study On Myanmar - MIVillarroel PDFKristine PresbiteroNo ratings yet
- Session 7-Fiscal Space - Juan M Villa PDFDocument31 pagesSession 7-Fiscal Space - Juan M Villa PDFKristine PresbiteroNo ratings yet
- Session 6B - Rep of Korea Experience - CKang PDFDocument19 pagesSession 6B - Rep of Korea Experience - CKang PDFKristine PresbiteroNo ratings yet
- Session 1-Social Protection Policies in Asia - DDYu PDFDocument48 pagesSession 1-Social Protection Policies in Asia - DDYu PDFKristine PresbiteroNo ratings yet
- Session 4 - Health Insurance Scheme of Rep Korea - Yun Suk-Myung PDFDocument20 pagesSession 4 - Health Insurance Scheme of Rep Korea - Yun Suk-Myung PDFKristine PresbiteroNo ratings yet
- Session 3 - Social Security Pension - Hagemejer - MCichon PDFDocument17 pagesSession 3 - Social Security Pension - Hagemejer - MCichon PDFKristine PresbiteroNo ratings yet
- Session 6B - Case Study On Mongolia - LCarraro PDFDocument14 pagesSession 6B - Case Study On Mongolia - LCarraro PDFKristine PresbiteroNo ratings yet
- Session 2-State of SP Financing in Asia - Michael Cichon PDFDocument25 pagesSession 2-State of SP Financing in Asia - Michael Cichon PDFKristine PresbiteroNo ratings yet
- Session 4 - Health Care Schemes - AWeber - MCichon PDFDocument12 pagesSession 4 - Health Care Schemes - AWeber - MCichon PDFKristine PresbiteroNo ratings yet
- Session 7 - Gambhir Bhatta PDFDocument7 pagesSession 7 - Gambhir Bhatta PDFKristine PresbiteroNo ratings yet
- Session 3-Social Assistance Schemes - FGassman PDFDocument17 pagesSession 3-Social Assistance Schemes - FGassman PDFKristine PresbiteroNo ratings yet
- Session 6A - Case Study On Timor-Leste - ABongestabs PDFDocument15 pagesSession 6A - Case Study On Timor-Leste - ABongestabs PDFKristine PresbiteroNo ratings yet
- Initial Poverty and Social AnalysisDocument3 pagesInitial Poverty and Social AnalysisKristine PresbiteroNo ratings yet
- APSP - Session 14B - Shamsul Alam - Social Protection and DRR-CCA-2Document7 pagesAPSP - Session 14B - Shamsul Alam - Social Protection and DRR-CCA-2Kristine PresbiteroNo ratings yet
- APSP Solo Lecture - N. Yoshino - SocialProtection Infra Aug04 2016Document28 pagesAPSP Solo Lecture - N. Yoshino - SocialProtection Infra Aug04 2016Kristine PresbiteroNo ratings yet
- APSP - Session 14B - San San Aye - Social Protection and DRMDocument17 pagesAPSP - Session 14B - San San Aye - Social Protection and DRMKristine PresbiteroNo ratings yet
- APSP - Session 14A - Sanjay ShahDocument26 pagesAPSP - Session 14A - Sanjay ShahKristine PresbiteroNo ratings yet
- CCT Design and Delivery Mechanism - ADBDocument30 pagesCCT Design and Delivery Mechanism - ADBKristine PresbiteroNo ratings yet
- APSP - Group 4 Recommendations - Better Monitoring Social Protection ProgramsDocument10 pagesAPSP - Group 4 Recommendations - Better Monitoring Social Protection ProgramsKristine PresbiteroNo ratings yet
- Shock-Responsive Social Protection in The PhilippinesDocument10 pagesShock-Responsive Social Protection in The PhilippinesKristine PresbiteroNo ratings yet
- APSP - Session 14B - Johanna Knoess (GIZ) - Asia Pacific Social Protection Week - 4.8.2016Document8 pagesAPSP - Session 14B - Johanna Knoess (GIZ) - Asia Pacific Social Protection Week - 4.8.2016Kristine PresbiteroNo ratings yet
- APSP - Session 14A - T. KoshyDocument8 pagesAPSP - Session 14A - T. KoshyKristine PresbiteroNo ratings yet
- APSP - Session 14A - Aurora Rubio - ICT For Social ProtectionDocument9 pagesAPSP - Session 14A - Aurora Rubio - ICT For Social ProtectionKristine PresbiteroNo ratings yet
- APSP - Group 5 Recommendations - Promoting Social Protection For Older PeopleDocument1 pageAPSP - Group 5 Recommendations - Promoting Social Protection For Older PeopleKristine PresbiteroNo ratings yet
- Apsp - Group 3 Recommendations - Ict InvestmentsDocument6 pagesApsp - Group 3 Recommendations - Ict InvestmentsKristine PresbiteroNo ratings yet
- APSP - Group 1 Recommendations - Sustainable Financing of Social Protection SystemsDocument5 pagesAPSP - Group 1 Recommendations - Sustainable Financing of Social Protection SystemsKristine PresbiteroNo ratings yet
- APSP - Group 2 Recommendations - Improving Delivery and Governance of Social ProtectionDocument5 pagesAPSP - Group 2 Recommendations - Improving Delivery and Governance of Social ProtectionKristine PresbiteroNo ratings yet
- APSP - Solo Lecture - Duncan Campbell - Labor Markets in The Digital EraDocument19 pagesAPSP - Solo Lecture - Duncan Campbell - Labor Markets in The Digital EraKristine PresbiteroNo ratings yet
- APSP - Session 10 - Mittal Shah - Emerging Issues in UHCDocument10 pagesAPSP - Session 10 - Mittal Shah - Emerging Issues in UHCKristine PresbiteroNo ratings yet
- PCG Master Consultancy Services AgreementDocument12 pagesPCG Master Consultancy Services Agreementawscobie100% (1)
- The Top 10 Strategic Technology Trends For 2020: Tomas Huseby Executive PartnerDocument31 pagesThe Top 10 Strategic Technology Trends For 2020: Tomas Huseby Executive PartnerCarlos Stuars Echeandia CastilloNo ratings yet
- BILL of Entry (O&A) PDFDocument3 pagesBILL of Entry (O&A) PDFHiJackNo ratings yet
- Developmen of Chick EmbryoDocument20 pagesDevelopmen of Chick Embryoabd6486733No ratings yet
- MP & MC Module-4Document72 pagesMP & MC Module-4jeezNo ratings yet
- Module 3 Paired and Two Sample T TestDocument18 pagesModule 3 Paired and Two Sample T TestLastica, Geralyn Mae F.No ratings yet
- 6a. ICMR STSDocument15 pages6a. ICMR STSVishnu Praba ANo ratings yet
- EasyLogic PM2000 Series - METSEPM2130Document4 pagesEasyLogic PM2000 Series - METSEPM2130ٍJordan SportNo ratings yet
- Amo Plan 2014Document4 pagesAmo Plan 2014kaps2385No ratings yet
- Assignment 2: Lesson Plan Analysis, Revision and Justification - Kaitlin Rose TrojkoDocument9 pagesAssignment 2: Lesson Plan Analysis, Revision and Justification - Kaitlin Rose Trojkoapi-408336810No ratings yet
- Experimental Investigation On The Properties of Compressed Earth Blocks Stabilised With A Liquid ChemicalDocument7 pagesExperimental Investigation On The Properties of Compressed Earth Blocks Stabilised With A Liquid ChemicalDeb Dulal TripuraNo ratings yet
- An Improved Ant Colony Algorithm and Its ApplicatiDocument10 pagesAn Improved Ant Colony Algorithm and Its ApplicatiI n T e R e Y eNo ratings yet
- Export - Import Cycle - PPSXDocument15 pagesExport - Import Cycle - PPSXMohammed IkramaliNo ratings yet
- Clinical Indications, Treatment and Current PracticeDocument14 pagesClinical Indications, Treatment and Current PracticefadmayulianiNo ratings yet
- Benefits of Eating OkraDocument4 pagesBenefits of Eating Okraama931No ratings yet
- Cuplock Scaffold 18mPHx1.6mx2.5m SafetyDocument1 pageCuplock Scaffold 18mPHx1.6mx2.5m SafetyDIGITAL SIRNo ratings yet
- SRC400C Rough-Terrain Crane 40 Ton Lifting CapacityDocument1 pageSRC400C Rough-Terrain Crane 40 Ton Lifting CapacityStephen LowNo ratings yet
- After EffectsDocument56 pagesAfter EffectsRodrigo ArgentoNo ratings yet