You might also like
- Chinese Herbal Medicine For Severe Acute Respiratory Syndrome A Systematic RevieDocument12 pagesChinese Herbal Medicine For Severe Acute Respiratory Syndrome A Systematic RevieRizqi Eko PNo ratings yet
- Culturing of Microbiology Specimens in LaboratoriesDocument100 pagesCulturing of Microbiology Specimens in Laboratoriestummalapalli venkateswara raoNo ratings yet
- Single Parent Households and The Effect On Student Learning PDFDocument69 pagesSingle Parent Households and The Effect On Student Learning PDFMalika AbdullahNo ratings yet
- Drug Study - MidazolamDocument2 pagesDrug Study - MidazolamKian HerreraNo ratings yet
- Congenital Clubfoot TreatmentDocument23 pagesCongenital Clubfoot TreatmentBernard Santoso0% (2)
- Clubfoot Anatomy, Causes, Diagnosis and TreatmentDocument74 pagesClubfoot Anatomy, Causes, Diagnosis and Treatmentnovia khairulbaria100% (2)
- Clinical Updates in the Management of Severe Asthma: New Strategies for Individualizing Long-term CareFrom EverandClinical Updates in the Management of Severe Asthma: New Strategies for Individualizing Long-term CareNo ratings yet
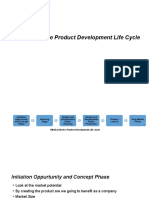
- Medical Device Product Development Life CycleDocument8 pagesMedical Device Product Development Life CycleSuresh Anand100% (1)
- Dental Materials 3rd Hatrick Test BankDocument12 pagesDental Materials 3rd Hatrick Test BankSaifoqqNo ratings yet
- Astm F-1185Document3 pagesAstm F-1185Pablo Cz100% (1)
- Applied Sciences: Post-Tuberculosis (TB) Treatment: The Role of Surgery and RehabilitationDocument18 pagesApplied Sciences: Post-Tuberculosis (TB) Treatment: The Role of Surgery and Rehabilitationraja yasminNo ratings yet
- Review: The Ef Ficacy and Safety of Probiotics in People With Cancer: A Systematic ReviewDocument11 pagesReview: The Ef Ficacy and Safety of Probiotics in People With Cancer: A Systematic ReviewNatália LopesNo ratings yet
- WHO Guidelines For The Programmatic Management of Drug-Resistant Tuberculosis: 2011 UpdateDocument13 pagesWHO Guidelines For The Programmatic Management of Drug-Resistant Tuberculosis: 2011 UpdateMuh FajriantoNo ratings yet
- Falzon ERJ 2011Document32 pagesFalzon ERJ 2011Mild PJantapanNo ratings yet
- Infection Control & Hospital EpidemiologyDocument9 pagesInfection Control & Hospital EpidemiologyRianNo ratings yet
- Servikal TBDocument15 pagesServikal TBnur wahidaNo ratings yet
- Treatment Outcomes of Multidrug-Resistant Tuberculosis: A Systematic Review and Meta-AnalysisDocument9 pagesTreatment Outcomes of Multidrug-Resistant Tuberculosis: A Systematic Review and Meta-AnalysisKamalina YustikariniNo ratings yet
- Jurnal Interna UTIDocument8 pagesJurnal Interna UTIErdika Satria WahyuonoNo ratings yet
- Makro LidDocument7 pagesMakro Liddoc_aswarNo ratings yet
- Plos Medicine /Article/Crossref/I /Article/Tw Itter/Info /Article/Metrics/Inf Info:Doi/10.1371/J Patient Adher 1185260400000Document25 pagesPlos Medicine /Article/Crossref/I /Article/Tw Itter/Info /Article/Metrics/Inf Info:Doi/10.1371/J Patient Adher 1185260400000khattak_i89No ratings yet
- Quinolonas en Neumonia Nosocomial Un IsDocument8 pagesQuinolonas en Neumonia Nosocomial Un IsIvan Ruiz HernandezNo ratings yet
- Early ViewDocument34 pagesEarly Viewyesid urregoNo ratings yet
- ÷, and A Number of Enteric GramDocument33 pages÷, and A Number of Enteric GramJohanna LehannaNo ratings yet
- Abx Empirica de NacDocument9 pagesAbx Empirica de NacMarcelo Jimenez CruzNo ratings yet
- Blood 2012 LudwigDocument43 pagesBlood 2012 LudwigRaquel LopesNo ratings yet
- WFSA UpdateDocument60 pagesWFSA UpdateSyaiful FatahNo ratings yet
- Rab 3Document8 pagesRab 3Belia DestamaNo ratings yet
- Impact of ASP in IcuDocument8 pagesImpact of ASP in Icuguilherme_ribeirNo ratings yet
- Fiber TreatmentDocument8 pagesFiber TreatmentLana AdilaNo ratings yet
- Chest: Health-Care-Associated Pneumonia Among Hospitalized Patients in A Japanese Community HospitalDocument8 pagesChest: Health-Care-Associated Pneumonia Among Hospitalized Patients in A Japanese Community HospitalAndi BintangNo ratings yet
- Wegener's Granulomatosis: Current and Upcoming Therapies: ReviewDocument12 pagesWegener's Granulomatosis: Current and Upcoming Therapies: ReviewAfif FaiziNo ratings yet
- Medicine American Journal of Hospice and PalliativeDocument6 pagesMedicine American Journal of Hospice and Palliativem1k0eNo ratings yet
- Fluoroquinolones Versus - Lactam Based Regimens For The Treatment of OsteomyelitisDocument8 pagesFluoroquinolones Versus - Lactam Based Regimens For The Treatment of OsteomyelitisFrank Barreiro SanchezNo ratings yet
- Ebn RespiDocument17 pagesEbn RespilablabkurmNo ratings yet
- Effect of Procalcitonin-Guided AntibioticDocument11 pagesEffect of Procalcitonin-Guided AntibioticRaul ContrerasNo ratings yet
- Outcome and Clinical Characteristics in Pleural Empyema: A Retrospective StudyDocument7 pagesOutcome and Clinical Characteristics in Pleural Empyema: A Retrospective StudylestarisurabayaNo ratings yet
- 6 FullDocument9 pages6 FullSukma EffendyNo ratings yet
- HHS Public AccessDocument15 pagesHHS Public AccessGustavo GomezNo ratings yet
- The Efficacy of Daily Chlorhexidine Bathing For Preventing Healthcare-Associated Infections in Adult Intensive Care UnitsDocument12 pagesThe Efficacy of Daily Chlorhexidine Bathing For Preventing Healthcare-Associated Infections in Adult Intensive Care UnitsKanameMizumiNo ratings yet
- PCT Guidance Reduces Antibiotic Use in CAPDocument10 pagesPCT Guidance Reduces Antibiotic Use in CAPmohd zonNo ratings yet
- Medi 99 E23649Document6 pagesMedi 99 E23649kornelis aribowoNo ratings yet
- TB treatment non-adherence EthiopiaDocument10 pagesTB treatment non-adherence EthiopiaCristopher OchoaNo ratings yet
- OutDocument8 pagesOutapi-284695722No ratings yet
- Dexamethason in ME TBDocument9 pagesDexamethason in ME TBYunita WidyaningsihNo ratings yet
- LeprosyDocument20 pagesLeprosyHafiz Sulistio UtomoNo ratings yet
- Afsharil 2011 Infection Cc11421Document8 pagesAfsharil 2011 Infection Cc11421giseladelarosa2006No ratings yet
- Full Text ADocument6 pagesFull Text AJoão NaveNo ratings yet
- Articulo NeumoniaDocument7 pagesArticulo NeumoniaEd BarajasNo ratings yet
- Corticosteroids For Managing Tuberculous Meningitis (Review)Document4 pagesCorticosteroids For Managing Tuberculous Meningitis (Review)ChangNo ratings yet
- Corticosteroids For Managing Tuberculous Meningitis (Review)Document4 pagesCorticosteroids For Managing Tuberculous Meningitis (Review)ChangNo ratings yet
- Pulmonary Impairment After Tuberculosis : Original ResearchDocument8 pagesPulmonary Impairment After Tuberculosis : Original ResearchPalaniappan MeyyappanNo ratings yet
- Chest.126.2.592 MBE EN UCIDocument9 pagesChest.126.2.592 MBE EN UCIJaime RomeroNo ratings yet
- Antibiotics 02 00001Document10 pagesAntibiotics 02 00001Jenny AlmagroNo ratings yet
- Muzii Et Al., 2020Document9 pagesMuzii Et Al., 2020Jonathan LucisNo ratings yet
- Antimicrobial ResistanceDocument11 pagesAntimicrobial Resistanceapi-253312159No ratings yet
- British Journal of Clinical PharmacologyDocument6 pagesBritish Journal of Clinical PharmacologyJunerey Hume Torres RodriguezNo ratings yet
- WJH 3 130bacteremiaDocument7 pagesWJH 3 130bacteremiaLasiaf AlaskaNo ratings yet
- Ciz 1049Document9 pagesCiz 1049Justin WilliemNo ratings yet
- Effect of Procalcitonin-Guided Antibiotic Treatment On Mortality in Acute Respiratory Infections: A Patient Level Meta-AnalysisDocument36 pagesEffect of Procalcitonin-Guided Antibiotic Treatment On Mortality in Acute Respiratory Infections: A Patient Level Meta-Analysisrista ria ariniNo ratings yet
- Procalcitonin and AB DecisionsDocument10 pagesProcalcitonin and AB DecisionsDennysson CorreiaNo ratings yet
- Meta-Analysis Evaluating Respiratory Fluoroquinolones For Community-Acquired PneumoniaDocument21 pagesMeta-Analysis Evaluating Respiratory Fluoroquinolones For Community-Acquired PneumoniaDiana Valeria Melo CNo ratings yet
- Pneumonia Treatment and DiagnosisDocument5 pagesPneumonia Treatment and Diagnosishusna fitriaNo ratings yet
- Korti Ko SteroidDocument7 pagesKorti Ko SteroidSisca AndrianyNo ratings yet
- CAP - PrinaDocument12 pagesCAP - PrinaSalNo ratings yet
- Adverse Drug Reactions of Primary Anti-tuberculosis DrugsDocument8 pagesAdverse Drug Reactions of Primary Anti-tuberculosis DrugsSelina WijayaNo ratings yet
- Dietary Supplement Use in Ambulatory Cancer Patients: A Survey On Prevalence, Motivation and AttitudesDocument9 pagesDietary Supplement Use in Ambulatory Cancer Patients: A Survey On Prevalence, Motivation and AttitudespilarerasoNo ratings yet
- Intranasal corticosteroids relieve sinusitis symptomsDocument9 pagesIntranasal corticosteroids relieve sinusitis symptomsagustinadianasariaguNo ratings yet
- 53-62 Barki S Et Al PDFDocument10 pages53-62 Barki S Et Al PDFnovia khairulbariaNo ratings yet
- Iaat14i12p644 PDFDocument8 pagesIaat14i12p644 PDFnovia khairulbariaNo ratings yet
- Diabetes Mellitus A Devastating Metabolic Disorder PDFDocument7 pagesDiabetes Mellitus A Devastating Metabolic Disorder PDFsshmitaaNo ratings yet
- Diabetes Mellitus Nair PDFDocument5 pagesDiabetes Mellitus Nair PDFWeng RamojalNo ratings yet
- Contoh Karakteristik SosialekonomiDocument10 pagesContoh Karakteristik Sosialekonominovia khairulbariaNo ratings yet
- Hipoglikemia PDFDocument12 pagesHipoglikemia PDFVhiny ChaNo ratings yet
- The Quality of Ambulatory Care Delivered To Children in The United StatesDocument9 pagesThe Quality of Ambulatory Care Delivered To Children in The United Statesnovia khairulbariaNo ratings yet
- Krisis Ekonomi Terhadap Kesehatan PDFDocument8 pagesKrisis Ekonomi Terhadap Kesehatan PDFnovia khairulbariaNo ratings yet
- Nej Mic M 1002094Document1 pageNej Mic M 1002094novia khairulbariaNo ratings yet
- Cardiovascular Complications of Diabetes ReviewDocument6 pagesCardiovascular Complications of Diabetes Reviewnovia khairulbariaNo ratings yet
- The Quality of Ambulatory Care Delivered To Children in The United StatesDocument9 pagesThe Quality of Ambulatory Care Delivered To Children in The United Statesnovia khairulbariaNo ratings yet
- Cochlear Implants For Children With Severe-to-Profound Hearing LossDocument8 pagesCochlear Implants For Children With Severe-to-Profound Hearing Lossnovia khairulbariaNo ratings yet
- Nej Me 1309006Document3 pagesNej Me 1309006novia khairulbariaNo ratings yet
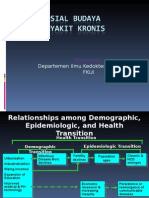
- Aspek Sosial BudayaDocument33 pagesAspek Sosial Budayanovia khairulbariaNo ratings yet
- Biaya Pengobatan Terhadap MDR PDFDocument10 pagesBiaya Pengobatan Terhadap MDR PDFnovia khairulbariaNo ratings yet
- Emergency Care in Fammed Practice PDFDocument25 pagesEmergency Care in Fammed Practice PDFnovia khairulbariaNo ratings yet
- Deteksi Dini KPDDocument52 pagesDeteksi Dini KPDMima Fatimah LuthfieNo ratings yet
- Cochlear Implants For Children With Severe-to-Profound Hearing LossDocument8 pagesCochlear Implants For Children With Severe-to-Profound Hearing Lossnovia khairulbariaNo ratings yet
- Rapid Assessment and Management of Trauma PatientsDocument92 pagesRapid Assessment and Management of Trauma PatientsRendi MuflihNo ratings yet
- Emergency and Disaster Risk ManagementDocument43 pagesEmergency and Disaster Risk Managementnovia khairulbariaNo ratings yet
- Emergency and Disaster Risk ManagementDocument43 pagesEmergency and Disaster Risk Managementnovia khairulbariaNo ratings yet
- Jurnal1 PDFDocument12 pagesJurnal1 PDFnovia khairulbariaNo ratings yet
- Presentation Damage Control in Thoracic SurgeryDocument44 pagesPresentation Damage Control in Thoracic Surgerynovia khairulbariaNo ratings yet
- Aspek Sosial BudayaDocument33 pagesAspek Sosial Budayanovia khairulbariaNo ratings yet
- Aspek Sosial BudayaDocument33 pagesAspek Sosial Budayanovia khairulbariaNo ratings yet
- Hipoglikemia PDFDocument12 pagesHipoglikemia PDFVhiny ChaNo ratings yet
- Hipoglikemia PDFDocument12 pagesHipoglikemia PDFVhiny ChaNo ratings yet
- Preparing for an English ExamDocument22 pagesPreparing for an English Examsukamto ilham100% (1)
- Oral Implants: The Paradigm Shift in Restorative Dentistry: JDR Centennial SeriesDocument7 pagesOral Implants: The Paradigm Shift in Restorative Dentistry: JDR Centennial SeriesShirmayne TangNo ratings yet
- Group 1 Ab12a4 Proposal Marketing PT 1 3Document13 pagesGroup 1 Ab12a4 Proposal Marketing PT 1 3쥬얼이No ratings yet
- Rapid Smart MethodologyDocument20 pagesRapid Smart MethodologyOscar Antún Castro HernándezNo ratings yet
- Ielts Speaking Transcript 1 3Document3 pagesIelts Speaking Transcript 1 3Hồng NhiNo ratings yet
- Zinc Reduces The Detection of Cocaine, Methamphetamine, and THC by ELISA Urine TestingDocument8 pagesZinc Reduces The Detection of Cocaine, Methamphetamine, and THC by ELISA Urine TestingParvatha SNo ratings yet
- (In Prague On 3 Sept 2007) : Dr. Masuda's TalksDocument27 pages(In Prague On 3 Sept 2007) : Dr. Masuda's TalksNestor GrahNo ratings yet
- Highcontainment BiolabsDocument84 pagesHighcontainment Biolabshansley cookNo ratings yet
- Behavior-Ethics-Leadership1 3322Document4 pagesBehavior-Ethics-Leadership1 3322api-515628516No ratings yet
- Exp. 9 Test For Vitamin CDocument5 pagesExp. 9 Test For Vitamin CClarice Catorce0% (1)
- Sabri T. Shuker - Maxillofacial Air-Containing Cavities, Blast Implosion Injuries, and ManagementDocument8 pagesSabri T. Shuker - Maxillofacial Air-Containing Cavities, Blast Implosion Injuries, and ManagementYamveaNo ratings yet
- Reflection Paper1 Psy111-1 A41Document1 pageReflection Paper1 Psy111-1 A41owyyyNo ratings yet
- Heart Disease rp2Document14 pagesHeart Disease rp2EkanshNo ratings yet
- Toprank Midterms Post TestDocument80 pagesToprank Midterms Post TestMaria Ana AguilarNo ratings yet
- APPLICATIONS FOR A DRIVING LICENCE AND ADDITION OF A NEW CLASS OF VEHICLE TO A DRIVING LICENCE (For Indian Citizen) PART - I.ÂDocument12 pagesAPPLICATIONS FOR A DRIVING LICENCE AND ADDITION OF A NEW CLASS OF VEHICLE TO A DRIVING LICENCE (For Indian Citizen) PART - I.ÂRahul UnnikrishnanNo ratings yet
- Cestodes Summary FinalsDocument2 pagesCestodes Summary FinalsKenneth Jake Batiduan100% (1)
- CIM PBL students' knowledge and attitudes towards PH healthcare referral systemDocument70 pagesCIM PBL students' knowledge and attitudes towards PH healthcare referral systemKurt CabahugNo ratings yet
- Week 7 Introduction To Nematodes PDFDocument5 pagesWeek 7 Introduction To Nematodes PDFewmedtechNo ratings yet
- 9700 s12 QP 23Document16 pages9700 s12 QP 23Farhad AliNo ratings yet
- 32 SMS - Cleaning Vessel (Air Line)Document6 pages32 SMS - Cleaning Vessel (Air Line)Mohd KhaidirNo ratings yet
- Grammar+HW-parallelism ADocument2 pagesGrammar+HW-parallelism Avijayendra koritalaNo ratings yet
- Theme 4 - Fixation and Stabilization of PRADDocument3 pagesTheme 4 - Fixation and Stabilization of PRADShany SchwarzwaldNo ratings yet
- CPS 2 ToxicologyDocument31 pagesCPS 2 ToxicologyNgọc Hà NguyễnNo ratings yet
- Informacion Del MonoetilenglicolDocument14 pagesInformacion Del MonoetilenglicolMartin Oscar Pacheco AlvarezNo ratings yet
- Deep Thoughts - PoemDocument2 pagesDeep Thoughts - Poemapi-462658463No ratings yet