You might also like
- Treatment: Ischemic StrokeDocument4 pagesTreatment: Ischemic StrokeGopi KrishnanNo ratings yet
- Intravenous Injection of Tissue Plasminogen Activator (tPA)Document2 pagesIntravenous Injection of Tissue Plasminogen Activator (tPA)Ralph Lorenz Avila AquinoNo ratings yet
- CABGDocument41 pagesCABGJasmin Jacob100% (2)
- Interventional NeuroradiologyDocument8 pagesInterventional NeuroradiologyAbhinav GuptaNo ratings yet
- Treatment of Ischemic StrokeDocument9 pagesTreatment of Ischemic Strokeka 66No ratings yet
- Coronary Artery DiseaseDocument9 pagesCoronary Artery DiseaseMariquita Buenafe100% (1)
- Clinical Pathway of Acute Stroke: Renz Darwin C. CastañadayDocument32 pagesClinical Pathway of Acute Stroke: Renz Darwin C. CastañadayRenz CastañadayNo ratings yet
- Coronary Angiogram and PCI GuideDocument9 pagesCoronary Angiogram and PCI Guideellaine0024100% (1)
- Heart CareDocument14 pagesHeart CareArman CareNo ratings yet
- Medical Procedure in Cardiogenic ShockDocument2 pagesMedical Procedure in Cardiogenic ShocksamsonNo ratings yet
- Neurovascular Conditions: Stroke and Transient Ischemic AttackDocument7 pagesNeurovascular Conditions: Stroke and Transient Ischemic AttackGinNo ratings yet
- Myocardial RevascularizationDocument3 pagesMyocardial Revascularizationapi-610954065No ratings yet
- Beating Surgery FinalDocument17 pagesBeating Surgery FinalSimon JosanNo ratings yet
- Stroke 1Document51 pagesStroke 1fatmaabdelazizNo ratings yet
- DX Dan TX StrokeDocument8 pagesDX Dan TX StrokeFirmansah SaputraNo ratings yet
- AngioplastyDocument10 pagesAngioplastyВлада ХоружийNo ratings yet
- PTCADocument51 pagesPTCAJasmin Jacob100% (1)
- Stroke PhilhealthDocument5 pagesStroke PhilhealthErwin BrionesNo ratings yet
- C P P C P P: Ardiology Atient AGE Ardiology Atient AGEDocument4 pagesC P P C P P: Ardiology Atient AGE Ardiology Atient AGEsatish_vsNo ratings yet
- Final Case Study - CADDocument109 pagesFinal Case Study - CADPatricia Marie Buenafe100% (1)
- Interventional Cardiology and SurgeryDocument19 pagesInterventional Cardiology and SurgeryDEV NANDHINI RNo ratings yet
- Aneurysm: TypesDocument12 pagesAneurysm: TypesSofia Isabelle GarciaNo ratings yet
- Endovascular Surgery - BenkőDocument33 pagesEndovascular Surgery - BenkőpampaszNo ratings yet
- Thorakales Aortenaneurysma DissertationDocument7 pagesThorakales Aortenaneurysma DissertationCustomWrittenPaperLittleRock100% (1)
- Aneurysmal Arterial Disease Is A Slow Process Through Which ArteriesDocument4 pagesAneurysmal Arterial Disease Is A Slow Process Through Which ArteriespritikachandNo ratings yet
- Carotid Artery Disease: Causes, Symptoms, Tests, and TreatmentDocument6 pagesCarotid Artery Disease: Causes, Symptoms, Tests, and TreatmentVijay Baskar SNo ratings yet
- Dust inDocument7 pagesDust inlarkspor31No ratings yet
- Heart and PericardiumDocument26 pagesHeart and PericardiumpalNo ratings yet
- 15A ArteryDocument72 pages15A Arterypavi7muruganathanNo ratings yet
- Biofluid Assignment 3Document6 pagesBiofluid Assignment 3Dina AssefaNo ratings yet
- Inside Blood Vessel Imaging TechniquesDocument3 pagesInside Blood Vessel Imaging TechniquesSai SridharNo ratings yet
- Assignment ON: TOPIC: PTCA (Percutaneous Transluminous Coronary Angioplasty)Document7 pagesAssignment ON: TOPIC: PTCA (Percutaneous Transluminous Coronary Angioplasty)soniya josephNo ratings yet
- Treat Acute Ischemic Stroke with Thrombolysis or ThrombectomyDocument3 pagesTreat Acute Ischemic Stroke with Thrombolysis or ThrombectomyXentur XenNo ratings yet
- New Options For Neurovascular DiseaseDocument3 pagesNew Options For Neurovascular DiseasecamillarugaNo ratings yet
- Ischemic Stroke: Let's Talk AboutDocument2 pagesIschemic Stroke: Let's Talk AboutAlexandra OpreaNo ratings yet
- Interventional RadiologyDocument53 pagesInterventional Radiologypri_29275% (4)
- Understanding Subdural Hematomas - Causes, Symptoms and TreatmentDocument54 pagesUnderstanding Subdural Hematomas - Causes, Symptoms and TreatmentNuzhat Noor Ayesha100% (1)
- pe-aneurruptDocument4 pagespe-aneurruptrungthanaporn4No ratings yet
- Mi DrugsDocument5 pagesMi DrugsKing Nehpets AlczNo ratings yet
- Brain AneurysmDocument2 pagesBrain Aneurysmmactrina100% (1)
- Cerebral Aneurysms: Aneurysms Posterior Circulation Basilar Artery Vertebral Arteries Posterior Communicating ArteryDocument10 pagesCerebral Aneurysms: Aneurysms Posterior Circulation Basilar Artery Vertebral Arteries Posterior Communicating ArteryRani SujithNo ratings yet
- Bypass SurgeryDocument1 pageBypass Surgeryandrzej36No ratings yet
- 4 - Surgical Interventions, Monitoring and SupportDocument32 pages4 - Surgical Interventions, Monitoring and Supportmaira ShahzadNo ratings yet
- Heart Disease and Heart Bypass SurgeryDocument3 pagesHeart Disease and Heart Bypass SurgeryAuladi Lubis ∑No ratings yet
- Consent Carotid StentingDocument13 pagesConsent Carotid StentingAbhinav GuptaNo ratings yet
- IGCSE BioDocument5 pagesIGCSE BioMajid DardasNo ratings yet
- Angioplasty and Vascular StentingDocument8 pagesAngioplasty and Vascular Stentingrajnishpathak648No ratings yet
- Neurovascular Conditions Treated at PennDocument7 pagesNeurovascular Conditions Treated at PennFatrawati BahuaNo ratings yet
- Regie Delariarte, Trexie Dipa - Khrystle Dote, Clarice Estores BN3A October 3, 2017Document4 pagesRegie Delariarte, Trexie Dipa - Khrystle Dote, Clarice Estores BN3A October 3, 2017random sharkNo ratings yet
- Rle RequirementDocument101 pagesRle RequirementJe KirsteneNo ratings yet
- Angioplasty: Made By: Group 2 8A Drea (05) Keane (11) Kimberly (12) VarrelDocument7 pagesAngioplasty: Made By: Group 2 8A Drea (05) Keane (11) Kimberly (12) VarrelkimberlyNo ratings yet
- PCI Procedures ExplainedDocument24 pagesPCI Procedures Explainedshejila c hNo ratings yet
- Carotid Stenosis (Carotid Artery Disease)Document5 pagesCarotid Stenosis (Carotid Artery Disease)Pieter SteenkampNo ratings yet
- StrokeDocument7 pagesStrokeD/Badr Saleh Al jabryNo ratings yet
- A Stroke RecoveryDocument2 pagesA Stroke Recoverymanjukumard2007No ratings yet
- TIADocument22 pagesTIAArabylle Maranca AbuelNo ratings yet
- AngioplastyDocument2 pagesAngioplastysubirghosh1100% (1)
- Arterial Disease GuideDocument34 pagesArterial Disease GuideIphie Ivanna OctavianiNo ratings yet
- STROKE: Handbook with activities, exercises and mental challengesFrom EverandSTROKE: Handbook with activities, exercises and mental challengesNo ratings yet
- A Simple Guide to Vascular Diseases, Diagnosis, Treatment and Related ConditionsFrom EverandA Simple Guide to Vascular Diseases, Diagnosis, Treatment and Related ConditionsNo ratings yet
- 1Document4 pages1Gopi KrishnanNo ratings yet
- Informed ConsentDocument1 pageInformed ConsentGopi KrishnanNo ratings yet
- Chest Physiotherapy or Techniques in Cardio Pulmonary Physiotherapy A Running CommentaryDocument5 pagesChest Physiotherapy or Techniques in Cardio Pulmonary Physiotherapy A Running CommentaryGopi KrishnanNo ratings yet
- VishakDocument2 pagesVishakGopi KrishnanNo ratings yet
- ConferenceDocument1 pageConferenceGopi KrishnanNo ratings yet
- Background and ObjectivesDocument2 pagesBackground and ObjectivesGopi KrishnanNo ratings yet
- FythqsgxchcsxjDocument1 pageFythqsgxchcsxjGopi KrishnanNo ratings yet
- MET knee extension testsDocument7 pagesMET knee extension testsGopi KrishnanNo ratings yet
- UgqsuguwsgugixhiDocument1 pageUgqsuguwsgugixhiGopi KrishnanNo ratings yet
- LefsDocument1 pageLefsGopi KrishnanNo ratings yet
- UgqsuguwsgugixhiDocument1 pageUgqsuguwsgugixhiGopi KrishnanNo ratings yet
- Acknowledgement: and Sports Medicine), Vice Principal, Bethany Navajeevan College of Physiotherapy, For HerDocument1 pageAcknowledgement: and Sports Medicine), Vice Principal, Bethany Navajeevan College of Physiotherapy, For HerGopi KrishnanNo ratings yet
- 719 SMA InjuryBrochure Hamstring - Web PDFDocument4 pages719 SMA InjuryBrochure Hamstring - Web PDFGopi KrishnanNo ratings yet
- Informed ConsentDocument1 pageInformed ConsentGopi KrishnanNo ratings yet
- GOPIKRISHNANDocument1 pageGOPIKRISHNANGopi KrishnanNo ratings yet
- Physiotherapy in Orthopeadic ConditionsDocument2 pagesPhysiotherapy in Orthopeadic ConditionsGopi KrishnanNo ratings yet
- Gopikrishnan.C.G: Career ObjectiveDocument4 pagesGopikrishnan.C.G: Career ObjectiveGopi KrishnanNo ratings yet
- Comparative Study Between Muscle Energy Techinque and Eccentric Training in Improving Hamstring Muscle Flexibility and Performance in Male College Athlete1Document3 pagesComparative Study Between Muscle Energy Techinque and Eccentric Training in Improving Hamstring Muscle Flexibility and Performance in Male College Athlete1Gopi KrishnanNo ratings yet
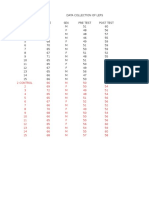
- Name: Age: Sex: Date:: Data Collection SheetDocument1 pageName: Age: Sex: Date:: Data Collection SheetGopi KrishnanNo ratings yet
- Gopi KrishnanDocument1 pageGopi KrishnanGopi KrishnanNo ratings yet
- Brochure PDFDocument2 pagesBrochure PDFGopi KrishnanNo ratings yet
- The Use of Surface Electromyography in Biomechanics PDFDocument29 pagesThe Use of Surface Electromyography in Biomechanics PDFRaul Enrique Castillo VeraNo ratings yet
- ARDS GuidelinesDocument18 pagesARDS GuidelinesGopi KrishnanNo ratings yet
- Ygwq 89 Yp UP8 ADocument1 pageYgwq 89 Yp UP8 AGopi KrishnanNo ratings yet
- 212700554/sport Speed and Agility Training 2dnDocument1 page212700554/sport Speed and Agility Training 2dnGopi KrishnanNo ratings yet
- Critical care approach to poisoned patientsDocument90 pagesCritical care approach to poisoned patientsGopi KrishnanNo ratings yet
- Critical care approach to poisoned patientsDocument90 pagesCritical care approach to poisoned patientsGopi KrishnanNo ratings yet
- Electrocardiograms - BasicDocument47 pagesElectrocardiograms - BasicGopi KrishnanNo ratings yet
- Cardiac SupportDocument8 pagesCardiac SupportGopi KrishnanNo ratings yet
- Posterior Cruciate Ligament InjuriesDocument26 pagesPosterior Cruciate Ligament InjuriesGopi KrishnanNo ratings yet
- Capillary MalformationsDocument7 pagesCapillary MalformationsDyah Ayu PitasariNo ratings yet
- Anesthesia For Neurosurgery in Infants and Children: Barbara Van de Wiele, M.D. Los Angeles, CaliforniaDocument24 pagesAnesthesia For Neurosurgery in Infants and Children: Barbara Van de Wiele, M.D. Los Angeles, CaliforniaKamel HadyNo ratings yet
- Arterial Doppler Waveforms: Understanding Hemodynamic PrinciplesDocument21 pagesArterial Doppler Waveforms: Understanding Hemodynamic PrinciplesL0v3B00k5100% (6)
- Cerebral Developmental Venous AnomaliesDocument12 pagesCerebral Developmental Venous AnomaliespincitopinNo ratings yet
- NCM 104 Midterm Exams - 1Document21 pagesNCM 104 Midterm Exams - 1Bing58No ratings yet
- Subarachnoid HemorrhageDocument3 pagesSubarachnoid Hemorrhagetenaj_purpleNo ratings yet
- Case Study CVDDocument49 pagesCase Study CVDzerpthederpNo ratings yet
- AHA ASA-AV Malformation 2017Document25 pagesAHA ASA-AV Malformation 2017Kym DominguezNo ratings yet
- Vascular Malformation Types, Causes, Diagnosis and TreatmentDocument37 pagesVascular Malformation Types, Causes, Diagnosis and TreatmentDudu LeeNo ratings yet
- AvmDocument6 pagesAvmWafya RamschieNo ratings yet
- ScoppingDocument10 pagesScoppingRizky Angga PNo ratings yet
- Hereditary Hemorrhagic Telangiectasia (HHT)Document15 pagesHereditary Hemorrhagic Telangiectasia (HHT)MarshallNo ratings yet
- Congenital Vascular MalformationsDocument19 pagesCongenital Vascular MalformationsBonny KoerniaNo ratings yet
- Therapeutic Interventions in Vascular MalformationsDocument47 pagesTherapeutic Interventions in Vascular MalformationsDr KhanNo ratings yet
- AVM Pediatric LilleDocument9 pagesAVM Pediatric LilleZdravko HeinrichNo ratings yet
- Journal Reading: Imaging of Intracranial HemorrhageDocument27 pagesJournal Reading: Imaging of Intracranial HemorrhagehasrilNo ratings yet
- Intraosseous Arteriovenous Malformations Mimicking Malignant DiseaseDocument7 pagesIntraosseous Arteriovenous Malformations Mimicking Malignant DiseaseNm SNo ratings yet
- Osler-Weber-Rendu Disease - StatPearls - NCBI BookshelfDocument4 pagesOsler-Weber-Rendu Disease - StatPearls - NCBI BookshelfanaNo ratings yet
- Fistulas and Fissures - Types, Symptoms, Causes, and Treatment - Pavlovich, DmitriDocument212 pagesFistulas and Fissures - Types, Symptoms, Causes, and Treatment - Pavlovich, DmitriKaranja Gitau100% (1)
- Color Atlas of Vascular Tumors and Vascular Malformations (Enjolras)Document310 pagesColor Atlas of Vascular Tumors and Vascular Malformations (Enjolras)Ciprian-Nicolae Muntean100% (1)
- Proceedings of The 2014 Spring Meeting of The Society of British 2014Document40 pagesProceedings of The 2014 Spring Meeting of The Society of British 2014rabiatul adawiyahNo ratings yet
- Jurnal Reading: Imaging in Acute StrokeDocument30 pagesJurnal Reading: Imaging in Acute StrokeBejo LanangNo ratings yet
- International Neurovascular Course: Multimodality Management of Intracranial and Spinal AvmsDocument6 pagesInternational Neurovascular Course: Multimodality Management of Intracranial and Spinal AvmsAmmar KadariNo ratings yet
- Laser RX VADocument62 pagesLaser RX VAhaneefmdfNo ratings yet
- What Is A Brain AVMDocument5 pagesWhat Is A Brain AVMCj UritaNo ratings yet
- Maria Citcos: Cap. 1 Cap. 1 Cap. 1 Cap. 1 Cap. 1 Cap. 2 Cap. 3 Cap. 6 Cap. 7 Cap. 1 Cap. 5 Cap. 4 Cap. 3 Cap. 4 Cap. 4Document11 pagesMaria Citcos: Cap. 1 Cap. 1 Cap. 1 Cap. 1 Cap. 1 Cap. 2 Cap. 3 Cap. 6 Cap. 7 Cap. 1 Cap. 5 Cap. 4 Cap. 3 Cap. 4 Cap. 4Smaranda-Elena MateiNo ratings yet
- Issva Classification 2014 Final TrialDocument20 pagesIssva Classification 2014 Final TrialFrancis MunguíaNo ratings yet
- Vascular Lesions of the Brain Classification and TreatmentDocument6 pagesVascular Lesions of the Brain Classification and TreatmentAlyssa NadiaNo ratings yet