You might also like
- Wahyuningtyas Et Al - Final - Nov2018 - 1-S2.0-S2212816618300131-MainDocument9 pagesWahyuningtyas Et Al - Final - Nov2018 - 1-S2.0-S2212816618300131-MainEkaSaktiWahyuningtyasNo ratings yet
- HNS EkaDocument9 pagesHNS EkaEkaSaktiWahyuningtyasNo ratings yet
- SSC Coo RRPP..CC Oom M: Ssa Am MPP LleeDocument2 pagesSSC Coo RRPP..CC Oom M: Ssa Am MPP LleeEkaSaktiWahyuningtyasNo ratings yet
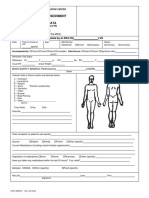
- Initial Nursing Assessment and Admission Data PDFDocument7 pagesInitial Nursing Assessment and Admission Data PDFEkaSaktiWahyuningtyasNo ratings yet
- Content ServerDocument4 pagesContent ServerEkaSaktiWahyuningtyasNo ratings yet
- Initial Nursing Assessment and Admission Data PDFDocument7 pagesInitial Nursing Assessment and Admission Data PDFEkaSaktiWahyuningtyasNo ratings yet
- Gordon's Functional Health PatternDocument2 pagesGordon's Functional Health PatternAnn Michelle Tarrobago100% (1)
- Gordon's Functional Health PatternDocument2 pagesGordon's Functional Health PatternAnn Michelle Tarrobago100% (1)
- Visual Analogue Scale (VAS-F) SAMPLEDocument4 pagesVisual Analogue Scale (VAS-F) SAMPLEEkaSaktiWahyuningtyasNo ratings yet
- Stroke 2012 Navi 1484 9Document8 pagesStroke 2012 Navi 1484 9EkaSaktiWahyuningtyasNo ratings yet
- Palliative Cancer Care in Middle Eastern CountriesDocument29 pagesPalliative Cancer Care in Middle Eastern CountriesEkaSaktiWahyuningtyasNo ratings yet
- Fatigue Severity ScaleDocument1 pageFatigue Severity ScaleAffuadiNo ratings yet
- DAPUSDocument1 pageDAPUSEkaSaktiWahyuningtyasNo ratings yet
- Daftar PustakaDocument1 pageDaftar PustakaEkaSaktiWahyuningtyasNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (894)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Coalition lobbyists see jobs boomDocument2 pagesCoalition lobbyists see jobs boomdoxagnosticNo ratings yet
- Chiongbian v. de Leon GR No. L-2007Document4 pagesChiongbian v. de Leon GR No. L-2007AnonymousNo ratings yet
- Crusade Prayer BookDocument59 pagesCrusade Prayer Bookmaria1grazia1mazzaNo ratings yet
- Summary of Plato's Republic - RevisedDocument5 pagesSummary of Plato's Republic - RevisedJhoice Ramirez Mactal100% (3)
- People vs. NuñezDocument28 pagesPeople vs. NuñezLourdes LescanoNo ratings yet
- Reported Speech ExercisesDocument4 pagesReported Speech ExercisesPatricia LorenzoNo ratings yet
- Book CatalogueDocument63 pagesBook CatalogueSomaCruz2xNo ratings yet
- Anti-Rape (Investigation and Trial) Ordinance, 2020Document12 pagesAnti-Rape (Investigation and Trial) Ordinance, 2020Farman KhanNo ratings yet
- Julious Caesar TranscriptDocument1 pageJulious Caesar TranscriptningruanantaNo ratings yet
- NEAJ Article on AraquioDocument4 pagesNEAJ Article on AraquioChristian Edezon LopezNo ratings yet
- What Is PrayerDocument4 pagesWhat Is PrayermbekosobizzyNo ratings yet
- People of The Philippines vs. Jose Belmar Umapas Y Crisostomo GR. No. 215742, March 22, 2017 FactsDocument1 pagePeople of The Philippines vs. Jose Belmar Umapas Y Crisostomo GR. No. 215742, March 22, 2017 FactsdnzrckNo ratings yet
- He Imes Eader: White House: Bin Laden UnarmedDocument44 pagesHe Imes Eader: White House: Bin Laden UnarmedThe Times LeaderNo ratings yet
- The Love RevolutionDocument2 pagesThe Love RevolutionEuniceNo ratings yet
- Camaya Vs PatulandongDocument5 pagesCamaya Vs PatulandongJesstonieCastañaresDamayoNo ratings yet
- Bellefonte Walkout Letter To ParentsDocument1 pageBellefonte Walkout Letter To ParentsMatt StevensNo ratings yet
- Makati City charter provisions challengedDocument2 pagesMakati City charter provisions challengedJovelan V. EscañoNo ratings yet
- Drug Abuse - Effects and Solutions (Informal Letter)Document6 pagesDrug Abuse - Effects and Solutions (Informal Letter)Qing Yi0% (1)
- Balance of Probabilities and The RuleDocument5 pagesBalance of Probabilities and The RuleGNo ratings yet
- An Institutional History of The LTTEDocument96 pagesAn Institutional History of The LTTEeelamviewNo ratings yet
- Ethical and Legal Issues in The Patient Care Continuum: Dr. Hector Gerard C. Belisario ABCD Law FirmDocument27 pagesEthical and Legal Issues in The Patient Care Continuum: Dr. Hector Gerard C. Belisario ABCD Law FirmCHRISTIAN HARVEY WONGNo ratings yet
- SSC GK History Notes - Mughal Empire Part IVDocument6 pagesSSC GK History Notes - Mughal Empire Part IVMalu SakthiNo ratings yet
- Origin and Evolution of The Society With Reference To Aggannasutta of DDocument1 pageOrigin and Evolution of The Society With Reference To Aggannasutta of DLong ShiNo ratings yet
- Talking in a New LandDocument33 pagesTalking in a New LandCn' TraveLog80% (5)
- Psychotropic Drug Overdose The Death of The Hollywood Celebrity Heath LedgerDocument5 pagesPsychotropic Drug Overdose The Death of The Hollywood Celebrity Heath LedgerlalipredebonNo ratings yet
- Tuana Coming To Understand Orgasm and The Epistemology of IgnoranceDocument40 pagesTuana Coming To Understand Orgasm and The Epistemology of IgnoranceEmilyR.DouglasNo ratings yet
- Oil and Water? The Philosophical Commitments of International Peace Studies and Conflict ResolutionDocument33 pagesOil and Water? The Philosophical Commitments of International Peace Studies and Conflict ResolutionCiurescu Simona100% (1)
- Fassmer Opv2020 Navy Vessels Technical DataDocument4 pagesFassmer Opv2020 Navy Vessels Technical DataVictor PileggiNo ratings yet
- Quotes For PageDocument161 pagesQuotes For PageSteve DurchinNo ratings yet
- F-15 Strike Eagle HandbookDocument228 pagesF-15 Strike Eagle Handbookremow89% (9)