You might also like
- The Impact of Meta-Strategy On Attendance DynamicsDocument13 pagesThe Impact of Meta-Strategy On Attendance DynamicstansoeiNo ratings yet
- Data Science Comprehensive OverviewDocument42 pagesData Science Comprehensive OverviewtansoeiNo ratings yet
- Knowns and UnknownsDocument26 pagesKnowns and Unknownstansoei100% (1)
- Autoimmune Diseases and The Potential Role of Chinese Herbal MedicineDocument15 pagesAutoimmune Diseases and The Potential Role of Chinese Herbal Medicinetansoei100% (1)
- Yinyang HealingDocument27 pagesYinyang HealingtansoeiNo ratings yet
- The Physics of ProductivityDocument9 pagesThe Physics of ProductivitytansoeiNo ratings yet
- 25ntkkeyperformanceindicators 140729020920 Phpapp01Document40 pages25ntkkeyperformanceindicators 140729020920 Phpapp01mailsianNo ratings yet
- On Line Algorithms For High Frequency TradingDocument12 pagesOn Line Algorithms For High Frequency TradingtansoeiNo ratings yet
- Wirth Good Ideas Through The Looking GlassDocument28 pagesWirth Good Ideas Through The Looking GlasstansoeiNo ratings yet
- Orloff Intuitive HealingDocument21 pagesOrloff Intuitive Healingtansoei100% (6)
- Beautifulsoup: Web Scraping With Python: Andrew PetersonDocument43 pagesBeautifulsoup: Web Scraping With Python: Andrew PetersontansoeiNo ratings yet
- The 4 Most Effective Ways Leaders Solve Problems - Forbes PDFDocument4 pagesThe 4 Most Effective Ways Leaders Solve Problems - Forbes PDFtansoeiNo ratings yet
- Netflix CultureDocument128 pagesNetflix CulturetansoeiNo ratings yet
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- ACI Remote Leaf Fabric Discovery v1.0 PDFDocument24 pagesACI Remote Leaf Fabric Discovery v1.0 PDFdelplayNo ratings yet
- Year 8 Fractions and PercentagesDocument20 pagesYear 8 Fractions and PercentagessanduedNo ratings yet
- How To Import Satellite Image From Google Earth To ArcGISDocument10 pagesHow To Import Satellite Image From Google Earth To ArcGISMehmood AlamNo ratings yet
- Mahindra Max 28items CSD PerDocument1 pageMahindra Max 28items CSD Perboobalan_shriNo ratings yet
- Dzone Refcard 347 Oauth Patterns Anti Patterns 202Document6 pagesDzone Refcard 347 Oauth Patterns Anti Patterns 202Brosoa LoquaNo ratings yet
- Decision Tree and TableDocument18 pagesDecision Tree and TablekamarulzamaniNo ratings yet
- TS 52PRO: Test SetDocument28 pagesTS 52PRO: Test SetOscar ChavesNo ratings yet
- KBC GameDocument27 pagesKBC GamerishabhNo ratings yet
- Important Notice: Kind RegardsDocument15 pagesImportant Notice: Kind RegardsLeonard GržetićNo ratings yet
- Maithili AmbavaneDocument62 pagesMaithili Ambavanerushikesh2096No ratings yet
- P4 (MGPS) - Multiplication, Division, and Word ProblemsDocument4 pagesP4 (MGPS) - Multiplication, Division, and Word ProblemsolgaNo ratings yet
- Annexure To SOW 10 Standard Specification For Steam TracingDocument9 pagesAnnexure To SOW 10 Standard Specification For Steam TracingASHISH GORDENo ratings yet
- GA and ANNDocument17 pagesGA and ANNini benNo ratings yet
- Variable Voltaje AlternadorDocument37 pagesVariable Voltaje AlternadorFrank Araya DiazNo ratings yet
- Index: S.No Program List Page NoDocument26 pagesIndex: S.No Program List Page NoVinay PadhiyarNo ratings yet
- Juniper Netscreen ISG Series DatasheetDocument12 pagesJuniper Netscreen ISG Series Datasheetbh.youssefNo ratings yet
- Syllabus Electrical Machines Subject Code: Ele-405 L T P: 2 1 0 Credits: 03Document3 pagesSyllabus Electrical Machines Subject Code: Ele-405 L T P: 2 1 0 Credits: 03Nitin PalNo ratings yet
- Ga-H61m-Ds2 Hdmi - R10Document31 pagesGa-H61m-Ds2 Hdmi - R10Emerson SilvaNo ratings yet
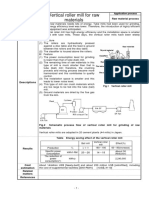
- Vertical Roller Mill For Raw MaterialsDocument1 pageVertical Roller Mill For Raw Materialsअहा मधुमक्खीपालनNo ratings yet
- Luna2000-5-S0 Cert N8aDocument1 pageLuna2000-5-S0 Cert N8acatalinnnspinuuuNo ratings yet
- Library Copy Merge ProcedureDocument6 pagesLibrary Copy Merge ProcedurecarloNo ratings yet
- RD400PXL-2 Precision Locator Technical Specification: Description Part NoDocument2 pagesRD400PXL-2 Precision Locator Technical Specification: Description Part NoJosé Luis Bastidas RosasNo ratings yet
- Topic Wise Bundle PDF Course 2022 - Quantitative Aptitude Ages Set-1Document5 pagesTopic Wise Bundle PDF Course 2022 - Quantitative Aptitude Ages Set-1bala15876No ratings yet
- Rashid Jamal's Resume: Full NameDocument3 pagesRashid Jamal's Resume: Full Namerasheed17No ratings yet
- Zinc Coating, Hot-Dip, Requirements For Application To Carbon and Alloy Steel Bolts, Screws, Washers, Nuts, and Special Threaded Fasteners (Metric)Document5 pagesZinc Coating, Hot-Dip, Requirements For Application To Carbon and Alloy Steel Bolts, Screws, Washers, Nuts, and Special Threaded Fasteners (Metric)DeepakRajurkarNo ratings yet
- 1.0 ESC 21 - ENGG MGT PRESENTATION-What Is Eng. Mgt. - Rev 0 Aug 12 2021Document14 pages1.0 ESC 21 - ENGG MGT PRESENTATION-What Is Eng. Mgt. - Rev 0 Aug 12 2021Feolo Riel TarayNo ratings yet
- How To Go Viral With A Tiktok Creator ArmyDocument3 pagesHow To Go Viral With A Tiktok Creator Armymarkus karcusNo ratings yet
- SQL - 02Document21 pagesSQL - 02Arun JithNo ratings yet
- Omnichannel Playbook 2021Document48 pagesOmnichannel Playbook 2021Giao lưu Phó nháy và Mẫu (GLPVNM)No ratings yet
- Basic Operations On MAP: ExampleDocument9 pagesBasic Operations On MAP: ExampleSamara SequeiraNo ratings yet