You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Project 4 Ethylene OxideDocument12 pagesProject 4 Ethylene OxideNhan Nguyen Van100% (4)
- Typewriter Olivetti Linea98 SerManDocument66 pagesTypewriter Olivetti Linea98 SerManmplennaNo ratings yet
- Operator Manual BT4500-00ING PDFDocument153 pagesOperator Manual BT4500-00ING PDFquanvh0% (1)
- Oscilador Baud Rate para 90HzDocument1 pageOscilador Baud Rate para 90HzmplennaNo ratings yet
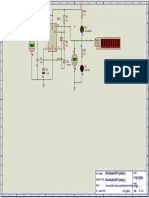
- LongWave TransmitterDocument1 pageLongWave TransmittermplennaNo ratings yet
- Ampl 15 WDocument1 pageAmpl 15 WmplennaNo ratings yet
- PW 1979 02Document93 pagesPW 1979 02mplennaNo ratings yet
- Rider-Resonance and Alignment - John F. RiderDocument95 pagesRider-Resonance and Alignment - John F. RidermplennaNo ratings yet
- Radio Craft 33 Amplifier Builder's GuideDocument68 pagesRadio Craft 33 Amplifier Builder's GuidemplennaNo ratings yet
- KA2297 DatasheetDocument6 pagesKA2297 DatasheetmplennaNo ratings yet
- 5.3W 2-Channel AF Power Amplifier: Package Dimensions FeaturesDocument12 pages5.3W 2-Channel AF Power Amplifier: Package Dimensions FeaturesmplennaNo ratings yet
- Radio TV Experimenter 1965-02-03Document132 pagesRadio TV Experimenter 1965-02-03mplennaNo ratings yet
- Babani 58 50 Circuits Using 7400 ICsDocument82 pagesBabani 58 50 Circuits Using 7400 ICsmplennaNo ratings yet
- Si861x/2x Data Sheet: Low-Power Single and Dual-Channel Digital IsolatorsDocument39 pagesSi861x/2x Data Sheet: Low-Power Single and Dual-Channel Digital IsolatorsmplennaNo ratings yet
- S I 4 8 2 2 / 2 6 / 2 7 / 4 0 / 4 4 A, S, L, D G: Ntenna Chematic Ayout AND Esign UidelinesDocument38 pagesS I 4 8 2 2 / 2 6 / 2 7 / 4 0 / 4 4 A, S, L, D G: Ntenna Chematic Ayout AND Esign UidelinesmplennaNo ratings yet
- CD4020BC - CD4040BC - CD4060BC 14-Stage Ripple Carry Binary Counters - 12-Stage Ripple Carry Binary Counters - 14-Stage Ripple Carry Binary CountersDocument8 pagesCD4020BC - CD4040BC - CD4060BC 14-Stage Ripple Carry Binary Counters - 12-Stage Ripple Carry Binary Counters - 14-Stage Ripple Carry Binary CountersmplennaNo ratings yet
- Role of Vitamins D, E and C in Immunity and in AmmationDocument6 pagesRole of Vitamins D, E and C in Immunity and in AmmationmplennaNo ratings yet
- G DFE G DFE: Main Functions Good SourcesDocument1 pageG DFE G DFE: Main Functions Good SourcesmplennaNo ratings yet
- Typewriter-Facit 1832 1831 1830 1828Document69 pagesTypewriter-Facit 1832 1831 1830 1828mplennaNo ratings yet
- TS-120V Instruction ManualDocument27 pagesTS-120V Instruction ManualmplennaNo ratings yet
- Tea 5711Document28 pagesTea 5711mplennaNo ratings yet
- YAESU FT 2000 Service ManualDocument206 pagesYAESU FT 2000 Service ManualmplennaNo ratings yet
- Data Sheet: TEA5591ADocument14 pagesData Sheet: TEA5591AmplennaNo ratings yet
- TBA570Document14 pagesTBA570mplennaNo ratings yet
- Tea 5710Document19 pagesTea 5710mplennaNo ratings yet
- FM/AM Tuner of Electronic Tuning Type: FunctionsDocument16 pagesFM/AM Tuner of Electronic Tuning Type: FunctionsmplennaNo ratings yet
- TA2003Document7 pagesTA2003mplennaNo ratings yet
- Tea 5551Document17 pagesTea 5551mplennaNo ratings yet
- Sum11 Pharma PDFDocument29 pagesSum11 Pharma PDFMostofa RubalNo ratings yet
- ESAB Welding & Cu Ing Products: A515 516 4 In. Thick 2 In. Root GapDocument1 pageESAB Welding & Cu Ing Products: A515 516 4 In. Thick 2 In. Root Gapalok987No ratings yet
- BR Int LD Id Inspiration 55-70plusDocument11 pagesBR Int LD Id Inspiration 55-70plustarkett tNo ratings yet
- AsdDocument3 pagesAsdMuStafaAbbasNo ratings yet
- ChE461-Course Outline and Teaching ScheduleDocument2 pagesChE461-Course Outline and Teaching ScheduleAl JawadNo ratings yet
- A Review On Natural Coagulants in Wastewater TreatmentDocument13 pagesA Review On Natural Coagulants in Wastewater Treatmentahsanur shuvoNo ratings yet
- Chemistry March 2008 EngDocument7 pagesChemistry March 2008 EngPrasad C M0% (2)
- Review of Related LiteratureDocument7 pagesReview of Related LiteratureJamie HaravataNo ratings yet
- Dyestone Blue MX SDS SA-0186-01Document5 pagesDyestone Blue MX SDS SA-0186-01gede aris prayoga mahardikaNo ratings yet
- Shades Eq Gloss Large Shade ChartDocument2 pagesShades Eq Gloss Large Shade ChartmeganNo ratings yet
- Carnauba-Super-Micropowder 2442 P 5: ApplicationDocument1 pageCarnauba-Super-Micropowder 2442 P 5: Application333cubi333No ratings yet
- Nta Abhyas Test-65 CDocument5 pagesNta Abhyas Test-65 CMIITY EDUNo ratings yet
- TIAC TechnologyDocument13 pagesTIAC TechnologyPaul SunnyNo ratings yet
- Processing of Roselle (Hibiscus Sabdariffa) Calyces For Value AdditionDocument7 pagesProcessing of Roselle (Hibiscus Sabdariffa) Calyces For Value AdditionSujata Ghodke100% (1)
- M Pharm Sem IIDocument25 pagesM Pharm Sem IIBhaven PatelNo ratings yet
- UV Coating Flooring - Radtech 2003 - D. Bontinck M. IdacageDocument6 pagesUV Coating Flooring - Radtech 2003 - D. Bontinck M. IdacageJuan Antonio Tito Esp CalNo ratings yet
- Borehole ProblemsDocument10 pagesBorehole ProblemsMuh Andika Pratama WarisNo ratings yet
- Endothermic and Exothermic Reactions WorksheetDocument4 pagesEndothermic and Exothermic Reactions Worksheetabdulhakim100% (1)
- WEIGHTSDocument11 pagesWEIGHTSvpjagannaathNo ratings yet
- Folder GluingDocument3 pagesFolder GluingSyed Mujtaba Ali Bukhari100% (1)
- 2018 10 08 ICSG Factbook Copper 2018Document66 pages2018 10 08 ICSG Factbook Copper 2018treNo ratings yet
- Proposed OS&E Requirement - Measuring Ozone DosageDocument3 pagesProposed OS&E Requirement - Measuring Ozone DosageProteina QuitinaseNo ratings yet
- FRP CLADDING PresentationDocument33 pagesFRP CLADDING PresentationDeepakNo ratings yet
- Part 7 StoichiometryDocument59 pagesPart 7 Stoichiometryjasumin91No ratings yet
- Anti-Aromatase Activity of Phytochemicals in White Button Mushrooms (Agaricus Bisporus)Document10 pagesAnti-Aromatase Activity of Phytochemicals in White Button Mushrooms (Agaricus Bisporus)Nimra Naveed ShaikhNo ratings yet
- Dielectric Strength of Transformer OilDocument2 pagesDielectric Strength of Transformer OilAnil VarriNo ratings yet
- Galvaspan G450Document2 pagesGalvaspan G450khurshedlakhoNo ratings yet
- Cytech Products Data SheetsDocument71 pagesCytech Products Data Sheetslinga2014No ratings yet