You might also like
- Introduction in Histopathology 2012Document105 pagesIntroduction in Histopathology 2012GigiEnergieNo ratings yet
- Us Marine Corps - First Aid MCRP 3-02GDocument227 pagesUs Marine Corps - First Aid MCRP 3-02GJessica StephensNo ratings yet
- Postural CorrectionDocument234 pagesPostural Correctiondhikaprasetya11_1969100% (1)
- Self - Non Self Limfocite T Si B MHC - Procesare / Prezentare AntigeneDocument52 pagesSelf - Non Self Limfocite T Si B MHC - Procesare / Prezentare AntigeneGigiEnergieNo ratings yet
- Self - Non Self Limfocite T Si B MHC - Procesare / Prezentare AntigeneDocument52 pagesSelf - Non Self Limfocite T Si B MHC - Procesare / Prezentare AntigeneGigiEnergieNo ratings yet
- 4 Sistem Raspuns Imun 2011 PDFDocument63 pages4 Sistem Raspuns Imun 2011 PDFGigiEnergieNo ratings yet
- 7 Imunodeficiente 2011Document58 pages7 Imunodeficiente 2011GigiEnergieNo ratings yet
- 2 Ag Ac 2011 PDFDocument8 pages2 Ag Ac 2011 PDFGigiEnergieNo ratings yet
- Useful BFTDocument2 pagesUseful BFTGigiEnergieNo ratings yet
- PlanseDocument3 pagesPlanseGigiEnergieNo ratings yet
- Unit 1Document10 pagesUnit 1GigiEnergieNo ratings yet
- The Present Tense Simple I. Formation RulesDocument14 pagesThe Present Tense Simple I. Formation RulesGigiEnergieNo ratings yet
- 1.ech Hidro ElectroliticDocument64 pages1.ech Hidro ElectroliticAdriana VillarrealNo ratings yet
- 2 Ag Ac 2011 PDFDocument8 pages2 Ag Ac 2011 PDFGigiEnergieNo ratings yet
- Intermediate Language PracticeDocument138 pagesIntermediate Language Practicerd_titus55595% (21)
- Fluid Mechanics PDFDocument15 pagesFluid Mechanics PDFGigiEnergieNo ratings yet
- WWI Air Medical ServiceDocument672 pagesWWI Air Medical ServiceCAP History Library100% (1)
- Muscle Biophysics - From Molecules To Cells - D. RassieerDocument374 pagesMuscle Biophysics - From Molecules To Cells - D. RassieerGigiEnergieNo ratings yet
- US Army Medical Course MD0694-200 - Basic Food Inspection ProceduresDocument83 pagesUS Army Medical Course MD0694-200 - Basic Food Inspection ProceduresGeorgesNo ratings yet
- Food ContainersDocument67 pagesFood ContainersPlainNormalGuy2No ratings yet
- Speed and Agility Progression for Knee RehabDocument3 pagesSpeed and Agility Progression for Knee RehabGigiEnergieNo ratings yet
- ARMY Medical - Wound Care Ed.100 78 PagesDocument78 pagesARMY Medical - Wound Care Ed.100 78 PagesDonT_RNNo ratings yet
- The Precise Neurological ExamDocument12 pagesThe Precise Neurological ExamGigiEnergieNo ratings yet
- Buoyancy in Aquatic Therapy: How Water Eases RehabilitationDocument3 pagesBuoyancy in Aquatic Therapy: How Water Eases RehabilitationGigiEnergieNo ratings yet
- The Trauma Manual - A. Peitzman, Et Al., (Lippincott, 1998) WWDocument312 pagesThe Trauma Manual - A. Peitzman, Et Al., (Lippincott, 1998) WWGigiEnergieNo ratings yet
- Exercise in Motor Neuron DiseasesDocument3 pagesExercise in Motor Neuron DiseasesGigiEnergieNo ratings yet
- Multiple Sclerosis - National Clinical Guideline (Diagnosis and Management) (2004) WW PDFDocument213 pagesMultiple Sclerosis - National Clinical Guideline (Diagnosis and Management) (2004) WW PDFGigiEnergieNo ratings yet
- Dystonia - The Many FacetDocument230 pagesDystonia - The Many FacetGigiEnergie100% (1)
- Adolescent Problems - Guide For Teachers, Parents, CounsellorsDocument169 pagesAdolescent Problems - Guide For Teachers, Parents, CounsellorsAbdelmjid Fiamanilahh100% (2)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5784)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (72)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Kantrowitz 2019Document6 pagesKantrowitz 2019koli bogiNo ratings yet
- G10 Q1 Health Module 3Document11 pagesG10 Q1 Health Module 3Manuel Rosales Jr.No ratings yet
- Maizir 2019 IOP Conf. Ser. Mater. Sci. Eng. 615 012105Document9 pagesMaizir 2019 IOP Conf. Ser. Mater. Sci. Eng. 615 012105Green MyanmarNo ratings yet
- Robot Manual Safety GuideDocument45 pagesRobot Manual Safety GuideTrung Truc NguyenNo ratings yet
- BS en 13479-17Document48 pagesBS en 13479-17jeffer rojasNo ratings yet
- Exp 3 Free Vortex N Forced VortexDocument5 pagesExp 3 Free Vortex N Forced VortexAmrun RusrlNo ratings yet
- Tutorial Guide Open FoamDocument104 pagesTutorial Guide Open FoaminaNo ratings yet
- A Model For Cell Growth in Batch BioreactorsDocument128 pagesA Model For Cell Growth in Batch BioreactorsalabastrinoNo ratings yet
- Assignment 2-Case of Anna ODocument6 pagesAssignment 2-Case of Anna Otonnibravo75% (4)
- Lámina ParacetamolDocument2 pagesLámina ParacetamolAndrea Alvarado RoNo ratings yet
- Soal Semester Genap 2019 Kelas XII Bahasa InggrisDocument9 pagesSoal Semester Genap 2019 Kelas XII Bahasa InggrisWalid UmarNo ratings yet
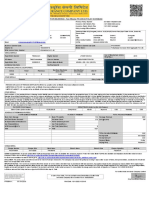
- Motor Insurance - Two Wheeler Package Policy ScheduleDocument1 pageMotor Insurance - Two Wheeler Package Policy SchedulePriya RNo ratings yet
- PE Basketball Rules SummaryDocument1 pagePE Basketball Rules SummaryKarlo RoseroNo ratings yet
- Diagram Al-Fe PDFDocument3 pagesDiagram Al-Fe PDFImeldaHiaNo ratings yet
- Anodize AluminiumDocument200 pagesAnodize AluminiumYunus LorrNo ratings yet
- Calculate Speed of Light, Radio & Microwave WavesDocument4 pagesCalculate Speed of Light, Radio & Microwave WavesNayeemAhmedNo ratings yet
- SATPREP Circular Measurement PracticeDocument5 pagesSATPREP Circular Measurement PracticeJoel SohNo ratings yet
- DowsingDocument76 pagesDowsingBacean Aurel IoanNo ratings yet
- Warman Mcu 350 Masbate Philippines Case Study DuplicateDocument2 pagesWarman Mcu 350 Masbate Philippines Case Study DuplicateBJ AbelaNo ratings yet
- Quiz No. 1Document3 pagesQuiz No. 1Keaven Rold FormilosNo ratings yet
- D1348Document6 pagesD1348Ненад КнежевићNo ratings yet
- EWD-H-KXJ3 Elevator Load Weighing GuideDocument10 pagesEWD-H-KXJ3 Elevator Load Weighing GuideKang RohendyNo ratings yet
- NPSM & NPSL - American Pipe Threads ChartDocument1 pageNPSM & NPSL - American Pipe Threads ChartAlvaro TreviñoNo ratings yet
- Causes and Symptoms of Vaginal Bleeding During PregnancyDocument28 pagesCauses and Symptoms of Vaginal Bleeding During PregnancyNurul AnnisaniNo ratings yet
- Company-Profile-word-final Kadakso AsiliDocument4 pagesCompany-Profile-word-final Kadakso AsiliHaron HB WritersNo ratings yet
- Class Timetable Summary for Periods 1-5Document14 pagesClass Timetable Summary for Periods 1-5عبدالرحمن فهمي الشريفNo ratings yet
- Home in Tacoma - Findings of Fact and Recommendation ReportDocument23 pagesHome in Tacoma - Findings of Fact and Recommendation ReportThe UrbanistNo ratings yet
- Toys of Early America ... You Can Make, by Reba Ann DunmireDocument84 pagesToys of Early America ... You Can Make, by Reba Ann DunmireJeff JeffersonNo ratings yet
- PEMERIKSAAN THORAX AND JANTUNGDocument59 pagesPEMERIKSAAN THORAX AND JANTUNGImada KhoironiNo ratings yet
- MSC Lecture06Document28 pagesMSC Lecture06Arpan GayenNo ratings yet