You might also like
- Food Fight: Carbs vs Fat for AthletesDocument28 pagesFood Fight: Carbs vs Fat for AthletesStephany ZamorasNo ratings yet
- Protein and Amino AcidsDocument43 pagesProtein and Amino AcidscloudoxyNo ratings yet
- 13 - Nutrition-Recovery-Carbohydrate-2Document13 pages13 - Nutrition-Recovery-Carbohydrate-2tran anhkhoaNo ratings yet
- Protein "Requirements" Beyond The RDA Implications For Optimizing HealthDocument8 pagesProtein "Requirements" Beyond The RDA Implications For Optimizing HealthTicinosthetics GainzSchoolNo ratings yet
- ProteinsDocument22 pagesProteinsAdilriazkhanachkzai AdilriazkhanachkzaiNo ratings yet
- Mac Nutrition 09Document63 pagesMac Nutrition 09Dhila FayaNo ratings yet
- Sports Health DisciplinesDocument15 pagesSports Health Disciplinesjade brionesNo ratings yet
- Symbiosis: Meal Frequency and Nutrient Distribution: What Is Ideal For Body Composition?Document4 pagesSymbiosis: Meal Frequency and Nutrient Distribution: What Is Ideal For Body Composition?WexZorNo ratings yet
- Energy Metabolism and NutritionDocument24 pagesEnergy Metabolism and NutritionVictoriaNo ratings yet
- A Proteína Dietética para Os Atletas - A Partir de Requisitos para A Adaptação Perfeita.Document8 pagesA Proteína Dietética para Os Atletas - A Partir de Requisitos para A Adaptação Perfeita.MarcosViníciusSilvaNo ratings yet
- Moderate CarbohydrateDocument9 pagesModerate CarbohydrateAndrea TorrealdayNo ratings yet
- Protein Update: How Much Protein is EnoughDocument3 pagesProtein Update: How Much Protein is EnoughManuel FerreiraNo ratings yet
- Biomedicine & Pharmacotherapy: A B C B B B BDocument8 pagesBiomedicine & Pharmacotherapy: A B C B B B BChronika RenamariaNo ratings yet
- Biomedicine & Pharmacotherapy: A B C B B B BDocument8 pagesBiomedicine & Pharmacotherapy: A B C B B B BChronika RenamariaNo ratings yet
- Biomedicine & Pharmacotherapy: A B C B B B BDocument8 pagesBiomedicine & Pharmacotherapy: A B C B B B BChronika RenamariaNo ratings yet
- Perioperative Pediatric Nutrition CareDocument51 pagesPerioperative Pediatric Nutrition CareAtria DewiNo ratings yet
- Protein Basic SlideshowDocument15 pagesProtein Basic Slideshowrichard eastNo ratings yet
- Optimal Protein Intake in The Elderly: Robert R. Wolfe, Sharon L. Miller, Kevin B. MillerDocument10 pagesOptimal Protein Intake in The Elderly: Robert R. Wolfe, Sharon L. Miller, Kevin B. MillerRoberto CasilloNo ratings yet
- Popular Weight Loss Diet PresentationDocument97 pagesPopular Weight Loss Diet PresentationRadwan AjoNo ratings yet
- Disease and Nutrition Research 5pgDocument9 pagesDisease and Nutrition Research 5pgthuo.harrison31No ratings yet
- Nutrition in CKD: DR Neeraj Nirala DNB NephrologyDocument50 pagesNutrition in CKD: DR Neeraj Nirala DNB NephrologyMOHIT NAREDI100% (2)
- Nutrition For Health and FitnessDocument36 pagesNutrition For Health and FitnessFaatoots FatsNo ratings yet
- LIFESCI 2N03: Human: Nutrition For Life ScienceDocument40 pagesLIFESCI 2N03: Human: Nutrition For Life ScienceAnnalisa NguyenNo ratings yet
- Sportska Ishrana - Doping U Sportu: Doc Dr. Brizita DjordjevicDocument61 pagesSportska Ishrana - Doping U Sportu: Doc Dr. Brizita DjordjevicAleksandar Sale JulovskiNo ratings yet
- Clarck Necessidades ProteicasDocument4 pagesClarck Necessidades ProteicasCássio ShividerskiNo ratings yet
- Sport Nutrition PowerpointDocument91 pagesSport Nutrition Powerpointapi-234854471No ratings yet
- Aarr - May .2012-.Document15 pagesAarr - May .2012-.Γιωργος ΒλαχοςNo ratings yet
- HTTP WWW - CoachesontarioDocument3 pagesHTTP WWW - CoachesontariomwoodspgNo ratings yet
- 2010 - Increased Protein Intake Reduces Lean Body Mass Loss During Weight Loss in AthletesDocument12 pages2010 - Increased Protein Intake Reduces Lean Body Mass Loss During Weight Loss in AthletescaiovcoNo ratings yet
- Glycemic Index and RecoveryDocument3 pagesGlycemic Index and Recoverymarin0410No ratings yet
- Lecture 8 - Ergogenic-AidsDocument43 pagesLecture 8 - Ergogenic-AidsMuhd AnasNo ratings yet
- Biomedicine & Pharmacotherapy: A B C B B B BDocument8 pagesBiomedicine & Pharmacotherapy: A B C B B B BprayogarathaNo ratings yet
- 7 Roleofmacronutrient2017Document9 pages7 Roleofmacronutrient2017LusianiNo ratings yet
- A Word of Caution Against Excessive Protein Intake (Mittendorfer, Klein y Fontana, 2019) PDFDocument8 pagesA Word of Caution Against Excessive Protein Intake (Mittendorfer, Klein y Fontana, 2019) PDFLucas CalleriNo ratings yet
- Effects of Daily 24 Gram Doses of Rice or Whey Protein On ResistanceDocument15 pagesEffects of Daily 24 Gram Doses of Rice or Whey Protein On ResistanceThiago BritoNo ratings yet
- Nutritional Management for Patients with Chronic Kidney DiseaseDocument41 pagesNutritional Management for Patients with Chronic Kidney DiseaseZaza ZunitaNo ratings yet
- 2021-06-01 EatingWell The Power of ProteinDocument100 pages2021-06-01 EatingWell The Power of Proteinniki399yNo ratings yet
- 8.minerals, Nutrition and MalnutritionDocument50 pages8.minerals, Nutrition and MalnutritionSantino MajokNo ratings yet
- Chapter 9-10. StudentDocument15 pagesChapter 9-10. StudentPrince Al AbidNo ratings yet
- Publikasi Ilmiah TR90Document9 pagesPublikasi Ilmiah TR90nelymasrurohNo ratings yet
- Nutrition & Metabolism: Dietary Guidelines Should Reflect New Understandings About AdultDocument6 pagesNutrition & Metabolism: Dietary Guidelines Should Reflect New Understandings About AdultNurfadhilahNo ratings yet
- Cancercleansequickstartguide 2018 PDFDocument13 pagesCancercleansequickstartguide 2018 PDFVinciane Baudoux100% (1)
- Nutrition in Surgical Patients PDFDocument2 pagesNutrition in Surgical Patients PDFJohn Christopher Luces100% (1)
- They Help in CholesterolDocument82 pagesThey Help in CholesterolEileen del RosarioNo ratings yet
- Basic Nutrition PDFDocument58 pagesBasic Nutrition PDFphinoetNo ratings yet
- Dr. Andrea Braakhuis-Performance Nutrition For Track & FieldDocument6 pagesDr. Andrea Braakhuis-Performance Nutrition For Track & FieldChris NickinsonNo ratings yet
- Final Case Study PresentationDocument49 pagesFinal Case Study Presentationapi-505518832No ratings yet
- Sport Physiology4 Komposisi KarboDocument27 pagesSport Physiology4 Komposisi Karbolala liliNo ratings yet
- Food Pattern PugsDocument32 pagesFood Pattern PugsAsh RoryNo ratings yet
- 23 DieteticsDocument71 pages23 DieteticsJai CarungayNo ratings yet
- Practical Approach To Determining Protein Requirements of The Critically Ill 2023 - 0107 JBO NHS DefDocument50 pagesPractical Approach To Determining Protein Requirements of The Critically Ill 2023 - 0107 JBO NHS DefMateo LondoñoNo ratings yet
- JCSM 12 2022Document12 pagesJCSM 12 2022Henrique OtavioNo ratings yet
- DR B SesikeranDocument30 pagesDR B SesikerandranandrtNo ratings yet
- 6 - June - 2008Document16 pages6 - June - 2008Warhammer13No ratings yet
- Research Digest: Exclusive Sneak PeekDocument11 pagesResearch Digest: Exclusive Sneak PeekIvan PitrulliNo ratings yet
- Balanced Food Whey Chocolate Clinical ApplicationsDocument2 pagesBalanced Food Whey Chocolate Clinical Applicationsapi-285232606No ratings yet
- Physiology of Metabolism and EnergyDocument44 pagesPhysiology of Metabolism and EnergyShilvia JungNo ratings yet
- Protein CalculatorDocument1 pageProtein CalculatorJoul BitarNo ratings yet
- High Protein & Low Carb Diet Women - Lose Weight Quickly and Much - Men - Increase Muscle Mass and Become Very Strong -: COOKBOOK, #3From EverandHigh Protein & Low Carb Diet Women - Lose Weight Quickly and Much - Men - Increase Muscle Mass and Become Very Strong -: COOKBOOK, #3No ratings yet
- Keeping Your Memory & Focus Sharp: How Your Diet & Nutrition Affect Cognition, Memory & FocusDocument20 pagesKeeping Your Memory & Focus Sharp: How Your Diet & Nutrition Affect Cognition, Memory & FocusBeneVia by HealthSpan InstituteNo ratings yet
- Going Gluten Free: Celiac Disease & Getting High Quality Protein Into Your DietDocument18 pagesGoing Gluten Free: Celiac Disease & Getting High Quality Protein Into Your DietBeneVia by HealthSpan InstituteNo ratings yet
- Protein Energy Is The Most Important Nutrient in Aging & PerformanceDocument11 pagesProtein Energy Is The Most Important Nutrient in Aging & PerformanceBeneVia by HealthSpan InstituteNo ratings yet
- The Heart of The Matter: Heart Health & DiabetesDocument18 pagesThe Heart of The Matter: Heart Health & DiabetesBeneVia by HealthSpan InstituteNo ratings yet
- Why Active Snacking Is The Most Effective Method of Nutritional SupplementationDocument15 pagesWhy Active Snacking Is The Most Effective Method of Nutritional SupplementationBeneVia by HealthSpan InstituteNo ratings yet
- UNIMED Past Questions-1Document6 pagesUNIMED Past Questions-1snazzyNo ratings yet
- Oilwell Fishing Operations Tools and TechniquesDocument126 pagesOilwell Fishing Operations Tools and Techniqueskevin100% (2)
- Thecodeblocks Com Acl in Nodejs ExplainedDocument1 pageThecodeblocks Com Acl in Nodejs ExplainedHamza JaveedNo ratings yet
- Critical Growth StagesDocument3 pagesCritical Growth StagesSunil DhankharNo ratings yet
- ICU Lines TubesDocument7 pagesICU Lines TubesCindy MurphyNo ratings yet
- Healthy Kitchen Shortcuts: Printable PackDocument12 pagesHealthy Kitchen Shortcuts: Printable PackAndre3893No ratings yet
- ICE Learned Event DubaiDocument32 pagesICE Learned Event DubaiengkjNo ratings yet
- Business Data Communications and Networking 13Th Edition Fitzgerald Test Bank Full Chapter PDFDocument40 pagesBusiness Data Communications and Networking 13Th Edition Fitzgerald Test Bank Full Chapter PDFthrongweightypfr100% (12)
- Amazfit Bip 5 Manual enDocument30 pagesAmazfit Bip 5 Manual enJohn WalesNo ratings yet
- 14 Worst Breakfast FoodsDocument31 pages14 Worst Breakfast Foodscora4eva5699100% (1)
- CVA: Health Education PlanDocument4 pagesCVA: Health Education Plandanluki100% (3)
- The Hittite Name For GarlicDocument5 pagesThe Hittite Name For GarlictarnawtNo ratings yet
- Coasts Case Studies PDFDocument13 pagesCoasts Case Studies PDFMelanie HarveyNo ratings yet
- How To Make Wall Moulding Design For Rooms Accent Wall Video TutorialsDocument15 pagesHow To Make Wall Moulding Design For Rooms Accent Wall Video Tutorialsdonaldwhale1151No ratings yet
- Writing Assessment and Evaluation Checklist - PeerDocument1 pageWriting Assessment and Evaluation Checklist - PeerMarlyn Joy YaconNo ratings yet
- Ds 1Document8 pagesDs 1michaelcoNo ratings yet
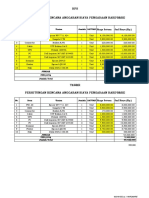
- HPS Perhitungan Rencana Anggaran Biaya Pengadaan Hardware: No. Item Uraian Jumlah SATUANDocument2 pagesHPS Perhitungan Rencana Anggaran Biaya Pengadaan Hardware: No. Item Uraian Jumlah SATUANYanto AstriNo ratings yet
- USP 11 ArgumentArraysDocument52 pagesUSP 11 ArgumentArraysKanha NayakNo ratings yet
- Chapter 15-Writing3 (Thesis Sentence)Document7 pagesChapter 15-Writing3 (Thesis Sentence)Dehan Rakka GusthiraNo ratings yet
- Sky Education: Organisation of Commerce and ManagementDocument12 pagesSky Education: Organisation of Commerce and ManagementKiyaara RathoreNo ratings yet
- 4TH Quarter English 10 Assessment TestDocument6 pages4TH Quarter English 10 Assessment TestafbnjkcdNo ratings yet
- Marylebone Construction UpdateDocument2 pagesMarylebone Construction UpdatePedro SousaNo ratings yet
- FE 405 Ps 3 AnsDocument12 pagesFE 405 Ps 3 Anskannanv93No ratings yet
- Infinitive Clauses PDFDocument3 pagesInfinitive Clauses PDFKatia LeliakhNo ratings yet
- (Section-A / Aip) : Delhi Public School GandhinagarDocument2 pages(Section-A / Aip) : Delhi Public School GandhinagarVvs SadanNo ratings yet
- Eurythmy: OriginDocument4 pagesEurythmy: OriginDananjaya PranandityaNo ratings yet
- Design Thinking SyllabusDocument6 pagesDesign Thinking Syllabussarbast piroNo ratings yet
- Motorizovaná Pechota RotaDocument12 pagesMotorizovaná Pechota RotaFran BejaranoNo ratings yet
- Organizational CultureDocument76 pagesOrganizational Culturenaty fishNo ratings yet
- Unit 6 Lesson 3 Congruent Vs SimilarDocument7 pagesUnit 6 Lesson 3 Congruent Vs Similar012 Ni Putu Devi AgustinaNo ratings yet