You might also like
- Role of Interleukins in Inflammation and DiseaseDocument9 pagesRole of Interleukins in Inflammation and DiseaseDavood HassanNo ratings yet
- Role of Cytokines As Inflammatory Mediators, EndocrineDocument34 pagesRole of Cytokines As Inflammatory Mediators, EndocrineRajarshi KumarNo ratings yet
- Unit 6 CytokinesDocument29 pagesUnit 6 CytokinesamirahaliNo ratings yet
- Inflammation and Inflammatory MediatorsDocument40 pagesInflammation and Inflammatory MediatorsQuty Papa KannaNo ratings yet
- Practice School Report On Interleukins Submitted by Davood AhmadDocument21 pagesPractice School Report On Interleukins Submitted by Davood AhmadDavood HassanNo ratings yet
- Cellular and Molecular Immunology 9th Edition Abbas Test BankDocument4 pagesCellular and Molecular Immunology 9th Edition Abbas Test Bankdrkevinlee03071984jki100% (28)
- (MID) IMMUNOSERO - Chapter 13 - Hypersensitivity (Reviewer)Document6 pages(MID) IMMUNOSERO - Chapter 13 - Hypersensitivity (Reviewer)Aisle Malibiran PalerNo ratings yet
- Cytokines in The Innate Immune ResponseDocument3 pagesCytokines in The Innate Immune ResponseNicole Tan100% (1)
- Cytokines N ChemokionesDocument31 pagesCytokines N ChemokionesMd. Ahsan-Ul BariNo ratings yet
- Ishaque PK Pondicherry UniversityDocument34 pagesIshaque PK Pondicherry UniversityRiska Resty WasitaNo ratings yet
- CytokinesDocument3 pagesCytokinesMohanad JawadNo ratings yet
- Cytokines & Their ActionsDocument59 pagesCytokines & Their ActionsSharanabasappa DurgNo ratings yet
- Citocinas e AsmaDocument14 pagesCitocinas e AsmaFabiula AbreuNo ratings yet
- Mediators of Inflammation and Immune Reaction - 1 Bradykinin, Nitric Oxide, Neuropeptides and Cytokines Saitoti S.S.MDocument30 pagesMediators of Inflammation and Immune Reaction - 1 Bradykinin, Nitric Oxide, Neuropeptides and Cytokines Saitoti S.S.MMusa yohanaNo ratings yet
- CytokinesDocument70 pagesCytokinesyudith novidaNo ratings yet
- Biotech Pharmaceuticals Cytokines: Cytokines Are Not The Same As HormonesDocument23 pagesBiotech Pharmaceuticals Cytokines: Cytokines Are Not The Same As HormonesSujan BoseNo ratings yet
- Activation of T Lymphocytes: Hypersensitivity Referring To Tissue Damage Caused by An ImmuneDocument8 pagesActivation of T Lymphocytes: Hypersensitivity Referring To Tissue Damage Caused by An ImmuneJorge SalinasNo ratings yet
- Topic: Cytokine and Their Roles in The Immune Regulation: Md. Jiyaul MustafaDocument21 pagesTopic: Cytokine and Their Roles in The Immune Regulation: Md. Jiyaul MustafaAisha Siddiq100% (1)
- Up To Date. Pathogenesis of Allergic RhinitisDocument16 pagesUp To Date. Pathogenesis of Allergic RhinitisGuardito PequeñoNo ratings yet
- Cytokine Roles and Functions in the Immune SystemDocument53 pagesCytokine Roles and Functions in the Immune SystemBima Ewando KabanNo ratings yet
- Asthma Pathophysiology TheraDocument3 pagesAsthma Pathophysiology TheraJayde TabanaoNo ratings yet
- E Lenkov 2002Document14 pagesE Lenkov 2002Matheus Tavares MartinsNo ratings yet
- Shock: A Review of Pathophysiology and Management. Part II: L. I. G. WorthleyDocument19 pagesShock: A Review of Pathophysiology and Management. Part II: L. I. G. Worthleynutnut_chanNo ratings yet
- 2006 SOM 208 Microbiology Syllabus Septic ShockDocument4 pages2006 SOM 208 Microbiology Syllabus Septic ShockDragan YottNo ratings yet
- Cytokines 2Document29 pagesCytokines 2Essington BeloNo ratings yet
- CYTOKINESDocument31 pagesCYTOKINESSaifi Alam100% (4)
- Systemic Lupus ErythemathosusDocument23 pagesSystemic Lupus ErythemathosusFransisca HardimartaNo ratings yet
- Citocinas ReviewDocument91 pagesCitocinas ReviewHugo SantanaNo ratings yet
- CH 7 Antibody 7E16Document1 pageCH 7 Antibody 7E16JUSASBNo ratings yet
- Anti InflammatorydrugsmodifiedsummaryDocument96 pagesAnti Inflammatorydrugsmodifiedsummary_RedX_No ratings yet
- To Study The Role of T-Regulatory Cells in The Infectious and Non-Infectious UveitisDocument30 pagesTo Study The Role of T-Regulatory Cells in The Infectious and Non-Infectious UveitisRavi SharmaNo ratings yet
- Cytokines: An Overview of Their Classification, Functions and Role in Rheumatoid ArthritisDocument39 pagesCytokines: An Overview of Their Classification, Functions and Role in Rheumatoid ArthritisRiska Resty WasitaNo ratings yet
- Basic Immunology of Allergic Disease: Tutik Ida Rosanti Laboratorium ParasitologiDocument17 pagesBasic Immunology of Allergic Disease: Tutik Ida Rosanti Laboratorium ParasitologiFiqrotul UmamNo ratings yet
- USMLE Step 1 NotesDocument5 pagesUSMLE Step 1 NotesvillarexNo ratings yet
- Type 1 HypersensitivityDocument38 pagesType 1 Hypersensitivitychocoholic potchiNo ratings yet
- Interleukin-33 in Asthma How Big of A Role Does It PlayDocument8 pagesInterleukin-33 in Asthma How Big of A Role Does It PlayFabiula AbreuNo ratings yet
- Cytokine Dysregulation, Infl Ammation and Well-Being: ReviewDocument15 pagesCytokine Dysregulation, Infl Ammation and Well-Being: Reviewcindyramadhanputri_4No ratings yet
- Cytokines and Thelper Subsets: MCB 150, PR CoscoyDocument42 pagesCytokines and Thelper Subsets: MCB 150, PR CoscoyMac Kevin MandapNo ratings yet
- Chapter 11:: Cytokines:: Ifor R. Williams & Thomas S. KupperDocument26 pagesChapter 11:: Cytokines:: Ifor R. Williams & Thomas S. KupperSartika Ayu NingsihNo ratings yet
- Cytokines in Acute and Chronic Inflammation: Carol A. Feghali, PH.D., and Timothy M. Wright, M.DDocument17 pagesCytokines in Acute and Chronic Inflammation: Carol A. Feghali, PH.D., and Timothy M. Wright, M.DWahyu Tri KusprasetyoNo ratings yet
- Cytokine functions and properties in immune response regulationDocument5 pagesCytokine functions and properties in immune response regulationMuneer AljamaanNo ratings yet
- Psoriasis Treatment by AnogenDocument27 pagesPsoriasis Treatment by AnogenAnogenNo ratings yet
- Perspectives: Diversification of T-Helper-Cell Lineages: Finding The Family Root of IL-17-producing CellsDocument5 pagesPerspectives: Diversification of T-Helper-Cell Lineages: Finding The Family Root of IL-17-producing CellsIván DiazNo ratings yet
- SirsDocument49 pagesSirsJesca MgegelaNo ratings yet
- Cytokines: General Properties and Role in Innate and Adaptive ImmunityDocument50 pagesCytokines: General Properties and Role in Innate and Adaptive ImmunityKhalil KhusairiNo ratings yet
- Ishaque PK Pondicherry UniversityDocument34 pagesIshaque PK Pondicherry UniversityharishchaudhariNo ratings yet
- Innate Immunity 3 (50 Q)Document5 pagesInnate Immunity 3 (50 Q)evelynseaaNo ratings yet
- AsthmaDocument100 pagesAsthmaMohamed HefnyNo ratings yet
- Suspected Article Mos 2009 JMA XII 1Document6 pagesSuspected Article Mos 2009 JMA XII 1Oana CraciunNo ratings yet
- Cytokine Functions and Receptor FamiliesDocument6 pagesCytokine Functions and Receptor FamiliesNur LiyanaNo ratings yet
- CytokineDocument7 pagesCytokineMaryam ShahrasbiNo ratings yet
- Table 10-1. Major Properties of Human Interleukins. Interleukin Principal Cell Source Principal EffectsDocument8 pagesTable 10-1. Major Properties of Human Interleukins. Interleukin Principal Cell Source Principal EffectsKhrisnanto NugrohoNo ratings yet
- aaaaa2Document11 pagesaaaaa2Nejc KovačNo ratings yet
- Innate and Adaptive Immunity: - Innate Is FIRST LINE OF DEFENCE: No Prior Exposure Needed - Comprised OfDocument31 pagesInnate and Adaptive Immunity: - Innate Is FIRST LINE OF DEFENCE: No Prior Exposure Needed - Comprised OfBegumHazinNo ratings yet
- Inflammation Lecture 3 Chemical Mediators and Regulators of IflammationDocument30 pagesInflammation Lecture 3 Chemical Mediators and Regulators of Iflammationtareqhaddad123No ratings yet
- Chemical Mediators of Acute Inflammation - HandoutDocument24 pagesChemical Mediators of Acute Inflammation - HandoutRawa MuhsinNo ratings yet
- Advances in treating allergic diseases and asthma through immunological approachesDocument17 pagesAdvances in treating allergic diseases and asthma through immunological approachesSam SonNo ratings yet
- Theroleofnasal Corticosteroidsinthe Treatmentofrhinitis: Eli O. MeltzerDocument16 pagesTheroleofnasal Corticosteroidsinthe Treatmentofrhinitis: Eli O. MeltzerJohn SmithNo ratings yet
- Co-signal Molecules in T Cell Activation: Immune Regulation in Health and DiseaseFrom EverandCo-signal Molecules in T Cell Activation: Immune Regulation in Health and DiseaseMiyuki AzumaNo ratings yet
- Platelets and Aspirin-Induced Asthma: Pathogenesis and MelatoninFrom EverandPlatelets and Aspirin-Induced Asthma: Pathogenesis and MelatoninNo ratings yet
- BivvkhDocument1 pageBivvkhDhila SafirinaNo ratings yet
- KMDNCKWDocument1 pageKMDNCKWDhila SafirinaNo ratings yet
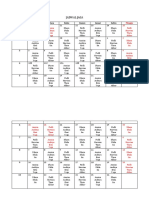
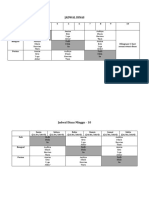
- Jadwal Jaga: Minggu Senin Selasa Rabu Kamis Jumat Sabtu 1Document2 pagesJadwal Jaga: Minggu Senin Selasa Rabu Kamis Jumat Sabtu 1Dhila SafirinaNo ratings yet
- WVRTBDocument2 pagesWVRTBDhila SafirinaNo ratings yet
- GJRDDocument1 pageGJRDDhila SafirinaNo ratings yet
- Duty Report Highlights Doctor and Patient DetailsDocument25 pagesDuty Report Highlights Doctor and Patient DetailsAuditya WidyasariNo ratings yet
- JngoeodDocument1 pageJngoeodDhila SafirinaNo ratings yet
- Jadwal Jaga: Minggu Senin Selasa Rabu Kamis Jumat Sabtu 1Document2 pagesJadwal Jaga: Minggu Senin Selasa Rabu Kamis Jumat Sabtu 1Dhila SafirinaNo ratings yet
- PPTDocument32 pagesPPTDhila SafirinaNo ratings yet
- BFGDocument1 pageBFGDhila SafirinaNo ratings yet
- DUTY REPORT PATIENT ASSESSMENTDocument18 pagesDUTY REPORT PATIENT ASSESSMENTDhila SafirinaNo ratings yet
- Duty Report: Co-Assistant On Duty: Fadhila Ayu Safirina Succi Islami PDocument23 pagesDuty Report: Co-Assistant On Duty: Fadhila Ayu Safirina Succi Islami PDhila SafirinaNo ratings yet
- Pathophysiology: RoductionDocument6 pagesPathophysiology: RoductionDhila SafirinaNo ratings yet
- Duty Report: Co-Assistant On Duty: Fadhila Ayu Safirina Succi Islami PutriDocument29 pagesDuty Report: Co-Assistant On Duty: Fadhila Ayu Safirina Succi Islami PutriDhila SafirinaNo ratings yet
- Duty Report: Co-Assistant On Duty: Fadhila Ayu Safirina Succi Islami PutriDocument29 pagesDuty Report: Co-Assistant On Duty: Fadhila Ayu Safirina Succi Islami PutriDhila SafirinaNo ratings yet
- DUTY REPORT PATIENT ASSESSMENTDocument18 pagesDUTY REPORT PATIENT ASSESSMENTDhila SafirinaNo ratings yet
- N O Name AGE SEX Vitamin D Lab Result DiagnosisDocument2 pagesN O Name AGE SEX Vitamin D Lab Result DiagnosisDhila SafirinaNo ratings yet
- Yearsandyears KingDocument4 pagesYearsandyears KingDhila SafirinaNo ratings yet
- Yearsandyears KingDocument4 pagesYearsandyears KingDhila SafirinaNo ratings yet
- Batik (: (Bate) ʔ (Bat K) Ɪ Wax-Resist Dyeing (Antiŋ) ƮƮʂ (Ap) ƮƮʂDocument1 pageBatik (: (Bate) ʔ (Bat K) Ɪ Wax-Resist Dyeing (Antiŋ) ƮƮʂ (Ap) ƮƮʂDhila SafirinaNo ratings yet
- National Museum Marks 236th AnniversaryDocument3 pagesNational Museum Marks 236th AnniversaryDhila SafirinaNo ratings yet
- Batik (: (Bate) ʔ (Bat K) Ɪ Wax-Resist Dyeing (Antiŋ) ƮƮʂ (Ap) ƮƮʂDocument1 pageBatik (: (Bate) ʔ (Bat K) Ɪ Wax-Resist Dyeing (Antiŋ) ƮƮʂ (Ap) ƮƮʂDhila SafirinaNo ratings yet
- Hanging TreeDocument3 pagesHanging TreeDhila SafirinaNo ratings yet
- The Wicked TowerDocument78 pagesThe Wicked TowerDark ShadowNo ratings yet
- AgnistomaDocument29 pagesAgnistomaArnaud DidierjeanNo ratings yet
- PORTFOLIO SHOWCASING STUDENT LESLY BULLON'S WRITINGS, SUMMARIES, AND CREATIVE WORKSDocument15 pagesPORTFOLIO SHOWCASING STUDENT LESLY BULLON'S WRITINGS, SUMMARIES, AND CREATIVE WORKSLess NuñezNo ratings yet
- Movie Script - The Lord of The Rings - The Two TowersDocument101 pagesMovie Script - The Lord of The Rings - The Two TowersMarc RitzNo ratings yet
- Surya Namaskar or 'Sun salutation': A way to happinessDocument4 pagesSurya Namaskar or 'Sun salutation': A way to happinessSummit GautamNo ratings yet
- John Rutter - Black SheepDocument4 pagesJohn Rutter - Black SheepAndoNo ratings yet
- Y2 Phonics Reading CardDocument35 pagesY2 Phonics Reading CardNorliniMohdRipinNo ratings yet
- Avsorb Forte - DairyDocument27 pagesAvsorb Forte - DairydrgsainiNo ratings yet
- Bio ExerciseDocument3 pagesBio Exerciseaina zulaikhaNo ratings yet
- Yokozawa Takafumi No Baai Vol 6Document40 pagesYokozawa Takafumi No Baai Vol 6Eruwaedhiel ArcamenelNo ratings yet
- MiletskiDocument281 pagesMiletskiCanisLupusZeta100% (2)
- Can You Guess The Title of These ExtractsDocument2 pagesCan You Guess The Title of These ExtractsHafis ZamNo ratings yet
- What Is PuppetDocument7 pagesWhat Is PuppetsylviannitaNo ratings yet
- Room On The BroomDocument31 pagesRoom On The BroomHebing WuNo ratings yet
- Full Blood Count Apr04, DR Eva RaikDocument7 pagesFull Blood Count Apr04, DR Eva RaikDanielcc LeeNo ratings yet
- Delhi Public School EVS Sample Book Chapter 1 Living and Non-Living ThingsDocument72 pagesDelhi Public School EVS Sample Book Chapter 1 Living and Non-Living ThingsPRNo ratings yet
- Super Gene - Twelve Winged Dark Burning AngeDocument15,541 pagesSuper Gene - Twelve Winged Dark Burning AngeIchchhit SinghNo ratings yet
- Cryptic Film TitlesDocument2 pagesCryptic Film TitlesChay HallNo ratings yet
- Parasitology TableDocument9 pagesParasitology TablehumanupgradeNo ratings yet
- Management of Tinea Capitis in ChildhoodDocument26 pagesManagement of Tinea Capitis in ChildhoodSandra aneeNo ratings yet
- 03 16Document104 pages03 16WoodsNo ratings yet
- Lion or SheepDocument1 pageLion or SheepPeter FalkingNo ratings yet
- Memotain: A CAD/CAM Nickel-Titanium Lingual Retainer: Clinician'S CornerDocument4 pagesMemotain: A CAD/CAM Nickel-Titanium Lingual Retainer: Clinician'S Cornerangianny_cdNo ratings yet
- Tanuki: The Badger' As Figure in Japanese: LiteratureDocument24 pagesTanuki: The Badger' As Figure in Japanese: LiteratureNicole BednarzNo ratings yet
- The Zoo Symbolform Process BookDocument13 pagesThe Zoo Symbolform Process BookJohn Andrew SalazarNo ratings yet
- An Overview of Knotting of YarnDocument4 pagesAn Overview of Knotting of YarnMohammed Atiqul Hoque ChowdhuryNo ratings yet
- Lesson 1-4 Spelling, Vocabulary and ComprehensionDocument16 pagesLesson 1-4 Spelling, Vocabulary and ComprehensionVera Hristofor - OjogNo ratings yet
- TSR 9125 - UK5 - Eye of The Serpent PDFDocument38 pagesTSR 9125 - UK5 - Eye of The Serpent PDFRobert Bailey100% (3)
- Assessment of The Lungs and ThoraxDocument21 pagesAssessment of The Lungs and ThoraxNur Rofikoh Bil Karomah100% (2)
- Rabies Control Program by DohDocument11 pagesRabies Control Program by DohSabrina Porquiado Magañan SNNo ratings yet