You might also like
- 2Document8 pages2Jaica Mangurali TumulakNo ratings yet
- 04 P001 11816Document12 pages04 P001 11816Jaica Mangurali TumulakNo ratings yet
- Generic Name, Brand, Company & Address of Olaparib tabletsDocument1 pageGeneric Name, Brand, Company & Address of Olaparib tabletsJaica Mangurali TumulakNo ratings yet
- NOTES On CDRRHRDocument8 pagesNOTES On CDRRHRJaica Mangurali TumulakNo ratings yet
- Checklist of Requirements For SPPDocument1 pageChecklist of Requirements For SPPJaica Mangurali TumulakNo ratings yet
- 9Document9 pages9Jaica Mangurali TumulakNo ratings yet
- Application for Registration of Equipment for Treating Medical WasteDocument1 pageApplication for Registration of Equipment for Treating Medical WasteShamira Yessa Lazaro EspinosaNo ratings yet
- Heneral Luna HereDocument3 pagesHeneral Luna HereJaica Mangurali TumulakNo ratings yet
- Salicylates: Common Name: Acetylsalicylic Acid IUPAC Name: 2-Acetoxybenzoic Acid Molecular Formula: C H ODocument3 pagesSalicylates: Common Name: Acetylsalicylic Acid IUPAC Name: 2-Acetoxybenzoic Acid Molecular Formula: C H OJaica Mangurali TumulakNo ratings yet
- Vitamin A FunctionsDocument2 pagesVitamin A FunctionsJaica Mangurali TumulakNo ratings yet
- 1907 50 Centavos CoinDocument2 pages1907 50 Centavos CoinJaica Mangurali TumulakNo ratings yet
- Quality Control Sample Problems in Titrimetry and GravimetryDocument17 pagesQuality Control Sample Problems in Titrimetry and GravimetryJaica Mangurali TumulakNo ratings yet
- Vitamin A FunctionsDocument2 pagesVitamin A FunctionsJaica Mangurali TumulakNo ratings yet
- Vitamin A FunctionsDocument2 pagesVitamin A FunctionsJaica Mangurali TumulakNo ratings yet
- 2015 DyslipidemiaDocument22 pages2015 DyslipidemiaHannah LeiNo ratings yet
- 2015 Loose Tabelets and Capsules IdentifierDocument5 pages2015 Loose Tabelets and Capsules IdentifierJaica Mangurali TumulakNo ratings yet
- Vitamin A FunctionsDocument2 pagesVitamin A FunctionsJaica Mangurali TumulakNo ratings yet
- Precolonial PhilippinesDocument38 pagesPrecolonial PhilippinesJaica Mangurali TumulakNo ratings yet
- Template For Paper Critique ActivityDocument4 pagesTemplate For Paper Critique ActivityJaica Mangurali TumulakNo ratings yet
- PresDocument3 pagesPresJaica Mangurali TumulakNo ratings yet
- Hemostasis and Thrombosis DrugsDocument30 pagesHemostasis and Thrombosis DrugsJaica Mangurali TumulakNo ratings yet
- Physics #2Document1 pagePhysics #2Jaica Mangurali TumulakNo ratings yet
- Administrative Order No. 55, SDocument4 pagesAdministrative Order No. 55, SJaica Mangurali TumulakNo ratings yet
- Exercise 2Document2 pagesExercise 2Jaica Mangurali TumulakNo ratings yet
- Cholera El TorDocument5 pagesCholera El TorJaica Mangurali TumulakNo ratings yet
- Rev. Fr. Rolando M. Castro: Vice Rector For FinanceDocument1 pageRev. Fr. Rolando M. Castro: Vice Rector For FinanceJaica Mangurali TumulakNo ratings yet
- Resistors Series Parallel CircuitsDocument6 pagesResistors Series Parallel CircuitsJaica Mangurali TumulakNo ratings yet
- Cover StoryDocument1 pageCover StoryJaica Mangurali TumulakNo ratings yet
- To Be A "Makabayan": The Essence of NSTP For MeDocument2 pagesTo Be A "Makabayan": The Essence of NSTP For MeJaica Mangurali TumulakNo ratings yet
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- VNACS Final Case ReportDocument9 pagesVNACS Final Case ReportVikram Singh TomarNo ratings yet
- ReadingDocument6 pagesReadingakhyar sanchiaNo ratings yet
- The English Center Articulation AgreementDocument9 pagesThe English Center Articulation AgreementJose CabreraNo ratings yet
- ADD MATH ProjectDocument13 pagesADD MATH Projectmegazat27No ratings yet
- Megneto TherapyDocument15 pagesMegneto TherapyedcanalNo ratings yet
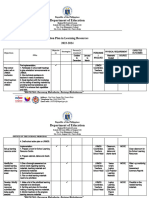
- aCTION PLAN IN HEALTHDocument13 pagesaCTION PLAN IN HEALTHCATHERINE FAJARDONo ratings yet
- List of Psychotropic Drugs Under International ControlDocument32 pagesList of Psychotropic Drugs Under International ControlRadhakrishana DuddellaNo ratings yet
- Ballari City Corporation: Government of KarnatakaDocument37 pagesBallari City Corporation: Government of KarnatakaManish HbNo ratings yet
- ACCA P1 Governance, Risk, and Ethics - Revision QuestionsDocument2 pagesACCA P1 Governance, Risk, and Ethics - Revision QuestionsChan Tsu ChongNo ratings yet
- Applying Graph Theory to Map ColoringDocument25 pagesApplying Graph Theory to Map ColoringAnonymous BOreSFNo ratings yet
- Chapter 3-The Hospitality & Travel Marketing SystemDocument14 pagesChapter 3-The Hospitality & Travel Marketing SystemCharis AbadNo ratings yet
- Keb Combivis 6 enDocument232 pagesKeb Combivis 6 enhaithamNo ratings yet
- How To Retract BPS Data Back To R3 When There Is No Standard RetractorDocument3 pagesHow To Retract BPS Data Back To R3 When There Is No Standard Retractorraphavega2010No ratings yet
- CSIR AnalysisDocument1 pageCSIR Analysisசெபா செல்வாNo ratings yet
- Ted Hughes's Crow - An Alternative Theological ParadigmDocument16 pagesTed Hughes's Crow - An Alternative Theological Paradigmsa46851No ratings yet
- RPH Sains DLP Y3 2018Document29 pagesRPH Sains DLP Y3 2018Sukhveer Kaur0% (1)
- Interviews: Personal Interview. Advantages and Disadvantages Business Is Largely A Social PhenomenonDocument8 pagesInterviews: Personal Interview. Advantages and Disadvantages Business Is Largely A Social PhenomenonSanjeev JayaratnaNo ratings yet
- Lecture-3 Sources of Bioelectric PotentialDocument13 pagesLecture-3 Sources of Bioelectric PotentialMurali krishnan.MNo ratings yet
- C ProgrammingDocument205 pagesC ProgrammingSrinivasan RamachandranNo ratings yet
- Name: Chakshu Purohit Course: BBA LLB Subject: Legal Research and Methodology Submitted To: Utkarsh MishraDocument5 pagesName: Chakshu Purohit Course: BBA LLB Subject: Legal Research and Methodology Submitted To: Utkarsh Mishrachakshu purohitNo ratings yet
- MT8820C LTE Measurement GuideDocument136 pagesMT8820C LTE Measurement GuideMuthannaNo ratings yet
- Case Study (DM)Document28 pagesCase Study (DM)Jai - Ho100% (1)
- Jt20 ManualDocument201 pagesJt20 Manualweider11No ratings yet
- Organic Evolution (Evolutionary Biology) Revised Updated Ed by Veer Bala RastogiDocument1,212 pagesOrganic Evolution (Evolutionary Biology) Revised Updated Ed by Veer Bala RastogiTATHAGATA OJHA83% (6)
- A-00 IndexDocument10 pagesA-00 IndexNizarHamrouniNo ratings yet
- MAS Assessment Exam Answer Key SolutionDocument7 pagesMAS Assessment Exam Answer Key SolutionJonalyn JavierNo ratings yet
- 8510C - 15, - 50, - 100 Piezoresistive Pressure Transducer: Features DescriptionDocument3 pages8510C - 15, - 50, - 100 Piezoresistive Pressure Transducer: Features Descriptionedward3600No ratings yet
- DMGT403 Accounting For Managers PDFDocument305 pagesDMGT403 Accounting For Managers PDFpooja100% (1)
- Living in a digital age unit review and digital toolsDocument1 pageLiving in a digital age unit review and digital toolsLulaNo ratings yet
- TheSun 2008-11-04 Page16 Asian Stocks Rally Continues On Policy HopesDocument1 pageTheSun 2008-11-04 Page16 Asian Stocks Rally Continues On Policy HopesImpulsive collectorNo ratings yet