You might also like
- Shoulder DislocationDocument6 pagesShoulder DislocationRizki IrwansyahNo ratings yet
- APJCP - Volume 16 - Issue 18 - Pages 8141-8143 PDFDocument3 pagesAPJCP - Volume 16 - Issue 18 - Pages 8141-8143 PDFRizki IrwansyahNo ratings yet
- Helicobacter A Paradigm ShiftDocument20 pagesHelicobacter A Paradigm ShiftRizki IrwansyahNo ratings yet
- The Elements of Fracture Fixation 2nd EdDocument13 pagesThe Elements of Fracture Fixation 2nd EdRizki Irwansyah0% (2)
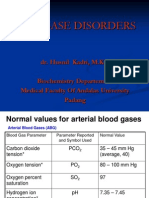
- Acid Base DisordersDocument28 pagesAcid Base DisordersRizki IrwansyahNo ratings yet
- DSTC LDocument465 pagesDSTC LRizki Irwansyah100% (2)
- The Evaluation of The Validity of Alvarado, Eskelinen, Lintula, Ohmann ScoreDocument5 pagesThe Evaluation of The Validity of Alvarado, Eskelinen, Lintula, Ohmann ScoreRizki IrwansyahNo ratings yet
- Worksheets EBMDocument19 pagesWorksheets EBMRizki IrwansyahNo ratings yet
- CT ScanDocument4 pagesCT ScanRizki IrwansyahNo ratings yet
- Red Eye DDDocument33 pagesRed Eye DDRizki IrwansyahNo ratings yet
- The One That Got AwayDocument5 pagesThe One That Got AwayRizki Irwansyah100% (1)
- Jay Sean-Down Piano CoverDocument9 pagesJay Sean-Down Piano CoverJun Hao HengNo ratings yet
- List Top GameDocument1 pageList Top GameRizki IrwansyahNo ratings yet
- Vaginal Birth After Cesarean: New Insights: Evidence Report/Technology AssessmentDocument397 pagesVaginal Birth After Cesarean: New Insights: Evidence Report/Technology AssessmentRizki IrwansyahNo ratings yet
- Hypertension and PregnancyDocument1 pageHypertension and PregnancyRizki IrwansyahNo ratings yet
- Jay Sean - TonightDocument3 pagesJay Sean - TonightRizki IrwansyahNo ratings yet
- Body Surface AreaDocument2 pagesBody Surface AreaRizki IrwansyahNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5784)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (72)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- First Aid Exam BDocument13 pagesFirst Aid Exam BDenise Barber100% (5)
- ImplantDocument4 pagesImplantMohamed KudaihNo ratings yet
- M4164-C 06-15 - Etrinsa Technical Manual - MN031r2hq PDFDocument142 pagesM4164-C 06-15 - Etrinsa Technical Manual - MN031r2hq PDFMaria Lavinia IordacheNo ratings yet
- MYOPIA REDUCTION... A View from the InsideDocument6 pagesMYOPIA REDUCTION... A View from the InsidePierre RodulfoNo ratings yet
- Testimonial Theatre-Making: Establishing or Dissociating The SelfDocument9 pagesTestimonial Theatre-Making: Establishing or Dissociating The SelfLucretia DespinoiuNo ratings yet
- Perioperative Nursing Care PhasesDocument5 pagesPerioperative Nursing Care PhasesanjieNo ratings yet
- Jurnal AnemiaDocument4 pagesJurnal AnemiaAchmad Aidil TazakkaNo ratings yet
- Comparative Effects of Pulsed and Continuous Short Wave Diathermy On Pain and Selected Physiological Parameters Among Subjects With Chronic Knee OsteoarthritisDocument10 pagesComparative Effects of Pulsed and Continuous Short Wave Diathermy On Pain and Selected Physiological Parameters Among Subjects With Chronic Knee Osteoarthritisjansen irawanNo ratings yet
- Clin Exp RheumatolDocument1 pageClin Exp RheumatolAstridNo ratings yet
- Resumen Pediatria 2Document77 pagesResumen Pediatria 2Chris Ledezma JorqueraNo ratings yet
- INTUSSUSCEPTIONDocument3 pagesINTUSSUSCEPTIONS GNo ratings yet
- Tetracycline HCl study drugDocument4 pagesTetracycline HCl study drugCheezy BreadNo ratings yet
- Outpatient Medicine Reimbursement Form - 002 PJVDocument4 pagesOutpatient Medicine Reimbursement Form - 002 PJVPJ ValenciaNo ratings yet
- HIV AIDS Workplace Policy & ProgramDocument4 pagesHIV AIDS Workplace Policy & ProgramMFB POTTERY67% (3)
- Soap Note Template 33Document3 pagesSoap Note Template 33Rafael G. Garcia SanchezNo ratings yet
- Etiologies and Medical AspectsDocument2 pagesEtiologies and Medical AspectsAnastasia Lincoln GreyNo ratings yet
- BSSP Course DescriptionsDocument3 pagesBSSP Course DescriptionsJilliane LagusNo ratings yet
- Importance of avoiding eight factors during and after Panchakarma therapyDocument2 pagesImportance of avoiding eight factors during and after Panchakarma therapy21 RakshitNo ratings yet
- 10 1 1 947 3241Document8 pages10 1 1 947 3241Mayur MulyeNo ratings yet
- Intro CBTDocument12 pagesIntro CBTAria LevinsNo ratings yet
- Symptom Distress Scale User ManualDocument99 pagesSymptom Distress Scale User ManualLivianty HukubunNo ratings yet
- Drug Interactions in Psychiatry, 3rdDocument454 pagesDrug Interactions in Psychiatry, 3rdKhaled AbdelNaserNo ratings yet
- Drug Study Amphotericin B, Meropenem, Furosemide, Ciprofloxacin, Pentoxifylline, Pip-Tazo, Midazolam, VecuroniumDocument12 pagesDrug Study Amphotericin B, Meropenem, Furosemide, Ciprofloxacin, Pentoxifylline, Pip-Tazo, Midazolam, Vecuroniumpaupaulala100% (4)
- Plumbing Questionnaire 2Document51 pagesPlumbing Questionnaire 2mcpayod100% (1)
- Balanced Diet: Includes Foods From All Food Groups During The DayDocument19 pagesBalanced Diet: Includes Foods From All Food Groups During The DayMayuri VohraNo ratings yet
- Unit 1: Consumer HealthDocument23 pagesUnit 1: Consumer HealthGriffin AndersonNo ratings yet
- An Update On The Management of Endometrial HyperplasiaDocument5 pagesAn Update On The Management of Endometrial Hyperplasiafitrah fajrianiNo ratings yet
- Tissue RepairDocument9 pagesTissue RepairSakidu LegionNo ratings yet
- Nimesulide ODTDocument10 pagesNimesulide ODTMihai SebastianNo ratings yet
- Research ProposalDocument6 pagesResearch Proposalapi-355503275No ratings yet